


Normally, 10 to 20 mL of pleural fluid, similar in composition to plasma but lower in protein (< 1.5 g/dL [< 15 g/L]), is spread thinly over the visceral and parietal pleurae, facilitating movement between the lungs and chest wall. The fluid enters the pleural space from systemic capillaries in the parietal pleurae and exits via parietal pleural stomas and lymphatics. The fluid ultimately drains into the right atrium, so clearance is dependent on capillary and, in part, right-sided pressures. Pleural fluid accumulates when too much fluid enters or too little exits the pleural space.
Etiology of Pleural Effusion
Pleural effusions are usually categorized as
Transudates
Exudates
Categorization of the effusions is based on laboratory characteristics of the fluid (see table Criteria for Identifying Exudative Pleural Effusions). Whether unilateral or bilateral, a transudate can usually be treated without extensive evaluation, whereas the cause of an exudate requires investigation. There are numerous (> 50) causes (see table Some Causes of Pleural Effusion).
Transudative effusions are caused by some combination of increased hydrostatic pressure and decreased plasma oncotic pressure. Heart failure is the most common cause, followed by cirrhosis with ascites and by hypoalbuminemia, usually due to the nephrotic syndrome.
Exudative effusions are caused by local processes that lead to increased capillary permeability, resulting in exudation of fluid, protein, cells, and other serum constituents. Causes are numerous; the most common are pneumonia, cancer, pulmonary embolism, viral infection, and tuberculosis (TB).
Yellow nail syndrome is a rare disorder causing chronic exudative pleural effusions, lymphedema, and dystrophic yellow nails—all thought to be the result of impaired lymphatic drainage.
Criteria for Identifying Exudative Pleural Effusions
Test | Exudate | Sensitivity (%) | Specificity (%) |
|---|---|---|---|
Light’s criteria (≥ 1 of the following 3): | 98 | 77 | |
| ≥ 2/3 ULN for serum LDH | 66 | 100 |
| ≥ 0.5 | 91 | 89 |
| ≥ 0.6 | 93 | 82 |
Fluid total protein | ≥ 3 g/dL (30 g/L) | 90 | 90 |
Fluid cholesterol | ≥ 60 mg/dL (1.55 mmol/L) ≥ 43 mg/dL (1.11 mmol/L) | 54 75 | 92 80 |
Pleural fluid:serum cholesterol ratio | ≥ 0.3 | 89 | 71 |
Serum protein – pleural fluid protein† | ≤ 3.1 g/dL (31 g/L) | 87 | 92 |
* Correction for increase in LDH due to red blood cell lysis = measured LDH − 0.0012 × red blood cell count/mcL. | |||
† Preferred test for patients who are prescribed diuretics after development of effusion if Light’s exudative criteria are met, but none of the biochemical measurements are > 15% above the cutoff levels for Light’s criteria. | |||
LDH = lactate dehydrogenase; ULN = upper limit of normal. | |||
Data modified from Light RW: Clinical practice: Pleural effusion. N Engl J Med 346:1971–1977, 2002. doi:10.1056/NEJMcp010731 | |||
Chylous effusion (chylothorax) is a milky white effusion high in triglycerides caused by traumatic or neoplastic (most often lymphomatous) damage to the thoracic duct. Chylous effusion also occurs with the superior vena cava syndrome.
Chyliform (cholesterol or pseudochylous) effusions resemble chylous effusions but are low in triglycerides and high in cholesterol. Chyliform effusions are thought to be due to release of cholesterol from lysed red blood cells and neutrophils in long-standing effusions when absorption is blocked by the thickened pleura. The most common causes are rheumatoid pleuritis and chronic TB.
Hemothorax is bloody fluid (pleural fluid hematocrit > 50% peripheral hematocrit) in the pleural space due to trauma or, rarely, as a result of coagulopathy or after rupture of a major blood vessel, such as the aorta or pulmonary artery.
Empyema is pus in the pleural space. It can occur as a complication of pneumonia, thoracotomy, abscesses (lung, hepatic, or subdiaphragmatic), or penetrating trauma with secondary infection. Empyema necessitatis is soft-tissue extension of empyema leading to chest wall infection and external drainage.
Trapped lung is a lung encased by a fibrous peel caused by empyema or tumor. Because the lung cannot expand, the pleural pressure becomes more negative than normal, increasing transudation of fluid from parietal pleural capillaries. The fluid characteristically is borderline between a transudate and an exudate; ie, the biochemical values are within 15% of the cutoff levels for Light’s criteria (see table Criteria for Identifying Exudative Pleural Effusions).
Iatrogenic effusions can be caused by migration or misplacement of a feeding tube into the trachea or perforation of the superior vena cava by a central venous catheter, leading to infusion of tube feedings or IV solution into the pleural space.
Some Causes of Pleural Effusion*
Cause | Comments |
|---|---|
Transudate | |
Bilateral effusions in 81%; right-sided in 12%; left-sided in 7% † With left ventricular failure, there is increased interstitial fluid, which crosses the visceral pleura and enters the pleural space | |
Cirrhosis with ascites (hepatic hydrothorax) | Right-sided effusions in 70%; left-sided in 15%; bilateral in 15% ‡ Ascitic fluid migration to the pleural space through diaphragmatic defects Effusion present in about 5% of patients with clinically apparent ascites |
Hypoalbuminemia | Uncommon Bilateral effusions in > 90% Intravascular oncotic pressure decreases, which leads to the pleural effusions Associated with edema or anasarca elsewhere |
Usually bilateral effusions; commonly subpulmonic Decreased intravascular oncotic pressure plus hypervolemia causing transudation into the pleural space | |
Retroperitoneal urine dissection into the pleural space, causing urinothorax | |
Constrictive pericarditis | Increases in right- and left-sided IV hydrostatic pressure In some patients, accompanied by massive anasarca and ascites due to a mechanism similar to that for hepatic hydrothorax |
Increases negative intrapleural pressure | |
Mechanism similar to that for hepatic hydrothorax Pleural fluid with characteristics similar to dialysate | |
Trapped lung | Encasement with fibrous peel increasing negative intrapleural pressure May be exudative or borderline exudate |
Systemic capillary leak syndrome | Rare Accompanied by anasarca and pericardial effusion |
Myxedema (hypothyroidism) | Effusion present in about 5% Usually transudate if pericardial effusion is also present, due to elevated hydrostatic pressures; either transudate or exudate if pleural effusion is isolated |
Exudate | |
Pneumonia (parapneumonic effusion) | May be uncomplicated (not frankly infected), or complicated with loculations or septations, or purulent (empyema) Thoracentesis necessary to differentiate Pleural fluid chemistry typically shows very high LDH (eg, > 900 U/L [15 microkat/L]) and low glucose |
Cancer | Most commonly lung cancer, breast cancer, or lymphoma but possible with any tumor metastatic to pleurae Typically causing dull, aching chest pain |
Effusion present in about 30%: Almost always exudative; bloody in < 50% Pulmonary embolism suspected when dyspnea is disproportionate to size of effusion | |
Viral infection | Effusion usually small with or without parenchymal infiltrate Predominantly systemic symptoms rather than pulmonary symptoms |
Effusions left-sided or larger on the left in 73%; bilateral and equal in 20%; right-sided or larger on the right in 7% > 25% of the hemithorax filled with fluid 30 days postoperatively in 10% of patients Bloody effusions related to postoperative bleeding likely to resolve Nonbloody effusions likely to recur; etiology unknown but probably with an immunologic basis | |
Effusion usually unilateral and ipsilateral to parenchymal infiltrates if present Effusion due to hypersensitivity reaction to TB protein Pleural fluid TB cultures positive in < 20% Typically, pleural fluid glucose level low (in the low nearly normal range) compared with serum glucose | |
Effusion in 1–2% Extensive parenchymal sarcoid and often extrathoracic sarcoid Pleural granulomas in many patients without effusion Pleural fluid predominantly lymphocytic | |
Uremia | Effusion in about 3% In > 50%, symptoms secondary to effusion: Most commonly fever (50%), chest pain (30%), cough (35%), and dyspnea (20%) Diagnosis of exclusion |
Infradiaphragmatic abscess | Causes sympathetic subpulmonic effusion Neutrophils predominant in pleural fluid pH and glucose normal |
Many possible etiologic factors: Pneumonias (parapneumonic), including Pneumocystis jirovecii pneumonia, other opportunistic infections, TB, and pulmonary Kaposi sarcoma | |
Effusion typically in older men with rheumatoid nodules and deforming arthritis Must differentiate from parapneumonic effusion (both characterized by low glucose, low pH, and high LDH) | |
Effusion possibly first manifestation of SLE Common with drug-induced SLE Diagnosis established by serologic tests of blood, not of pleural fluid | |
Medications | |
Ovarian hyperstimulation syndrome | Effusion developing 7–14 days after hCG injection Effusion right-sided in 52%; bilateral in 27% |
Acute: Effusion present in about 50%: Bilateral in 77%; left-sided in 16%; right-sided in 8% Effusion due to transdiaphragmatic transfer of the exudative inflammatory fluid and diaphragmatic inflammation Chronic: Effusion due to sinus tract from pancreatic pseudocyst through diaphragm into pleural space Predominantly chest symptoms rather than abdominal symptoms Patients presenting with cachexia that resembles cancer | |
Superior vena cava syndrome | Effusion usually caused by blockage of intrathoracic venous and lymphatic flow by cancer or thrombosis in a central catheter May be an exudate or a chylothorax |
Patients extremely sick Medical emergency Morbidity and mortality due to infection of the mediastinum and pleural space | |
Benign asbestos pleural effusion | Effusion occurring > 30 years after initial exposure Frequently asymptomatic Tends to come and go Diagnosis of exclusion; must rule out mesothelioma |
Benign ovarian tumor (Meigs syndrome) | Mechanism similar to that for hepatic hydrothorax Surgery sometimes indicated for patients with ovarian mass, ascites, and pleural effusion For diagnosis, disappearance of ascites and effusion postoperatively required |
Yellow nail syndrome | Triad of pleural effusion, lymphedema, and yellow nails, sometimes appearing decades apart Pleural fluid with relatively high protein but low lactate dehydrogenase Tendency for effusion to recur No pleuritic chest pain |
* Causes are listed in approximate order of greatest frequency first. | |
† Morales-Rull JL, Bielsa S, Conde-Martel A, et al. Pleural effusions in acute decompensated heart failure: Prevalence and prognostic implications. Eur J Intern Med 2018;52:49-53. doi:10.1016/j.ejim.2018.02.004 | |
‡ Alonso JC. Pleural effusion in liver disease. Semin Respir Crit Care Med 2010;31(6):698-705. doi:10.1055/s-0030-1269829 | |
hCG = human chorionic gonadotropin; IV = intravenous; LDH = lactate dehydrogenase. | |
Effusions with no obvious cause are often due to occult pulmonary emboli, tuberculosis, or cancer (1). Etiology is unknown for some effusions even after extensive study (also referred to as non-specific pleuritis); many of these effusions are thought to be due to viral infection.
Etiology reference
1. Roberts ME, Rahman NM, Maskell NA, et al. British Thoracic Society Guideline for pleural disease. Thorax 2023;78(Suppl 3):s1-s42. doi:10.1136/thorax-2022-219784
Symptoms and Signs of Pleural Effusion
Some pleural effusions are asymptomatic and are discovered incidentally during physical examination or on chest x-ray.
Many effusions cause dyspnea, pleuritic chest pain, or both. Pleuritic chest pain, a vague discomfort or sharp pain that worsens during inspiration, indicates inflammation of the parietal pleura. Pain is usually felt over the inflamed site, but referred pain is possible. The posterior and peripheral portions of the diaphragmatic pleura are supplied by the lower 6 intercostal nerves, and irritation there may cause pain in the lower chest wall or abdomen that may simulate intra-abdominal disease. Irritation of the central portion of the diaphragmatic pleura, innervated by the phrenic nerves, causes pain that is referred to the neck and shoulder.
Physical examination reveals absent tactile fremitus, dullness to percussion, and decreased breath sounds on the side of the effusion. These findings can also be caused by pleural thickening. With large-volume effusions, respiration is usually rapid and shallow.
A pleural friction rub, although infrequent, is the classic physical sign. The friction rub varies from a few intermittent sounds that may simulate crackles to a fully developed harsh grating, creaking, or leathery sound synchronous with respiration, heard during inspiration and expiration. Friction sounds adjacent to the heart (pleuropericardial rub) may vary with the heartbeat and may be confused with the friction rub of pericarditis. Pericardial rub is best heard over the left border of the sternum in the 3rd and 4th intercostal spaces, is characteristically a to-and-fro sound synchronous with the heartbeat, and is not influenced significantly by respiration. Sensitivity and specificity of the physical examination for detecting effusion are probably low.

Diagnosis of Pleural Effusion
Chest x-ray
Thoracic ultrasonography
Pleural fluid analysis
Sometimes CT with venous contrast, CT angiography, or other tests
Pleural effusion is suspected in patients with pleuritic pain, unexplained dyspnea, or suggestive signs. Diagnostic tests are indicated to document the presence of pleural fluid and to determine its cause (see figure Diagnosis of Pleural Effusion).
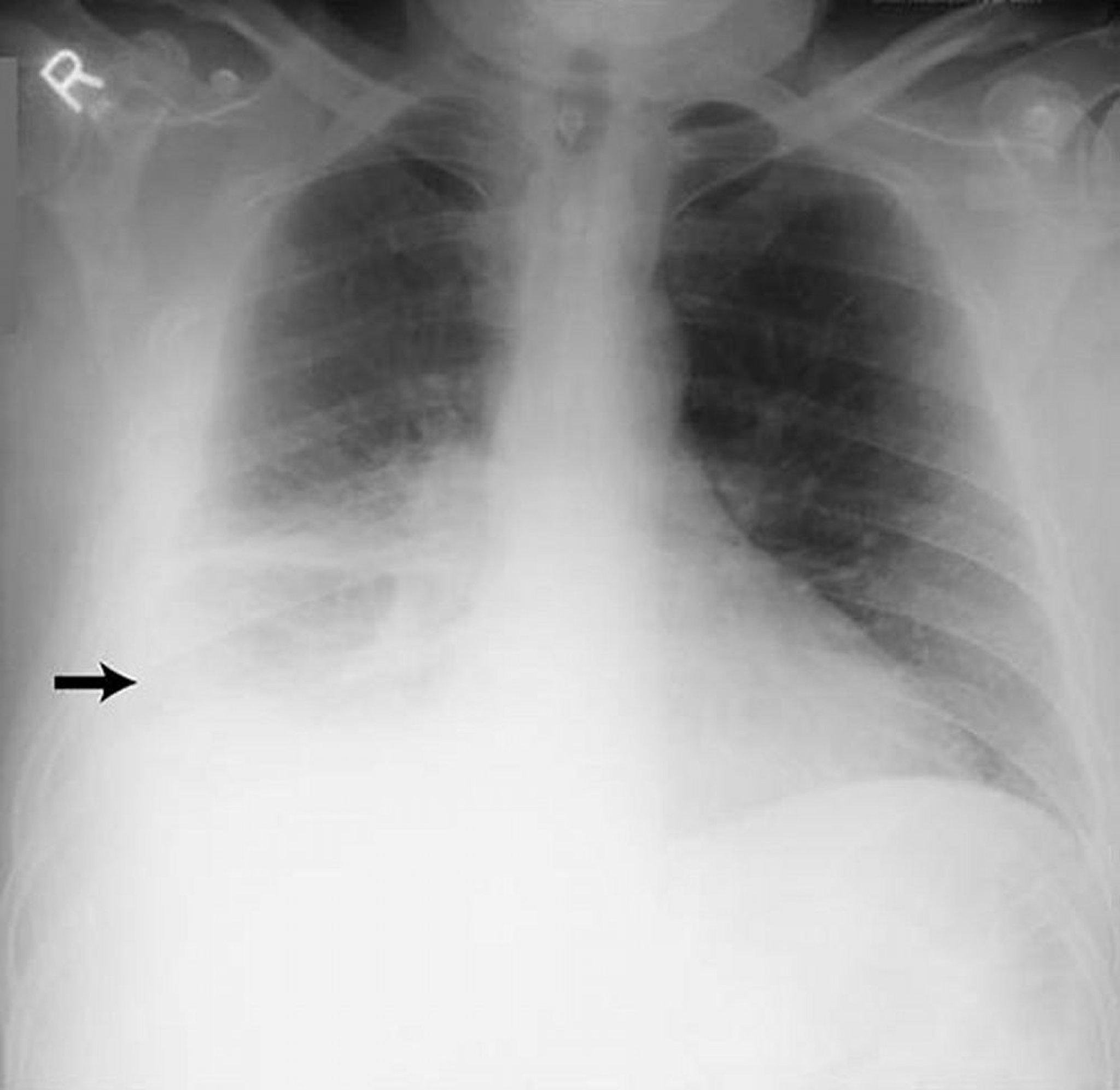
Presence of effusion


By permission of the publisher. From Huggins J, Sahn S. In Bone's Atlas of Pulmonary and Critical Care Medicine. Edited by J Crapo. Philadelphia, Current Medicine, 2005.
Chest x-ray is the first test done to confirm the presence of pleural fluid. The lateral upright chest x-ray should be examined when a pleural effusion is suspected. In an upright x-ray, 75 mL of fluid blunts the posterior costophrenic angle. Blunting of the lateral costophrenic angle usually requires about 175 mL but may take as much as 500 mL. Larger pleural effusions opacify portions of the hemithorax and may cause mediastinal shift; effusions > 4 L may cause complete opacification of the hemithorax and mediastinal shift to the contralateral side.

By permission of the publisher. From Huggins J, Sahn S. In Bone's Atlas of Pulmonary and Critical Care Medicine. Edited by J Crapo. Philadelphia, Current Medicine, 2005.

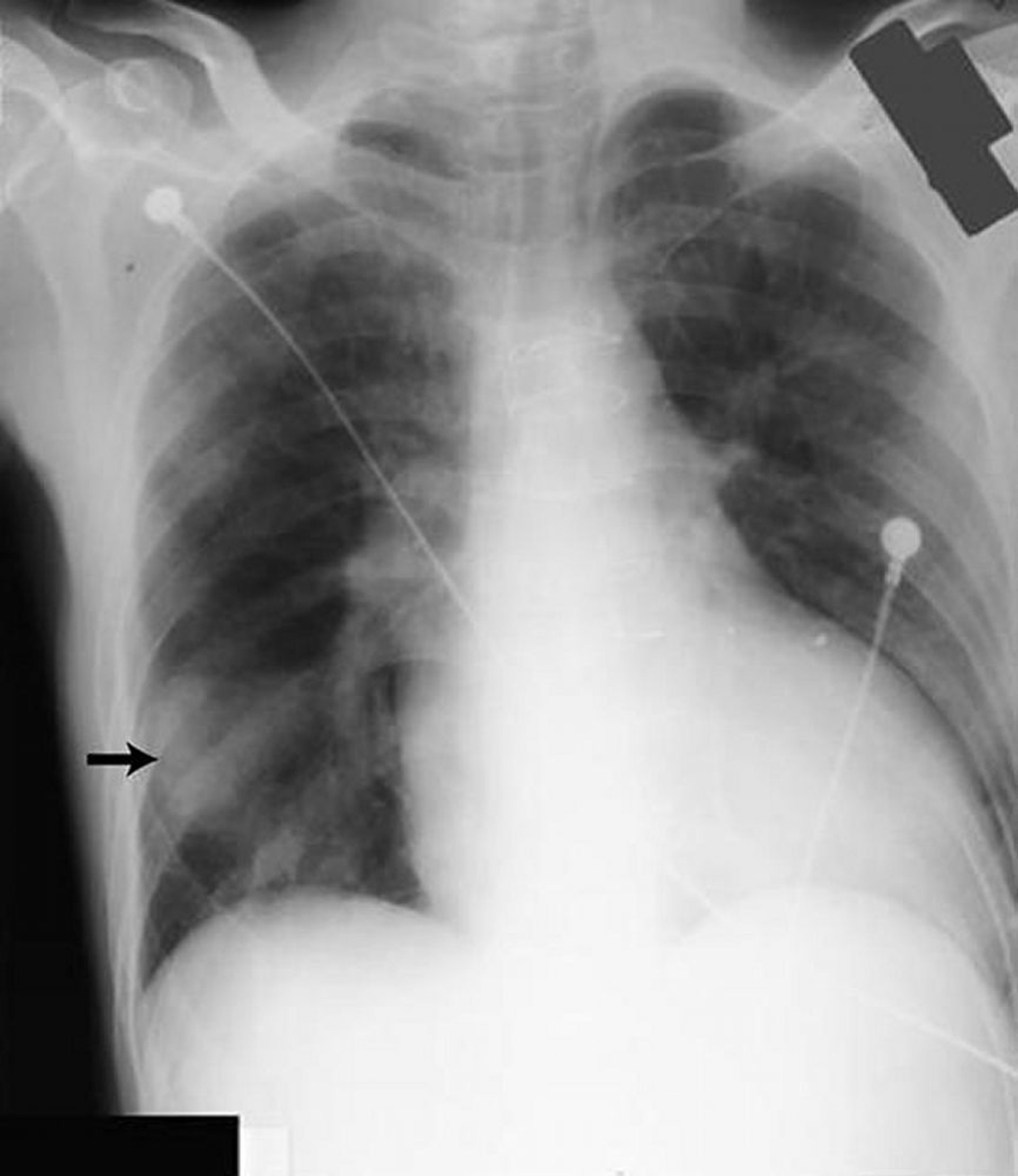
By permission of the publisher. From Huggins J, Sahn S. In Bone's Atlas of Pulmonary and Critical Care Medicine. Edited by J Crapo. Philadelphia, Current Medicine, 2005.
Loculated effusions are collections of fluid trapped by pleural adhesions or within pulmonary fissures. Further imaging (lateral decubitus x-rays, chest CT, or ultrasonography) should be done if it is unclear whether an x-ray density represents fluid or parenchymal infiltrates or whether suspected fluid is loculated or free-flowing; these tests are more sensitive than upright x-rays and can detect small fluid volumes. Loculated effusions, particularly those in the horizontal or oblique fissure, can be confused with a solid pulmonary mass (pseudotumor). They may change shape and size with changes in the patient’s position and amount of pleural fluid.
Thoracic ultrasonography is considered standard of care for diagnosis of pleural effusion and is done at the bedside by pulmonologists, or sometimes emergency physicians, avoiding the need for radiologist review. It is highly accurate for the detection of small volumes of pleural fluid and provides additional diagnostic information (eg, the presence of septation, pleural thickening).
CT with venous contrast is a valuable next investigation that provides information on pleural enhancement and potential pleural nodularity. CT with venous contrast is valuable for evaluating the underlying lung parenchyma for infiltrates or masses when the lung is obscured by the effusion or when the detail on chest x-rays is insufficient for distinguishing loculated fluid from a solid mass.


Image courtesy of Najib M. Rahman, BMBCh MA (oxon) DPhil.

Image courtesy of Najib M. Rahman, BMBCh MA (oxon) DPhil.
Cause of effusion
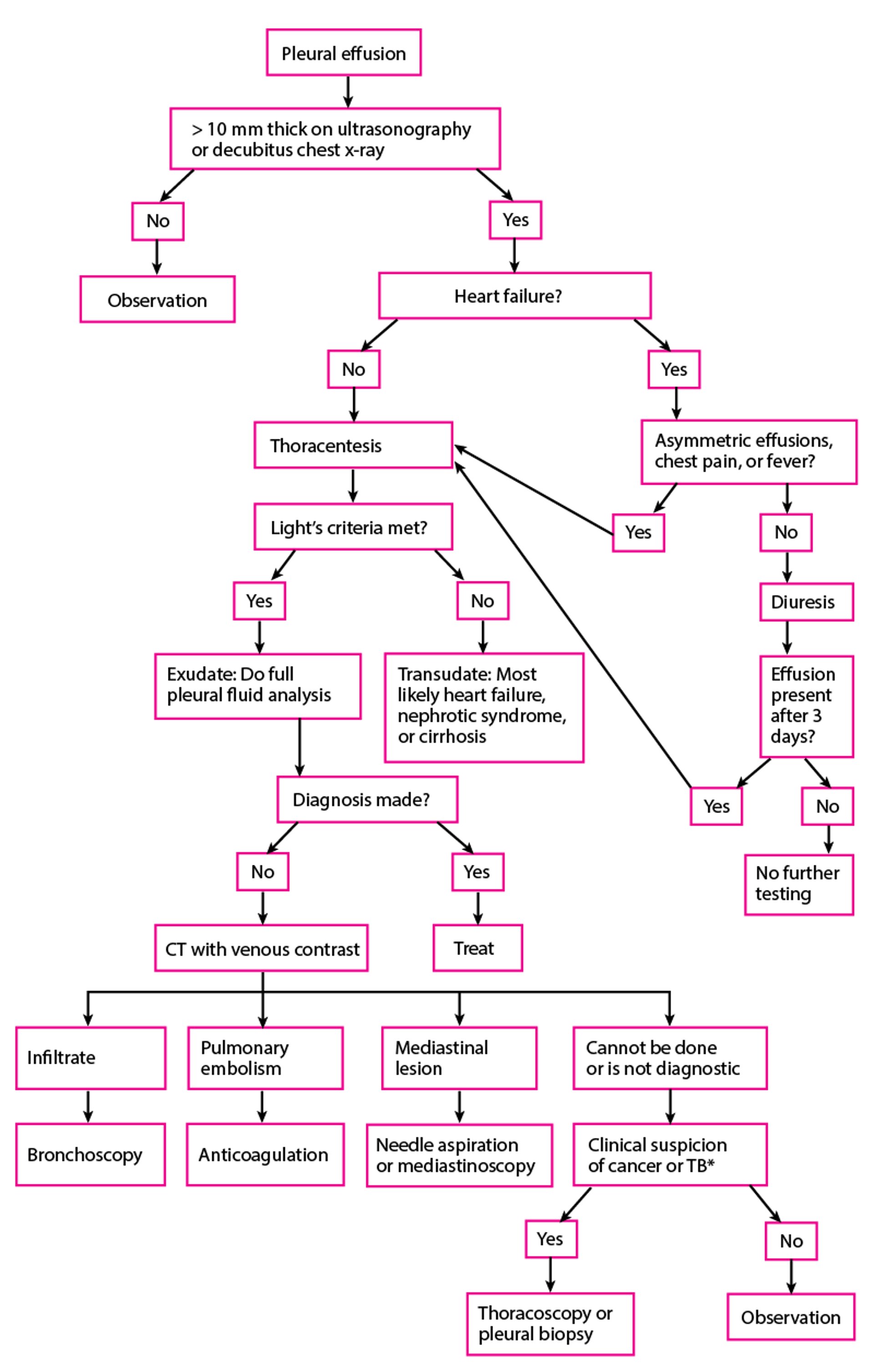
Thoracentesis should be done in almost all patients who have pleural fluid that is ≥ 10 mm in thickness on CT, ultrasonography, or lateral decubitus x-ray and that is new or of uncertain etiology. In general, the only patients who do not require thoracentesis are those who have heart failure with symmetric pleural effusions and no chest pain or fever; in these patients, diuresis can be tried, and thoracentesis avoided unless effusions persist for ≥ 3 days. Thoracentesis and subsequent pleural fluid analysis are also often unnecessary for pleural effusions that are chronic, have a known cause, and cause no symptoms.
Thoracentesis should be done using ultrasonographic guidance in all cases because it increases procedure accuracy and prevents complications.
Pearls & Pitfalls
|
Pleural fluid analysis is done to diagnose the cause of pleural effusion. Analysis begins with visual inspection, which can
Distinguish bloody and chylous (or chyliform) from other effusions
Identify purulent effusions strongly suggestive of empyema
Identify viscous fluid, which is characteristic of some mesotheliomas
Fluid should always be sent for total protein, glucose, lactate dehydrogenase (LDH), cell count and cell differential, and Gram stain. Other tests such as pleural fluid pH, aerobic and anaerobic bacterial cultures, cytology, tuberculosis fluid markers [adenosine deaminase or interferon-gamma], amylase, mycobacterial and fungal stains and cultures, triglycerides, and cholesterol are used in appropriate clinical settings.
Fluid analysis helps distinguish transudates from exudates; multiple criteria exist, but not one perfectly discriminates between the 2 types. When Light’s criteria are used (see table Criteria for Identifying Exudative Pleural Effusions), serum LDH and total protein levels should be measured as close as possible to the time of thoracentesis for comparison with those in pleural fluid. Light’s criteria correctly identify almost all exudates but misidentify about 20% of transudates as exudates. If transudative effusion is suspected (eg, due to heart failure or cirrhosis) and none of the biochemical measurements are < 15% above the cutoff levels for Light’s criteria, the difference between serum and the pleural fluid protein is measured. If the difference is > 3.1 g/dL (> 31 g/L), the patient probably has a transudative effusion.
Imaging may also help. If the diagnosis remains unclear after pleural fluid analysis, CT with venous contrast enhancement is indicated to assess for pleural enhancement, pleural nodularity, pulmonary infiltrates, or mediastinal lesions. CT pulmonary angiography is indicated to rule out suspected pulmonary embolus. Findings of pulmonary emboli indicate the need for long-term anticoagulation. Pleural nodularity and thickening indicate the need for pleural biopsy (thoracoscopic or image guided). The presence of lung infiltrates or lesions, depending on suspected causes, may indicate the need for bronchoscopy or image-guided lung biopsy.
When tuberculous pleuritis is suspected, the level of adenosine deaminase in the pleural fluid is measured. A level > 40 U/L (667 nkat/L) has a 95% sensitivity and specificity for the diagnosis of tuberculous pleuritis (1); however, the adenosine deaminase level can also be positive in patients with cancer.
Diagnosis of Pleural Effusion
* Based on presence of fever, weight loss, history of cancer, or other suggestive symptoms. TB = tuberculosis. |

Diagnosis reference
1. Roberts ME, Rahman NM, Maskell NA, et al. British Thoracic Society Guideline for pleural disease. Thorax 2023;78(Suppl 3):s1-s42. doi:10.1136/thorax-2022-219784
Treatment of Pleural Effusion
Treatment of symptoms and underlying disorder
Drainage of some symptomatic effusions
Other treatments for parapneumonic and malignant effusions
The effusion itself generally does not require treatment if it is asymptomatic because many effusions resorb spontaneously when the underlying disorder is treated, especially effusions due to uncomplicated pneumonias, pulmonary embolism, or surgery. Pleuritic pain can usually be managed with nonsteroidal anti-inflammatory drugs (NSAIDs) or other oral analgesics. At times, a short course of oral opioids is required.
Therapeutic thoracentesis (usually around 1 to 1.5 L in a single treatment) is sufficient for many symptomatic effusions and can be repeated for effusions that reaccumulate. There are no arbitrary limits on the amount of fluid that can be removed (1). Removal of fluid can be continued until the effusion is drained or the patient develops chest tightness, chest pain, or severe coughing.
Effusions that are chronic, recurrent, and causing symptoms can be treated with pleurodesis or by intermittent drainage with an indwelling catheter. Effusions caused by pneumonia or cancer may require additional specific measures.
Parapneumonic effusion and empyema
In patients with adverse prognostic factors (pH < 7.20, glucose < 60 mg/dL [< 3.33 mmol/L], positive Gram stain or culture, loculations), the effusion should be completely drained via thoracentesis or tube thoracostomyVideo-assisted thoracoscopic surgery (VATS) is usually tried first, although thoracotomy may be required.
Malignant pleural effusion
If dyspnea caused by malignant pleural effusion is relieved by thoracentesis but fluid and dyspnea redevelop, chronic (intermittent) drainage or pleurodesis is indicated. Asymptomatic effusions and effusions causing dyspnea unrelieved by thoracentesis do not require additional procedures.
Shunting of pleural fluid to the peritoneum (pleuroperitoneal shunt) is rarely done but is an option in patients who have trapped lung.
Surgical treatment (pleurectomy or decortication) should be considered in patients with trapped lung who have good performance status and a good prognosis.
Treatment reference
1. Feller-Kopman D, Berkowitz D, Boiselle P, et al: Large-volume thoracentesis and the risk of reexpansion pulmonary edema. Ann Thoracic Surg 84:1656–1662, 2007.
Key Points
Transudative effusions are caused by some combination of increased hydrostatic pressure and decreased plasma oncotic pressure.
Exudative effusions result from increased capillary permeability, leading to leakage of protein, cells, and other serum constituents.
The most common causes of transudative effusions are heart failure, cirrhosis with ascites, and hypoalbuminemia (usually due to the nephrotic syndrome).
The most common causes of exudative effusions are pneumonia, cancer, pulmonary embolism, and tuberculosis.
Evaluation requires imaging (usually chest x-ray and thoracic ultrasonography) to confirm presence of fluid and pleural fluid analysis to help determine cause.
Lateral decubitus x-rays, chest CT, or ultrasonography should be done if it is unclear whether an x-ray density represents fluid or parenchymal infiltrates or whether suspected fluid is loculated or free-flowing.
Effusions that are chronic or recurrent and causing symptoms can be treated with pleurodesis or by intermittent drainage with an indwelling catheter.







