


Benign paroxysmal positional vertigo (BPPV) is a common disorder causing short episodes of vertigo (a false sensation of moving or spinning) in response to changes in head position that stimulate the posterior semicircular canal of the inner ear.
People briefly (usually for less than a minute) feel as if they or their surroundings are moving or spinning when they move their head.
People may also feel nauseated and vomit, and their eyes may move abnormally.
Doctors base the diagnosis on symptoms and the situations in which they occur and results of a physical examination.
The Epley maneuver, done once or twice, relieves symptoms in most people.
People with vertigo have a false sensation that they, their surroundings, or both are moving or spinning. Most people describe this unpleasant feeling as "dizziness," although people often also use the word "dizzy" for other sensations, such as being light-headed. "Positional" vertigo means that the vertigo occurs when people change position, for example, laying down in bed and turning their head. "Benign" means that the disorder is not dangerous.
BPPV affects people increasingly as they age and can severely affect balance in older people, which may lead to falls and possibly injuries. Sometimes BPPV occurs after head trauma.
(See also Overview of the Inner Ear.)
Sababu za Kizunguzungu Chenye Nafuu Kinachotokana na Mwelekeo wa Muda Mfupi
Most episodes of BPPV are triggered by a change in head position—typically turning the head over on the pillow after awakening in the morning or tipping the head backward to reach a high shelf. BPPV usually develops when calcium particles (otoconia) that are normally embedded in one part of the inner ear (the utricle and saccule) are displaced and move into another part of the inner ear (most commonly the posterior semicircular canal).
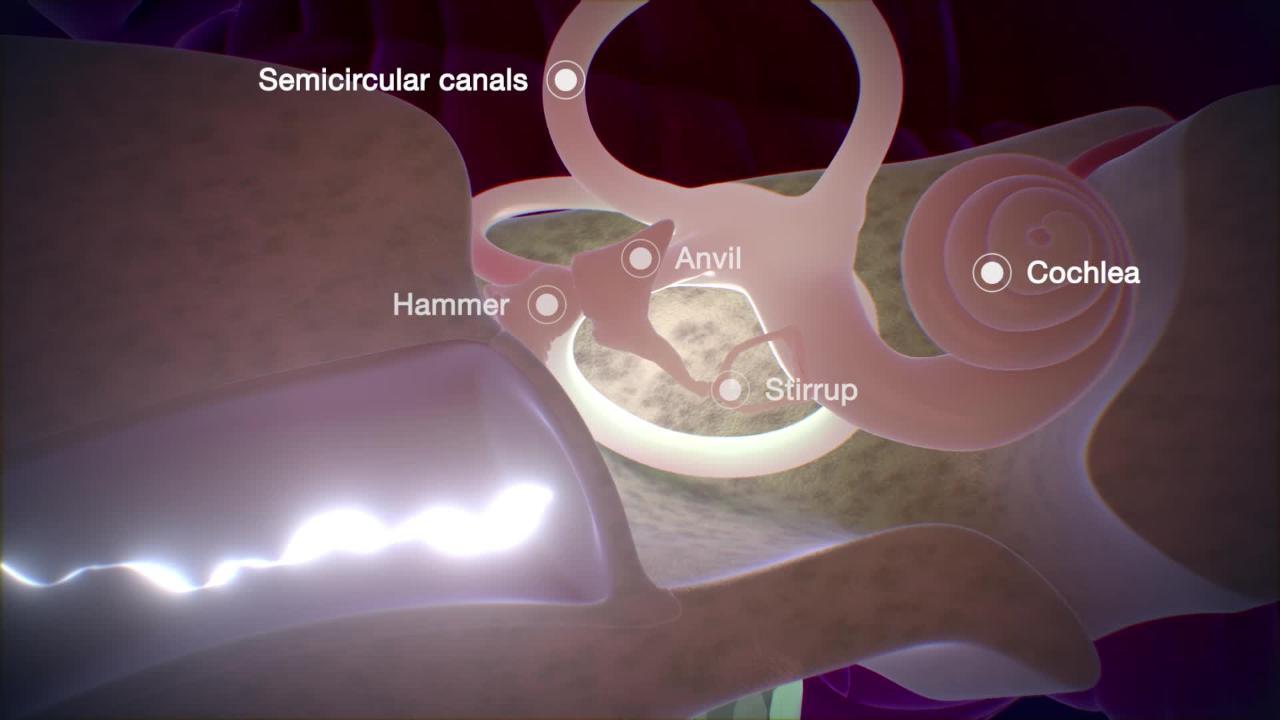
The inner ear contains three semicircular canals, which help with balance. Of the three canals,the posterior canal is in the best position to receive most of the loose particles through gravity during the night. Less commonly, the particles move into the other two canals. As the particles collect, they form a chalky sludge that exaggerates the movement of fluid in the canal when the head changes position. The result is overstimulation of nerve receptors (hair cells) inside the posterior canal, creating a false sensation of moving or spinning.
Kuangalia Ndani ya Sikio




Particles may be displaced from the utricle and saccule as people age. Or, displacement may be caused by
Ear infections
Head or ear injury
Prolonged bed rest
Ear surgery
Some people with symptoms of BPPV have other disorders including other inner ear disorders (such as Meniere disease), blockage of an artery to the inner ear, and a tumor of the central nervous system.
Dalili za Kizunguzungu Chenye Nafuu Kinachotokana na Mwelekeo wa Muda Mfupi
The symptoms of BPPV are
Short episodes of vertigo, in which people feel as if they or their surroundings are moving or spinning
Nausea and/or vomiting
BPPV can be frightening and uncomfortable, but it is usually harmless and disappears by itself or with simple maneuvers.
Vertigo is triggered when the person’s head moves, such as when rolling over in bed or bending over to pick up something. Each episode of vertigo lasts only a few seconds to minutes. People may have many episodes over the course of a few days to weeks after which episodes gradually subside on their own. Vertigo may be accompanied by nausea, vomiting, and a specific type of eye movement in which the eyes rapidly jerk in one direction alternating with a slower drift back to their original position (called nystagmus). No hearing loss or noise in the ears (tinnitus) occurs.
Although the symptoms are not dangerous, they may lead to falls or other accidents if an episode occurs while a person is in a possibly unsafe situation such as driving a car.
Utambuzi wa Kizunguzungu Chenye Nafuu Kinachotokana na Mwelekeo wa Muda Mfupi
Dix-Hallpike maneuver
Sometimes imaging tests
Diagnosis of BPPV is based on a description of the symptoms and the circumstances in which they occur.
Usually, the test used is the Dix-Hallpike maneuver. During the Dix-Hallpike maneuver
The person sits on the examining table with the head turned 45 degrees to the right.
Then the person lies down backwards so that the head remains turned at 45 degrees and hangs over the examining table by about 20 degrees.
There is a delay of about 5 to 10 seconds (called latency) before vertigo and nystagmus occur, but the delay may be as long as 30 seconds.
Symptoms last 10 to 30 seconds, then decrease and disappear (called fatigue).
Maintaining the gaze on a single location (visual fixation) can shorten or even abolish nystagmus, so the maneuver is ideally done with the person wearing Frenzel lenses (which make it impossible to visually fixate on anything).
If the maneuver is repeated several times, the intensity of the vertigo and nystagmus decreases (called habituation or fatigability) in people who have BPPV. However, in people who have vertigo due to a brain disorder (such as stroke or multiple sclerosis), which is more serious, the Dix-Hallpike maneuver triggers symptoms immediately, the vertigo persists as long as the head is held in the same position, and habituation does not occur when the maneuver is repeated.
Sometimes imaging tests (such as gadolinium-enhanced magnetic resonance imaging) are done when doctors are not sure whether the vertigo is being caused by another, possibly dangerous, disorder.
Matibabu ya Kizunguzungu Chenye Nafuu Kinachotokana na Mwelekeo wa Muda Mfupi
Head maneuvers to reposition particles in the ear canal
Usually, BPPV is easily treated. Medications are not typically recommended. They rarely help and can worsen symptoms.
Displaced particles can often by moved out of the posterior semicircular canal and into a part of the ear where they do not cause symptoms. Doing so requires a somersault-like maneuver of the head, called a canalith repositioning maneuver, such as the Epley maneuver. This maneuver immediately lessens vertigo in about 90% of people. Repeating the maneuver may help a few additional people.
Maneva ya Epley: Tiba Rahisi ya Sababu za Kawaida za Kizunguzungu

In the Epley maneuver, the person’s body and head are moved into different positions, one after the other. Each position is maintained for about 30 seconds to allow the particles to move by gravity into a different part of the canal. To check if the maneuver worked, the person moves the head in the same way that previously caused vertigo. If vertigo does not occur, the maneuver worked. After this maneuver is done, people should remain upright or semiupright for 1 to 2 days.
In some people, the vertigo recurs. If it does, the repositioning maneuver is repeated. People can be taught how to do the maneuver at home in case vertigo recurs.
Another effective maneuver, called the Brandt-Daroff exercise, can be taught to the person and be done at home. The person sits upright, then lies on one side with the head turned at a 45-degree angle. The person remains in this position for about 30 seconds or until the vertigo subsides and then sits upright again. The same motion is repeated on the opposite side. This cycle is repeated 5 times in a row, 3 times a day for about 2 weeks or until vertigo no longer occurs when the exercise is done.
Although the posterior semicircular canal is most commonly affected by BPPV, occasionally the lateral canal is affected, and people can roll themselves like a log to relieve the symptoms.
If the repositioning maneuvers do not work, doctors usually look for other, more serious, disorders that may be the cause of symptoms and require other treatments.
Very rarely, surgery is needed.


