


Heart failure is a disorder in which the heart is unable to keep up with the demands of the body, leading to reduced blood flow, back-up (congestion) of blood in the veins and lungs, and/or other changes that may further weaken or stiffen the heart.
Heart failure develops when the contracting action or the relaxing action of the heart is inadequate, typically because the heart muscle is weak, stiff, or both.
Many disorders that affect the heart can cause heart failure.
Most people have no symptoms at first, and shortness of breath and fatigue develop gradually over days to months.
Fluid may accumulate in the lungs, abdomen, or legs.
Doctors usually suspect heart failure on the basis of symptoms, but tests, such as echocardiography (ultrasound of the heart), are usually done to evaluate heart function.
Treatment focuses on treating the disorder causing heart failure, making lifestyle changes, and treating heart failure with drugs or with surgery or other interventions.
Heart failure can occur in people of any age, even in young children (especially those born with a heart defect). However, it is much more common among older people, because older people are more likely to have disorders that predispose to heart failure (such as coronary artery disease, which damages the heart muscle), or disorders of the heart valves. Age-related changes in the heart also tend to make the heart work less efficiently.
About 6.5 million people in the United States have heart failure and about 960,000 new cases occur each year. Worldwide, about 26 million people are affected. The disorder is likely to become more common because people are living longer and because, in some countries, certain risk factors for heart disease (such as obesity, diabetes, smoking, and high blood pressure) are affecting more people.
Heart failure does not mean that the heart has stopped. It means that the heart cannot keep up with the work required to pump adequate blood to all parts of the body (its workload). However, this definition is somewhat simplistic. Heart failure is complex, and no simple definition can encompass its many causes, aspects, forms, and consequences.

The function of the heart is to pump blood. A pump moves fluid out of one place and into another. With the heart,
The right side of the heart pumps blood from the veins into the lungs
The left side of the heart pumps blood from the lungs out through the arteries to the rest of the body
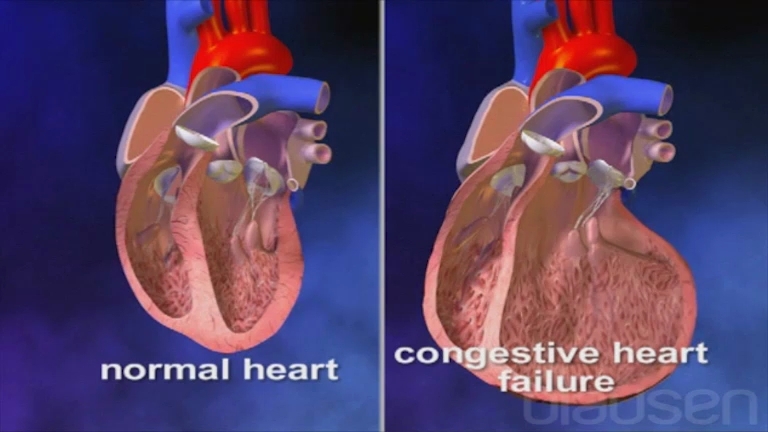
Blood goes out of the heart when the heart muscle contracts (called systole) and comes into the heart when the heart muscle relaxes (called diastole). Heart failure develops when the contracting or the relaxing action of the heart is inadequate, typically because the heart muscle is weak, stiff, or both. As a result, blood may not flow out in adequate amounts. Blood may also build up in the tissues, causing congestion. That is why heart failure is sometimes known as congestive heart failure.
Je, Ulijua...
|
Accumulation of blood coming into the left side of the heart causes congestion in the lungs, making breathing difficult. Accumulation of blood coming into the right side of the heart causes congestion and fluid accumulation in other parts of the body, such as the legs and the liver. Heart failure usually affects both the right and left sides of the heart to some degree. However, one side may be affected by disease more than the other. In such cases, heart failure may be described as right-sided heart failure or left-sided heart failure.
In heart failure, the heart may not pump enough blood to meet the body’s need for oxygen and nutrients, which are supplied by the blood. As a result, arm and leg muscles may tire more quickly, and the kidneys may not function normally. The kidneys filter fluid and waste products from the blood into the urine, but when the heart cannot pump adequately, the kidneys malfunction and cannot remove excess fluid from the blood. As a result, the amount of fluid in the bloodstream increases, and the workload of the failing heart increases, creating a vicious circle. Thus, heart failure becomes even worse.
Aina za moyo kushindwa kufanya kazi
The types of heart failure are classified by the ejection fraction (EF), which is the percentage of blood pumped out by the heart with each beat and is a measure of how well the heart is pumping. A normal left ventricle ejects about 55 to 60% of the blood in it.
In heart failure with reduced ejection fraction (HFrEF—sometimes called systolic heart failure):
The heart contracts less forcefully and pumps out a lower percentage of the blood that is returned to it. As a result, more blood remains in the heart. Blood then accumulates in the lungs, veins, or both.
In heart failure with preserved ejection fraction (HFpEF—sometimes called diastolic heart failure):
The heart is stiff and does not relax normally after contracting, which impairs its ability to fill with blood. The heart contracts normally, so it is able to pump a normal proportion of blood out of the ventricles, but the total amount pumped with each contraction may be less. Sometimes the stiff heart compensates for its poor filling by pumping out an even higher proportion of the blood than it normally does. However, eventually, as in systolic heart failure, the blood returning to the heart accumulates in the lungs or veins.
Heart failure with mildly reduced ejection fraction (HFmrEF) is a newer concept that includes people whose ejection fraction is somewhere between preserved and reduced ejection fraction.
Moyo Kushindwa Kufanya Kazi: Matatizo ya Kusukuma na Kujaza
Normally, the heart stretches as it fills with blood (during diastole), then contracts to pump out the blood (during systole). The main pumping chambers in the heart are the ventricles. Heart failure due to systolic dysfunction usually develops because the heart cannot contract normally. It may fill with blood, but the heart cannot pump out as much of the blood it contains because the muscle is weaker or because a heart valve malfunctions. As a result, the amount of blood pumped to the body and to the lungs is reduced, and the ventricle usually enlarges. Heart failure due to diastolic dysfunction develops because the heart muscle stiffens (particularly the left ventricle) and may thicken so that the heart cannot fill normally with blood. Consequently, blood backs up in the left atrium and lung (pulmonary) blood vessels and causes congestion. Nonetheless, the heart may be able to pump out a normal percentage of the blood it receives (but the total amount pumped out may be less). The heart chambers always contain some blood, but different amounts of blood may enter or leave the chambers with each heartbeat as indicated by the thickness of the arrows. |


Sababu za moyo kushindwa kufanya kazi
Doctors often divide causes of heart failure into
Disorders that directly affect the heart (cardiac causes)
Disorders of other body systems that indirectly affect the heart (non-cardiac causes)
Any disorder that directly affects the heart can lead to heart failure, as can some disorders that indirectly affect the heart. Some disorders cause heart failure quickly. Other disorders cause heart failure only after many years. Some disorders cause systolic heart failure, others cause diastolic heart failure, and some disorders, such as high blood pressure and some heart valve disorders, can cause both types of dysfunction.
Sababu za moyo vinavyofanya moyo kushindwa kufanya kazi
Cardiac disorders that cause heart failure may impair the entire heart or one area of the heart. In many cases, a combination of factors results in heart failure.
A common cardiac cause of heart failure is
Coronary artery disease can impair large areas of heart muscle because it reduces the flow of oxygen-rich blood to the heart muscle, which needs oxygen for normal contraction. Blockage of a coronary artery can cause a heart attack, which destroys an area of heart muscle. As a result, that area can no longer contract normally.
Other cardiac causes of heart failure include
Myocarditis (inflammation of heart muscle)
Some drugs (for example, some chemotherapy drugs)
Some toxins (for example, alcohol)
Heart valve disorders
An abnormal connection between heart chambers (for example, ventricular septal defect)
Disorders that affect the heart's electrical conduction system and cause an abnormal heart rhythm
Some genetic disorders
Disorders that stiffen the heart
Myocarditis (heart inflammation) caused by a bacterial, viral, or other infection can damage all or part of the heart muscle, impairing its pumping ability.
Some drugs used to treat cancer and some toxins (such as alcohol) may also damage heart muscle.
Heart valve disorders—narrowing (stenosis) of a valve, which hinders blood flow through the heart, or leakage of blood backward (regurgitation or insufficiency) through a valve—can cause heart failure. Both stenosis and regurgitation of a valve can severely stress the heart, so that over time, the heart enlarges and cannot pump adequately.
An abnormal connection (for example, ventricular septal defect) between the heart chambers can allow blood to recirculate within the heart, increasing the workload of the heart, and thus can cause heart failure.
Disorders that affect the heart’s electrical conduction system (see figure Tracing the Heart's Electrical Pathway) and cause prolonged changes in heart rhythms (especially if these are fast or irregular) can cause heart failure. When the heart beats abnormally, it cannot pump blood efficiently.
Some genetic disorders can affect the heart and cause heart failure. For example, Duchenne muscular dystrophy causes weakness of the heart muscle (along with many other muscles). Down syndrome can cause birth defects of the heart.
Heart failure may result from disorders that cause the heart’s walls to stiffen, such as infiltrations and infections. For example, in amyloidosis, amyloid, an abnormal protein passes into (infiltrates) many tissues in the body. If amyloid infiltrates the heart’s walls, they stiffen, and heart failure results. In tropical countries, infiltration of heart muscle by certain parasites (such as in Chagas disease) can cause heart failure, even in young people.
In constrictive pericarditis, the sac that envelops the heart (pericardium) stiffens, preventing even a healthy heart from pumping and filling normally.
Je, Ulijua...
|
Sababu zisizo za moyo vinavyofanya moyo kushindwa kufanya kazi
The most common non-cardiac cause of heart failure is
Inadequately treated high blood pressure
High blood pressure stresses the heart because the heart must pump blood more forcefully than normal to eject blood into the arteries against the higher pressure. Eventually, the heart’s walls thicken (hypertrophy) and/or stiffen. The stiff heart does not fill quickly or adequately, so that with each contraction, the heart pumps less blood than it normally does. Diabetes and obesity also cause changes that stiffen the walls of the ventricle.
As people age, the heart’s walls also tend to stiffen. The combination of high blood pressure, obesity, and diabetes, which are common among older people, and age-related stiffening makes heart failure particularly common among older people.
Less common non-cardiac causes of heart failure include
High blood pressure in arteries to the lungs (pulmonary hypertension, sometimes caused by pulmonary embolism)
Anemia
Thyroid gland disorders
Kidney failure
Some drugs
Some lung disorders, such as pulmonary hypertension, may alter or damage blood vessels in the lungs (pulmonary arteries). As a result, the right side of the heart has to work harder to pump blood into the lungs. The person may then develop cor pulmonale, in which the right ventricle is enlarged and there is right-sided heart failure.
Sudden, severe blockage of a pulmonary artery by one or more blood clots (pulmonary embolism) also makes pumping blood into the pulmonary arteries difficult and can cause right-sided heart failure.
Anemia is a severe deficiency of red blood cells (low blood count). Red blood cells carry oxygen from the lungs to body tissues. Anemia reduces the amount of oxygen the blood carries, so that the heart must work harder to provide the same amount of oxygen to tissues. Anemia has many causes, including heart failure itself.
An overactive thyroid gland (hyperthyroidism) overstimulates the heart, so that it pumps too rapidly and does not empty normally during each heartbeat. When the thyroid gland is underactive (hypothyroidism), all muscles, including the heart, become weak because muscles depend on thyroid hormones to function normally.
Kidney failure strains the heart because the kidneys cannot remove excess fluid from the bloodstream, so the heart has a larger volume of blood to pump. Eventually, the heart cannot keep up, and heart failure develops.
Some drugs, such as nonsteroidal anti-inflammatory drugs, may cause the body to retain fluid, which increases the workload of the heart and may precipitate heart failure.
Mbinu za Kusawazisha
The body has several mechanisms to compensate for heart failure.
Majibu ya homoni
The body’s first response to stress, including that due to heart failure, is to release the fight-or-flight hormones, epinephrine (adrenaline) and norepinephrine (noradrenaline). For example, these hormones may be released immediately after a heart attack damages the heart. Epinephrine and norepinephrine cause the heart to pump faster and more forcefully. They help the heart increase the amount of blood pumped out (cardiac output), sometimes to a normal amount, and thus initially help compensate for the heart’s impaired pumping ability.
People who do not have heart disease usually benefit from release of these hormones when more work is temporarily required of the heart. However, for people who have chronic heart failure, this sustained response increases demands on an already damaged heart. Over time, the heart stops responding as well to the hormones, and the increased demands lead to further deterioration of heart function.
Majibu ya figo
Another of the body’s main compensatory mechanisms for the reduced blood flow in heart failure is to increase the amount of salt and water retained by the kidneys. Retaining salt and water instead of excreting it into urine increases the volume of blood in the bloodstream and helps maintain blood pressure. However, the larger volume of blood also stretches the heart muscle, enlarging the heart chambers, particularly the ventricles. At first, the more the heart muscle is stretched, the more forcefully it contracts, which improves heart function. However, after a certain amount of stretching, stretching no longer helps but instead weakens the heart’s contractions (as when a rubber band is overstretched). Consequently, heart failure worsens. In addition, salt and water retention increase fluid congestion in organs such as the lungs, leading to worsening symptoms of heart failure.
Kuongezeka kwa moyo
Another important compensatory mechanism is enlargement of the muscular walls of the ventricles (ventricular hypertrophy). When the heart must work harder, the heart’s walls enlarge and thicken, as biceps muscles enlarge after months of weight training. At first, the enlargement allows the heart to maintain the amount of blood it pumps out (cardiac output). However, the enlarged and/or thickened heart eventually becomes stiff, causing or worsening heart failure. Also, the enlargement can stretch the heart valve openings, causing them to malfunction, which causes more pumping problems.
Dalili za Moyo Kushindwa Kufanya Kazi
Symptoms of heart failure may begin suddenly, especially if the cause is a heart attack. However, most people have no symptoms when the heart first begins to develop problems. Symptoms then develop gradually over days to months or years. Heart failure may stabilize for periods of time but often progresses slowly and insidiously. However, people may become aware of symptoms suddenly, as when symptoms restrict an activity for the first time or when symptoms occur while at rest.
Some common symptoms are
Fatigue
Fluid accumulation (edema) in the legs
Inability to exercise or do other activities that require exertion
In older people, heart failure sometimes causes vague symptoms such as sleepiness, confusion, and disorientation.
The severity of heart failure is usually classified based on how well the person is able to carry out activities of daily life. The New York Heart Association (NYHA) classification remains an important tool for people and their caregivers to understand the severity of the illness and its impact on their life.
Uainishaji wa Moyo Kushindwa Kufanya Kazi*
Class | Symptoms |
|---|---|
I No limitation | Ordinary physical activity does not cause undue tiredness, shortness of breath, or awareness of heartbeats (palpitations). |
II Mild | Ordinary physical activity causes tiredness, shortness of breath, palpitations, or chest discomfort (angina). |
III Moderate | The person is comfortable at rest, but ordinary physical activity causes tiredness, shortness of breath, and palpitations or chest discomfort (angina). |
IV Severe | Symptoms occur at rest, and any physical activity increases symptoms. |
* New York Heart Association classification. | |
Right-sided heart failure and left-sided heart failure cause different symptoms. Although both types of heart failure may be present, the symptoms of failure of one side often predominate. Eventually, left-sided heart failure causes right-sided failure.
Dalili za kushindwa kwa moyo wa upande wa kulia
The main symptom of right-sided heart failure is fluid accumulation, leading to swelling (edema) in the feet, ankles, legs, lower back, liver, and abdomen. Where the fluid accumulates depends on the amount of excess fluid and the effects of gravity. If a person is standing, fluid accumulates in the legs and feet. If a person is lying down, fluid usually accumulates in the lower back. If the amount of fluid is large, fluid also accumulates in the abdomen. Fluid accumulation in the liver or stomach can cause nausea, bloating, and loss of appetite. Severe right-sided heart failure can result in loss of weight and muscle. This condition is called cardiac cachexia.
Dalili za kushindwa kwa moyo wa upande wa kushoto
Left-sided heart failure leads to fluid accumulation in the lungs, which causes shortness of breath. At first, shortness of breath occurs only during exertion, but as heart failure progresses, it occurs with less and less exertion and eventually occurs even at rest. People with severe left-sided heart failure may be short of breath when lying down (a condition called orthopnea) because gravity causes more fluid to move into the lungs. Such people often wake up, gasping for breath or wheezing (a condition called paroxysmal nocturnal dyspnea). Sitting up causes some of the fluid to drain to the bottom of the lungs and makes breathing easier. People with left-sided heart failure also feel tired and weak when doing physical activities, because their muscles are not receiving enough blood.

Dalili za moyo kushindwa kufanya kazi
When heart failure is advanced, Cheyne-Stokes respiration (periodic breathing) may develop. In this unusual pattern of breathing, a person has a period of not breathing for a few seconds, and then begins to breathe progressively faster and deeper, then slower and shallower until they again briefly stop breathing and repeat the cycle over and over. Cheyne-Stokes respiration develops because blood flow to the brain is reduced and the areas of the brain that control breathing therefore do not receive enough oxygen. Cheyne-Stokes respiration is considered a form of central sleep apnea.
Obstructive sleep apnea (in which airway blockage interrupts sleep, resulting in daytime sleepiness) is a different and more common breathing disorder that can occur in people with or without heart failure. Severe obstructive sleep apnea can make heart failure worse.
Acute pulmonary edema is a sudden accumulation of a large amount of fluid in the lungs. It causes extreme difficulty breathing, rapid breathing, bluish skin, and feelings of restlessness, anxiety, and suffocation. Some people have severe spasms of the airways (bronchospasms) and wheezing. Acute pulmonary edema is a life-threatening emergency that can occur when people with heart failure develop very high blood pressure, have a heart attack, or sometimes just stop taking their heart failure drugs or eat salty food.
Blood clots can form in the heart chambers when the heart is severely damaged. The blood clots can form because blood flow within the chambers is sluggish. Clots may break loose (becoming emboli), travel through the bloodstream, and partially or completely block an artery elsewhere in the body. If a clot blocks an artery to the brain, a stroke may result.
Depression and decline in mental function are common in people with severe heart failure, particularly in older people, and require careful evaluation and treatment.
Utambuzi wa Moyo Kushindwa Kufanya Kazi
Chest x-ray
Electrocardiography (ECG)
Echocardiography and sometimes other imaging tests
Blood tests
Doctors usually suspect heart failure on the basis of symptoms alone. The diagnosis is supported by the results of a physical examination, including a weak, often rapid pulse, reduced blood pressure, abnormal heart sounds and murmurs and fluid accumulation in the lungs both heard through a stethoscope, an enlarged heart, swollen neck veins, an enlarged liver, and swelling in the abdomen or legs.
Procedures to evaluate heart function are usually done. Testing is also needed to identify the cause of heart failure.
Eksirei ya kifua
A chest x-ray can show an enlarged heart, and congested blood vessels and fluid accumulation in the lungs.
Elektrokadiografia
Electrocardiography (ECG) is almost always done to determine whether the heart rhythm is normal, whether the walls of the ventricles are thickened, and whether the person has had a heart attack.
Elektrokadografia
Echocardiography, which uses sound waves to produce an image of the heart, is one of the best procedures for evaluating heart function, including the pumping ability of the heart and the functioning of heart valves. Echocardiography can show the following:
Whether the heart walls are thickened and relax normally
Whether the valves are functioning normally
Whether contractions are normal
Whether any area of the heart is contracting abnormally
Echocardiography may help determine whether heart failure is due to systolic or diastolic dysfunction by enabling doctors to estimate the thickness and stiffness of the heart walls and the ejection fraction. The ejection fraction, an important measure of heart function, is the percentage of blood pumped out by the heart with each beat. A normal left ventricle ejects about 55 to 60% of the blood in it. If the ejection fraction is low (less than 40%), systolic heart failure is confirmed. If the ejection fraction is normal or high in a person who has symptoms of heart failure, diastolic heart failure is likely.
Vipimo vya damu
Blood tests are almost always done. Doctors frequently measure natriuretic peptides (NPs). NPs are substances that accumulate in the blood when heart failure is present but less often when other disorders that cause shortness of breath are present. Other blood tests may be done to look for disorders that may be causing heart failure.
Vipimo vingine
Other procedures, such as radionuclide imaging, magnetic resonance imaging (MRI), computed tomography, cardiac catheterization with angiography, and exercise (stress) testing may be done to identify the presence or cause of heart failure.
Rarely, a biopsy of heart muscle is needed, usually when doctors suspect infiltration of the heart (as occurs in amyloidosis) or myocarditis due to a bacterial, viral, or other infection.
Uzuiaji wa Moyo Kushindwa Kufanya Kazi
Preventing heart failure involves treating disorders that can cause heart failure before they lead to heart failure. Disorders that can be treated include the following:
High blood pressure
Obesity
Obstructive sleep apnea
Blockage of a coronary artery
Heart valve disorders
Some abnormal heart rhythms
Alcoholism
Anemia
Thyroid disorders
Matibabu ya Moyo Kushindwa Kufanya Kazi
Diet and lifestyle changes
Treatment of the cause of heart failure
Drugs
Sometimes an implantable cardioverter-defibrillator, cardiac resynchronization therapy, or mechanical circulatory support
Sometimes heart transplantation
Treatment of heart failure requires several general measures, along with treatment of the disorder causing heart failure, lifestyle changes, and drugs for heart failure.
Hatua za jumla
Although for most people heart failure is a chronic disorder, much can be done to make physical activity more comfortable, improve the quality of life, minimize the risk of sudden worsening (acute heart failure), and prolong life. Affected people and their family members should learn all they can about heart failure because much care occurs at home. In particular, they should know how to recognize the early warning symptoms of worsening heart failure and should be aware of the actions they need to take (for example, reduce salt intake, take an extra dose of a diuretic, or contact their doctor).
Regular communication with health care practitioners and examinations by doctors are critical because heart failure can worsen suddenly. For example, nurses may regularly call people who have heart failure to ask about changes in weight and in symptoms. Thus, they can gauge whether people need to see a doctor.
People may also go to specialized heart failure clinics. These clinics have doctors with expertise in heart failure who work closely with specially trained nurses and other health care practitioners, such as pharmacists, dietitians, and social workers, to care for people with heart failure by teaching self-care skills to people and their caregivers. These clinics can also help decrease symptoms, reduce hospitalizations, and improve life expectancy by making sure that people receive the most effective treatments and by teaching people how to fully participate in their care. This care complements rather than replaces care provided by primary care doctors.
People with heart failure should always check with their doctor before taking a new drug, even a nonprescription drug. Some drugs (including many used to treat arthritis) can cause salt and fluid retention. Other drugs may make the heart function less efficiently. Forgetting to take necessary drugs is a common cause of worsening symptoms, and people should be given ways to remind themselves to take their drugs.
Because influenza can cause a sudden worsening of a person's heart failure, doctors recommend a yearly influenza vaccination for people with heart failure. Vaccination against COVID-19 is also recommended.
Je, Ulijua...
|
Matibabu ya kisababishi
For example, if the cause of heart failure is a narrowed or leaking heart valve or an abnormal connection between heart chambers, surgery can often correct the problem. Blockage of a coronary artery may require treatment with drugs, surgery, or angioplasty with a coronary stent. Antihypertensive drugs can reduce and control high blood pressure. Antibiotics can eliminate some infections.
Hali za mtindo wa maisha
Changes in lifestyle can help people with heart failure feel and function better.
People who have heart failure should stay as physically fit as possible, even if they cannot exercise vigorously. People who have mild heart failure should follow an exercise program as prescribed by a doctor. People with more severe heart failure may need to exercise in a cardiovascular rehabilitation facility under the supervision of a trained attendant.
If people with heart failure are overweight, the heart has to work harder during activity, worsening heart failure. Such people should follow a healthy weight loss diet to attain and maintain ideal weight.
Smoking damages blood vessels. Large amounts of alcohol can act as a direct toxin to the heart. Thus, smoking and drinking alcohol can worsen heart failure and should be stopped or at least minimized.
Excess salt (sodium) in the diet can cause fluid retention, which counteracts drugs given to increase the excretion of water (such as diuretics) and relieve fluid accumulation. Thus, consuming excess salt worsens symptoms. Almost all people with heart failure should limit their intake of table salt and salty foods and their use of salt in cooking. The sodium content of packaged foods can be determined by reading the label. People with severe heart failure are usually given detailed information about how to limit salt intake. Instruction by a dietitian can be helpful. People who limit their salt intake can usually consume a normal amount of water unless fluid retention is severe. Drinking extra amounts of water is not recommended.
A simple, reliable way to check whether the body is retaining fluid is to check body weight daily. Doctors often ask people with heart failure to weigh themselves as accurately as possible every day, typically once in the morning, after they arise and urinate and before they eat breakfast. Trends are easier to spot when people weigh themselves at the same time every day, use the same scale, wear a similar amount of clothing, and keep a written record of their daily weight. Increases of more than 2 pounds (about 1 kilogram) per day are early warning signs of fluid retention. A consistent, rapid weight gain (such as 2 pounds per day) is a clue that heart failure is worsening.
Many people who limit their salt intake still have swelling. Swollen legs should be kept elevated on a stool when sitting. This position helps the body reabsorb and eliminate the excess fluid. Some people also need to wear full-length supportive stockings that help prevent accumulation of fluid. If fluid accumulates in the lungs, sleeping with several pillows or elevating the head of the bed makes sleeping easier.
Dawa za moyo kushindwa kufanya kazi
Drug treatment of heart failure involves
Drugs to help relieve symptoms: Diuretics, nitrates, or digoxin
Drugs to help improve survival: Angiotensin-converting enzyme (ACE) inhibitors, beta-blockers, aldosterone antagonists, angiotensin II receptor blockers (ARBs), angiotensin receptor/neprilysin inhibitors (ARNIs), sodium-glucose cotransporter-2 inhibitors (SGLT2s), sinus node inhibitors
For details on the specific drugs and classes, see Drug Treatment of Heart Failure.
The type of drug used depends on the type of heart failure. In systolic heart failure (HFrEF), all drug classes are helpful. In diastolic heart failure (HFpEF), only ACE inhibitors, ARBs, aldosterone antagonists and beta-blockers are typically used. In HFmrEF, ARNIs may be helpful.
It is important for people to take their drugs regularly and be sure not to let the prescription run out.
Sababu zingine
People with pulmonary edema require oxygen, which is sometimes given by special masks. Occasionally, a tube may be inserted into the airway so that a mechanical ventilator can help with the increased work of breathing.
Sometimes doctors implant a small monitoring device in the chest of people with severe heart failure The monitor continuously measures the pressures in their lungs, which can help their doctor make adjustments to their drugs. The device is especially useful in people with recurrent episodes of heart failure and coexisting kidney failure.
Heart transplantation may be an option for people who have very severe, worsening heart failure and who have not responded to drug therapy.
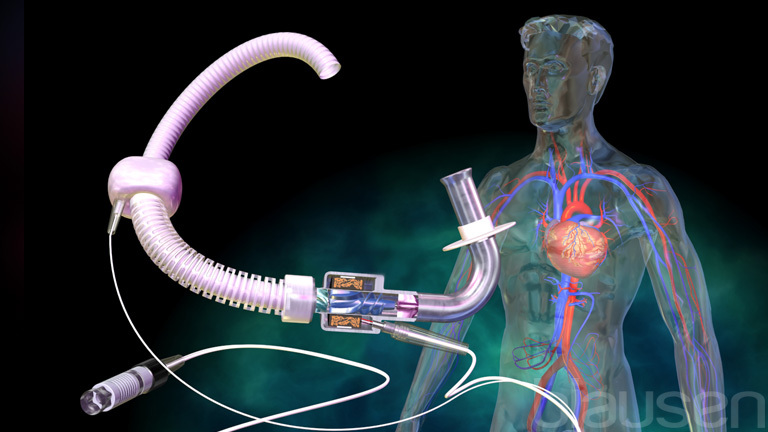
Mechanical devices that help pump blood are used for certain people with very severe heart failure that is not responding to drug therapy. Types of devices include
Intra-aortic counterpulsation balloon pump (IABP, also sometimes just called a balloon pump): A sausage-shaped balloon on the end of a catheter is placed in the aorta. A machine monitors the heart beat and inflates the balloon when the heart relaxes and deflates it when the heart contracts, which makes it easier for the heart to pump blood.
Ventricular assist devices: Different mechanical pumps can be implanted in or near the left or right ventricle to help the heart pump blood.
Intravascular assist devices: Small pumps can be implanted within large vessels such as the aorta to help pump blood.
Extracorporeal membrane oxygenation (ECMO): A device similar to a heart-lung bypass machine takes blood from a large artery and pumps it past a membrane that allows oxygen into the blood and then pumps it back into a large vein.


Heart rhythm problems can sometimes be helped with drugs, but some people require a pacemaker. Special pacemakers with two or three wires can restore the normal sequence of heart chamber contractions (cardiac resynchronization therapy) and improve outcome in some people with heart failure. Doctors may consider an implantable cardioverter-defibrillator in people with very poor heart function because their risk of sudden death is increased.
If heart failure is caused by a problem with a heart valve, doctors may repair or replace the valve.
Matibabu ya moyo kushindwa kufanya kazi kwa ghafla
Heart failure that develops or worsens quickly requires emergency treatment in a hospital.
If acute pulmonary edema (rapid accumulation of fluid in the lungs) develops, oxygen is given through a face mask. Diuretics given intravenously and other drugs such as nitroglycerin given intravenously or under the tongue can give rapid, dramatic improvement. Morphine relieves the anxiety that usually accompanies acute pulmonary edema but it also decreases the rate of breathing and is no longer used as often. If these measures do not adequately improve breathing, a specialized mask to deliver oxygen at controlled pressures may be used or a tube may be inserted into the person’s airway so that a mechanical ventilator can assist breathing.


For people who have severe symptoms and have not responded well to treatments, drugs that are similar to epinephrine and norepinephrine (such as dopamine or dobutamine) or other drugs that make cardiac muscle contract more forcefully (such as milrinone) are sometimes used for a short time to enhance the pumping function of the heart. These drugs are not useful for long-term treatment.
Masuala ya mwisho wa uhai
Life expectancy depends on many factors, including how severe the heart failure is, whether its cause can be corrected, and which treatment is used. However, once people have needed to be hospitalized for heart failure, only about 1 in 3 live another 5 years. About half of those who have severe heart failure live at least 2 years. Life expectancy does improve with treatment.
Eventually, for a person whose heart failure has been present for some time, quality of life deteriorates and the possibilities for further treatment may become limited, especially for an older person for whom heart transplantation may not be feasible. Keeping the person comfortable may eventually become more important than trying to prolong life. The person and the family members should be involved in these decisions. In fact, many studies show that people with severe heart failure and their families want to discuss these issues and that doing so does not cause undue distress. Much can be done to provide compassionate care, relieve symptoms, and maintain the person’s dignity (see Death and Dying).
Heart failure can cause death suddenly and unexpectedly, without symptoms worsening. Consequently, when possible, people who have heart failure should prepare advance directives about the type of care desired in case they are no longer able to make decisions about their care. Also, making or updating a will is important.
Taarifa Zaidi
The following English-language resource may be useful. Please note that THE MANUAL is not responsible for the content of this resource.
American Heart Association: Provides resources and information for people living with heart failure and their families


