



- Muhtasari wa Hitilafu za Moyo
- Mgawanyiko usio Kamili wa Mishipa Kubwa
- Stenosisi ya Vali ya Mkole katika Watoto
- Kasoro ya Septamu ya Atiria na Ventrikali
- Kasoro za Utando wa Atrioventricular
- Vali ya Aota yenye Sehemu Mbili
- Kubana kwa Aota
- Uhamisho Uliosahihishwa wa Kuzaliwa wa Mishipa Kubwa
- Ventrikali ya Kulia ya Kutoa Mara Mbili
- Kasoro ya Ebstein
- Ugonjwa wa Upande wa Kushoto wa Moyo wa Haipoplastiki
- Daktasi ya Ateriosasi Iliyo wazi
- Truncus Arteriosus inayoendelea
- Stenosisi ya Vali za Mapafu katika Watoto
- Tetralojia ya Fallot
- Jumla ya Kurudi kwa Mshipa wa Mapafu (TAPVR)
- Uhamisho wa Mishipa Kubwa
- Hitilafu Zingine za Moyo za kuzaliwa Nazo
Nyenzo za Mada


About one in 100 babies is born with a heart defect. Some are severe, but many are not. Defects may involve abnormal formation of the heart's walls or valves or of the blood vessels that enter or leave the heart.
Symptoms of heart birth defects vary with age. Infants may have labored or rapid breathing, poor feeding, sweating or increased breathing rate while feeding, bluish discoloration (cyanosis) of the lips or skin, unusual irritability, or failure to gain weight. Toddlers may tire easily during activity or have a rapid heart beat. Older children and adolescents may have decreased activity tolerance, chest pain during activity, awareness of heartbeats (palpitations), dizziness, or fainting.
During examination, a doctor may notice abnormal skin color, abnormal pulsations of the left side of the chest, a heart murmur or other abnormal sounds, a rapid heart beat, rapid or labored breathing, weak pulses, and/or a large liver.
Echocardiography (ultrasonography of the heart) helps identify almost all heart defects.
Treatment includes open-heart surgery for severe defects, use of a catheter with a balloon at its tip to open or widen valves or blood vessels, use of a device placed by catheter to close certain holes or extra blood vessels, or medications.
The most common birth defect of the heart is a bicuspid aortic valve. The aortic valve is the valve that opens with each heartbeat to allow blood to flow from the heart to the body. A normal aortic valve has three cusps, or leaflets. When the valve is bicuspid, it has only two cusps instead of three. Bicuspid aortic valve usually does not cause problems in infancy or childhood so it may not be diagnosed until people become adults. The most common heart defects that are diagnosed in infancy and childhood are atrial and ventricular septal defects (holes between the chambers of the heart).
Je, Ulijua...
|
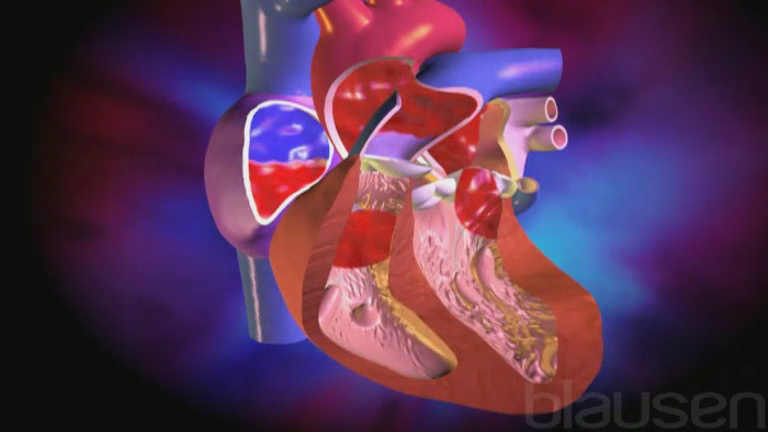
Anatomia ya Moyo
The heart is divided into two sides (right and left), and each side is divided into two chambers (an atrium and a ventricle). The atria and ventricles on both sides are separated from each other by valves.
On the right side of the heart
Blood enters from the vena cava (the largest vein in the body) and flows into the right atrium
Then flows through the tricuspid valve into the right ventricle
Then flows out of the heart through the pulmonary valve and into the pulmonary artery
The pulmonary artery delivers blood to the lungs (where the blood picks up oxygen and gets rid of carbon dioxide)
On the left side of the heart
Oxygen-rich blood enters from the pulmonary vein and flows into the left atrium
Then flows through the mitral valve into the left ventricle
Then flows out of the heart through the aortic valve and into the aorta (the largest artery in the body)
Blood circulates through the body, first through arteries, then through veins, and then through the vena cava (and back to the heart)
(See also A Look Into the Heart and Overview of the Heart and Blood Vessels.)
Mzunguko wa Kawaida wa Damu Kwenye Kijusi
Blood flow is different in the fetus than in children and adults.
In children and adults, all blood returning to the heart from the body (blue blood from the veins, which is low in oxygen) goes through the right atrium and then through the right ventricle to the pulmonary artery, and from there it enters the lungs. In the lungs, the blood picks up oxygen from the air sacs (alveoli) of the lungs and also releases carbon dioxide (see Exchanging Oxygen and Carbon Dioxide). This blood, which is rich in oxygen and appears red, returns from the lungs to the left atrium and left ventricle, and from there it is pumped out of the heart to the body through a large artery called the aorta and then through smaller arteries.
In the fetus, the path by which blood circulates through the heart and lungs is different. Because the fetus is inside the uterus, it is not exposed to air, and its lungs are collapsed and filled with amniotic fluid (the fluid inside the uterus during pregnancy). Because the fetus does not breathe air while in the uterus, the fetus' blood gets oxygen through the placenta. The mother's oxygen-rich blood flows through the blood vessels of the uterus. The mother's blood does not flow directly to the fetus. Only the oxygen in the mother's blood transfers to the fetal blood in the placenta, which then passes to the fetus through the umbilical blood vessels (in the umbilical cord).
Before birth, much of the blood from the veins (venous blood) coming to the right side of the heart bypasses the nonfunctioning lungs and travels through two short-cuts (shunts) to get to the fetus' body. These short-cuts are
The foramen ovale, a hole between the two upper chambers of the heart, the right atrium and the left atrium
The ductus arteriosus, a blood vessel connecting the two great arteries leaving the heart, the pulmonary artery and the aorta

In the fetus, venous blood arriving at the heart has received oxygen from the placenta. This oxygenated blood can be delivered to the body through the foramen ovale and the ductus arteriosus, largely bypassing the nonfunctioning lungs. This circulation pattern changes immediately after birth. During passage through the birth canal, fluid is squeezed out of the newborn's lungs. With the newborn's first breath, the lungs fill with air, which brings in oxygen. When the umbilical cord is cut, the placenta (and therefore the mother's circulation) is no longer connected to the newborn's circulation, and all the newborn's oxygen comes through the lungs. Thus, the foramen ovale and ductus arteriosus are no longer needed, and they usually close within the first days to weeks of life, making the newborn's circulation the same as that of an adult. Sometimes, the foramen ovale does not close (called patent foramen ovale), but a patent foramen ovale does not usually cause any health problems.
Mzunguko wa Kawaida wa Damu Kwenye Kijusi
Blood flow through the heart in a fetus differs from that in children and adults. In children and adults, blood picks up oxygen in the lungs. The fetus is not exposed to air. It is inside the uterus, and its lungs are collapsed and filled with amniotic fluid. Because the fetus does not breathe air, the fetus' blood gets oxygen that passes from the mother's blood vessels to the placenta. The oxygen-rich fetal blood in the placenta passes through the umbilical blood vessels (in the umbilical cord) and enters the fetal heart. Only a small amount of blood goes through the lungs. The rest of the blood bypasses the lungs by flowing through two short-cuts (shunts):
Normally, these two short-cuts close soon after birth. The red arrows represent blood that has the highest amount of oxygen. The blue arrows represent blood that has the lowest amount of oxygen. The purple arrows represent blood that has an intermediate amount of oxygen. |


Aina za Hitilafu za Moyo
The ways that heart defects cause changes in the normal blood flow to the lungs and body are
Shunting the flow of blood (blood flows through openings that are not part of the normal circulation)
Re-routing the flow of blood (blood flows through vessels that are arranged differently from the normal circulation)
Blocking the flow of blood, as occurs when a heart valve or blood vessel is defective
Uzuiaji wa mtiririko wa damu
Shunting is usually classified as
Right-to-left
Left-to-right
Right-to-left shunting involves mixing of the oxygen-poor blood from the right side of the heart with the oxygen-rich blood in the left side of the heart that is pumped to the body tissues. The more oxygen-poor blood (which is blue) that flows to the body, the bluer the body appears, particularly the lips, tongue, skin, and nail beds. Many heart defects are characterized by a bluish discoloration of the skin (called cyanosis). Cyanosis indicates that not enough oxygen-rich blood is reaching the tissues where it is needed. Many different types of birth defects of the heart can cause right-to-left shunting and thus cyanosis, but one of the most common is tetralogy of Fallot.
Left-to-right shunting involves oxygen-rich blood, which is pumped under high pressures from the left side of the heart, mixing with oxygen-poor blood being pumped from the right side of the heart through the pulmonary artery to the lungs. Left-to-right shunting makes the circulation inefficient and increases the amount of blood flowing to the lungs, which sometimes also causes high pressure in the pulmonary artery. Over time, high flow and high pressure can damage the blood vessels of the lungs and overwork both the left and right sides of the heart, causing the heart muscle to become weak and not function (heart failure—see figure Heart Failure: Pumping and Filling Problems). Examples of disorders in which left-to-right shunting occurs are ventricular septal defects, atrial septal defects, patent ductus arteriosis, and atrioventricular septal defects.
Kubadilisha njia ya mtiririko wa damu
In transposition of the great arteries, the normal connections of the aorta and the pulmonary artery to the heart are reversed. The aorta, which supplies the body, connects to the right ventricle instead of the left ventricle, and the pulmonary artery, which supplies the lungs, connects to the left ventricle instead of the right ventricle. As a result, oxygen-poor blood is circulated to the body, and oxygen-rich blood is circulated between the lungs and the heart and not the rest of the body. The body does not get enough oxygen, and severe cyanosis occurs within minutes of birth.
Mtiririko wa damu uliozuiwa
Blockages may develop in the valves of the heart or in the blood vessels leading away from the heart. Blood may be impeded from flowing
To the lungs because of narrowing of the pulmonic valve (pulmonic valve stenosis) or narrowing within the pulmonary artery itself (pulmonary artery stenosis)
Through the aorta to the body because of narrowing of the aortic valve (aortic valve stenosis) or blockage within the aorta itself (coarctation of the aorta)
Into the heart because of narrowing of the tricuspid valve (on the right side of the heart) or the mitral valve (on the left side of the heart)
Blockage of blood flow can lead to heart failure. Heart failure does not mean that the heart has stopped beating and is not the same as a heart attack. Heart failure means that the heart is unable to pump blood normally. As a result, blood from the left side of the heart may back up into the lungs and blood from the right side may back up into the body causing enlargement of the liver or swelling of the legs. Heart failure can also develop when the heart pumps too weakly (for example, when a baby is born with a weak heart muscle).
Sababu za Hitilafu za Moyo
Both environmental and genetic factors contribute to the development of birth defects of the heart.
Environmental factors include certain disorders the mother has or develops during pregnancy and some medications she has taken. Disorders that may increase the risk of an infant having a birth defect of the heart include diabetes, rubella, and systemic lupus erythematosus. Certain medications, including lithium, isotretinoin, and antiseizure medications, also increase the risk.
Genetic factors that are strongly associated with birth defects of the heart include certain chromosome abnormalities, particularly Down syndrome, trisomy 13, trisomy 18, and Turner syndrome. Other genetic disorders, such as DiGeorge syndrome, Marfan syndrome, Williams syndrome, and Noonan syndrome may cause birth defects that affect several organs, including the heart. Women over 35 years of age are at higher risk of having chromosomal abnormalities in the fetus. Even without a chromosomal abnormality, older maternal age appears to be a separate risk factor for heart birth defects. Older age of fathers may also contribute to birth defects of the heart.
When a family has had one child with a heart defect, the risk of a heart birth defect occurring in a subsequent pregnancy depends on the type of heart defect and whether there is a specific chromosome abnormality. Adults who were born with a heart defect should get tested for chromosome abnormalities and meet with a genetic counselor to help them determine their risk of having a child with a heart defect.
Dalili za Hitilafu za Moyo
Sometimes heart defects cause few or no symptoms and are not detectable even during a physical examination of the child. Some mild defects cause symptoms only later in life. Fortunately, most serious heart defects in children are detectable based on symptoms noticed by parents and by abnormalities noticed during a doctor's examination.
Because normal circulation of oxygen-rich blood is necessary for normal growth, development, and activity, infants and children with heart defects may fail to grow or gain weight normally. They may have difficulty feeding or may tire quickly during physical activities.
In more severe cases, breathing may be labored or a bluish color of the skin (cyanosis) may develop. Older children with heart defects may not be able to keep up with their peers during exercise or may experience shortness of breath, fainting, or chest pain, particularly during exercise.
Abnormal blood flow through the heart usually causes an abnormal sound (heart murmur) that can be heard using a stethoscope. Serious heart murmurs are often easy for a doctor to hear. However, the vast majority of heart murmurs that occur during childhood are not caused by heart defects and are not a sign of a problem. Murmurs that are not caused by a heart disorder are usually called innocent or functional murmurs.
Heart failure makes the heart beat rapidly and often causes fluid to collect in the lungs or liver. Fluid build up can lead to trouble breathing while eating, rapid breathing, grunting during breathing, crackling sounds in the lungs, an enlarged liver, and swelling of the legs.
Some heart defects (such as a hole in the atrium) increase the risk that a blood clot will form on the right side of the heart and pass across the defect, into the left side of the heart and then out to the body where it may block an artery in the brain, leading to a stroke. However, such blood clots are rare in childhood.
Je, Ulijua...
|
Ugonjwa wa Eisenmenger
Eisenmenger syndrome occurs when a large left-to-right shunt that is not corrected early in life leads to irreversible damage to the blood vessels of the lungs. This damage eventually leads to reversal of the shunt to one that is right-to-left.
Left-to-right shunting involves oxygen-rich blood, which is pumped from the left side of the heart, mixing with oxygen-poor blood being pumped through the pulmonary artery to the lungs. Left-to-right shunting makes the circulation inefficient and increases the amount of blood flowing to the lungs. Over time, this extra blood flow damages the lung blood vessels, causing the walls of the blood vessels to thicken abnormally. This may happen slowly, over many decades such as with an atrial septal defect or rapidly as occurs in persistent truncus arteriosus.
Eventually, the resistance to flow from the damaged and thickened lung arteries in the lungs can becomes so high that there is a reversal of blood flow from the right side of the heart to the left side. This reversal of blood flow is called Eisenmenger syndrome. Eisenmenger syndrome can overwork the right side of the heart, causing heart failure. Other complications include increasing bluish discoloration (cyanosis), abnormally increased thickness of the blood, bleeding from the lungs, and strokes.
Disorders that may lead to Eisenmenger syndrome include
Because birth defects of the heart are usually diagnosed and treated promptly, Eisenmenger syndrome is becoming less common.
Symptoms include a bluish color of the skin (cyanosis), widening and swelling of the fingernails or toenails (clubbing), fainting, shortness of breath during activity, fatigue, and chest pain. Other symptoms may develop, depending on which birth defect causes Eisenmenger syndrome.
If doctors suspect Eisenmenger syndrome, electrocardiography, echocardiography, and cardiac catheterization are done to provide more information about how the heart is functioning. Doctors also do laboratory tests to identify abnormalities caused by the lack of oxygen.
Although there are some interventions or medications that can delay the natural progression of this condition, heart and lung transplantation is the only definitive treatment for Eisenmenger syndrome. Therefore, it is important that heart birth defects are identified and corrected as soon as possible.
Utambuzi wa Ungonjwa wa Hitilafu za Moyo
Before birth, ultrasonography
Electrocardiography
Chest x-ray
Echocardiography
Cardiac catheterization
Many heart defects can be diagnosed before birth by using echocardiography (ultrasonography of the heart). If a heart defect is diagnosed or suspected by the obstetrician, the mother is often referred for a specialized ultrasound examination called fetal echocardiography. This procedure allows the fetus's heart to be examined in detail. When a serious heart defect is confirmed, plans can be made for optimal care of the newborn immediately after birth.
In the United States and many other countries, newborns are screened for heart defects when they are one or two days old. Screening is done with a pulse oximeter (a painless test that checks oxygen levels in the blood using a sensor applied to the skin). Heart defects that are not detected before or right after birth are suspected in newborns or young children when symptoms develop, when abnormal heart murmurs are heard when a doctor listens to the heart with a stethoscope, or when other signs of a heart condition are recognized.
Diagnosing heart defects in children involves the same techniques used for diagnosing heart problems in adults. Doctors will often suspect a defect after asking the family specific questions and doing a physical examination. Then they typically do echocardiography, electrocardiography (ECG), and a chest x-ray.
Echocardiography can diagnose almost all of the specific defects. Magnetic resonance imaging (MRI) of the heart and computed tomography (CT) scanning of the heart may be use to add important anatomic details of certain heart or blood vessel defects. Cardiac catheterization can provide further details of the abnormality and also can be used to treat some heart defects.
Matibabu ya Hitilafu za Moyo
Open-heart surgery
Cardiac catheterization procedures
Medications
Extracorporeal membrane oxygenation (ECMO) and ventricular assist devices (VADs)
Rarely a heart transplant
Utunzaji wa papo hapo
Heart failure or cyanosis that occurs in the first week of life is a medical emergency. Doctors often insert a thin tube (a catheter) in the newborn's vein within the umbilical cord to make giving medications easier and faster. Medications, are given by vein to reduce the workload of the heart and to improve the amount of oxygen that can be delivered to the body. In newborns, prostaglandins can be life saving in certain critical heart defects that require the ductus arteriosus to stay open. Newborns may also need a ventilator to help them breathe. When certain defects are present, newborns are sometimes also given oxygen.
Upasuaji wa moyo wazi
Many serious heart defects can be effectively repaired with open-heart surgery. The timing of the operation depends on the specific defect, its symptoms, and the severity. However, infants with severe symptoms resulting from a heart defect should have surgery during the first days or weeks of life.
The repair of some complicated heart defects may be too difficult in the first few weeks and a non-open-heart procedure may need to be done to stabilize the infant's condition and delay the need for a more corrective operation. An example of this type of operation would be creation of a shunt between the aorta and the pulmonary artery.
Uchunguzi wa mishipa ya moyo kwa kutumia katheta
Cardiac catheterization is a procedure in which a thin tube (catheter) is inserted into a vein or artery in the groin and advanced to the heart for diagnosis or treatment. Other approaches to the heart are sometimes used, including the umbilical (belly button) vein or artery in the newborn.
Narrowed structures can sometimes be widened by passing a catheter into the narrowed area of the heart. A balloon attached to the catheter is inflated and widens the narrowing, usually in a valve (a procedure called balloon valvuloplasty) or blood vessel (balloon angioplasty). These balloon procedures may be done instead of open-heart surgery or may delay the need for open-heart surgery.
In some newborns, such as those with transposition of the great arteries, a procedure called balloon atrial septostomy can be done during a cardiac catheterization. In this situation, a balloon is used to enlarge the foramen ovale (hole between the upper chambers of the heart) to help improve oxygen flow to the body. This procedure is usually done to stabilize the baby before open-heart surgery.
Cardiac catheterization can also be used to close a patent ductus arteriosus or certain holes in the heart (many atrial septal defects and some ventricular septal defects) by inserting a plug or other specialized device through the catheter. Cardiac catheterization does not leave a large scar on the skin, and the recovery time is much shorter than recovery after open-heart surgery.
Dawa
In a newborn, when blood flow to the body or to the lungs is severely blocked, a type of medication called a prostaglandin can be given to keep the ductus arteriosus open, which can be life-saving.
Other medications that are commonly used in children with a heart defect include
A diuretic, such as furosemide, which helps to remove excess fluid from the body and lungs
Angiotensin-converting enzyme (ACE) inhibitors, such as captopril, enalapril, or lisinopril (which relax blood vessels and help the heart to pump more easily)
Digoxin, which helps the heart to pump a bit more forcefully
Milrinone, a powerful drug given by vein (intravenously) to stimulate the heart to beat more strongly and relax tight blood vessels
Vifaa vya kusaidia utendakazi wa moyo
Mechanical devices may be used to support the heart in children who have severe heart failure and do not respond to medication. These devices have a pump that helps to send enough blood to the lungs and to the body when the heart is unable to pump effectively. They can be used for days, weeks, or even months to allow a child's heart to recover from a viral infection or major open-heart surgery or to help stabilize the child until a heart transplant can be done.
In extracorporeal membrane oxygenation (ECMO), blood from the child is circulated through a machine that adds oxygen and removes carbon dioxide and then pumps that blood to the child's body.
Some devices, called ventricular assist devices (VADs) can be inserted into the body. A VAD pumps blood from the heart to the body. This device allows for longer support of the circulation than ECMO.
Upandikizaji wa moyo
In rare cases, when no other treatment helps, heart transplantation is done. However, the lack of donor hearts limits the availability of this procedure.
Usimamizi wa muda mrefu
Children with a weak heart muscle or residual valve problems after surgery require long-term treatment with medications and changes to their diet (such as salt restriction and use of a high-calorie formula in a relatively small amount of liquid). These treatments decrease the workload of the heart.
Some children who have significant heart defects or have had surgeries to repair their heart defects need to take antibiotics before visits to the dentist and before certain surgeries (such as on the respiratory tract). These antibiotics are used to prevent a serious heart infection called endocarditis. However, most children with heart defects, whether or not they had surgery, do not require these antibiotics. However, all children with heart defects, should take good care of their teeth and gums to decrease the risk of infection spreading to their heart.
Taarifa Zaidi
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
American Heart Association: Common Heart Defects: Provides an overview of common birth defects of the heart for parents and caregivers
American Heart Association: Infective Endocarditis: Provides an overview of infective endocarditis, including summarizing antibiotic use, for parents and caregivers


