



Surgical tube thoracostomy is insertion of a surgical tube into the pleural space to drain air or fluid from the chest.
Topic Resources


Indications for Tube and Catheter Thoracostomy
Pneumothorax that is recurrent, persistent, traumatic, large, under tension, or bilateral
Pneumothorax in a patient receiving positive-pressure ventilation
Symptomatic or recurrent large pleural effusion
Empyema or complicated parapneumonic effusion
Chylothorax
Contraindications to Tube and Catheter Thoracostomy
Absolute contraindications:
None
Relative contraindications:
Coagulopathy or bleeding disorder (may require blood products or coagulation factors)
Skin or soft tissue infection at the site (a different site without infection should be used if possible to avoid introducing intrathoracic infections)
Complications of Tube and Catheter Thoracostomy
Malpositioning of the tube in the lung parenchyma, in the lobar fissure, under the diaphragm, or subcutaneously
Blockage of the tube due to blood clots, debris, or kinking
Dislodgement of the tube, requiring replacement
Bleeding
Infection of residual pleural fluid or recurrent effusion
Re-expansion pulmonary edema
Subcutaneous emphysema
Pulmonary or diaphragmatic laceration
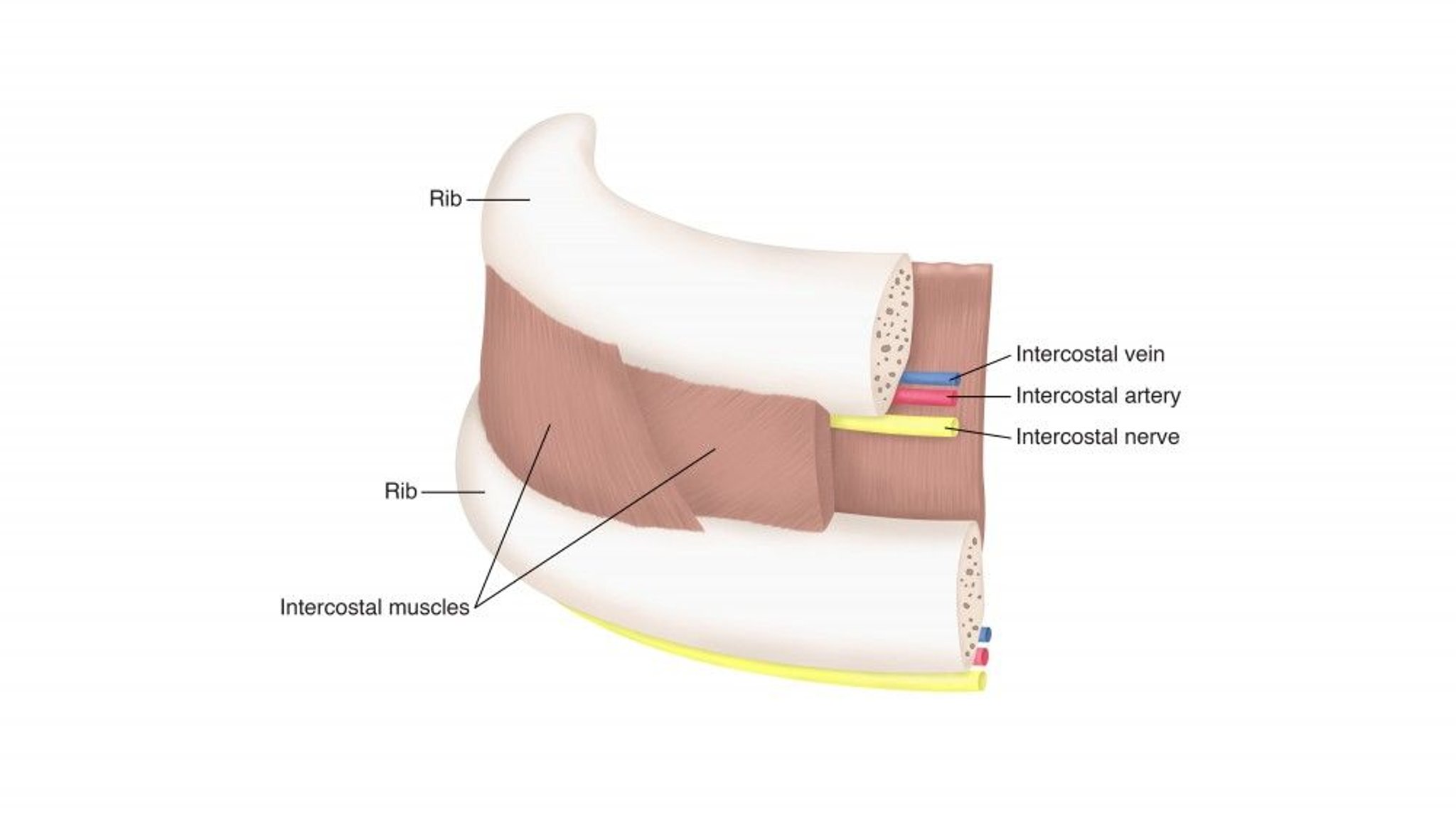
Intercostal neuralgia due to injury of the neurovascular bundle below a rib
Rarely, perforation of other structures in the chest or abdomen
Equipment for Surgical Tube and Catheter Thoracostomy
Equipment for surgical tube thoracostomy
Sterile gown, mask, eyewear, gloves, and drapes
Petroleum-based and regular gauze dressings and tape
Cleansing solution such as 2% chlorhexidine solution or povidone-iodineCleansing solution such as 2% chlorhexidine solution or povidone-iodine
25- and 21-gauge needles
10-mL and 20-mL syringes
Local anesthetic such as 1% lidocaineLocal anesthetic such as 1% lidocaine
2 Hemostats or Kelly clamps
Nonabsorbable, strong silk or nylon suture (eg, 0 or 1-0)
Scalpel (size 11 blade)
Suction apparatus
Water seal drainage apparatus and connecting tubing
Skin marking pen (optional)
Chest tube: Size ranges from 16 to 36 French (Fr) and depends on intended use (20 to 24 Fr for pneumothorax or malignant pleural effusion; 28 to 36 Fr for complicated parapneumonic effusions, empyema, and bronchopleural fistula; 32 to 36 Fr for hemothorax).
Equipment for catheter thoracostomy
Equipment required for surgical tube thoracostomy except chest tube
A ≤ 14 Fr thoracostomy catheter ("pigtail catheter")
Additional Considerations for Surgical Tube and Catheter Thoracostomy
Elective chest tube insertion is best done by a physician trained in the procedure. Other physicians can relieve a tension pneumothorax with needle thoracostomy.
Chest tube placement is an inpatient procedure. If done in the emergency department, the patient must then be admitted to the hospital.
Catheter thoracostomy is preferred for pneumothoraces or free-flowing effusions (1). However, since smaller diameter catheters are more prone to clogging and kinking, larger diameter tubes are preferred for purulent effusions and hemothoraces. The main advantages of smaller diameter catheters are less pain and the lack of need for sutures after catheter removal.
Relevant Anatomy for Surgical Tube and Catheter Thoracostomy
Neurovascular bundles are located at the lower edge of each rib. Therefore, the tube must be placed over the upper edge of the rib to avoid damage to the neurovascular bundle.

Positioning for Surgical Tube and Catheter Thoracostomy
In a patient who is breathing spontaneously, the head of the bed is elevated 30 to 60° to limit the elevation of the diaphragm that occurs during expiration and thus decrease the risk of inadvertent intra-abdominal tube placement, and liver or spleen injury.
The arm of the affected side can be placed in a position over the patient’s head or otherwise abducted and the hand placed behind the head so as to be out of the way.

Step-by-Step Description of Surgical Tube and Catheter Thoracostomy
For this procedure, a commercially available apparatus that connects to wall suction and the thoracostomy tube or catheter with plastic connectors is used. Take the water seal suction apparatus sealed with sterile water and connect it to a source of suction. Place this apparatus aside.
The insertion site can vary based on whether air or fluid is being drained. For pneumothorax, the tube is usually inserted in the fourth intercostal space, and for other indications in the fifth intercostal space, in the mid-axillary or anterior axillary line.
Mark the insertion site.
Prepare the area at and around the insertion site using an antiseptic solution such as chlorhexidine or povidone-iodine.Prepare the area at and around the insertion site using an antiseptic solution such as chlorhexidine or povidone-iodine.
Drape the area.
Inject a local anesthetic such as 1% lidocaine into the skin, subcutaneous tissue, rib periosteum (of the rib below the insertion site), and the parietal pleura. Inject a large amount of local anesthetic around the highly pain-sensitive periosteum and parietal pleura. Aspirate with the syringe before injecting lidocaine to check for blood; this step is needed to avoid injection into a blood vessel. Proper location is confirmed by return of air or fluid in the anesthetic syringe when the pleural space is entered.Inject a local anesthetic such as 1% lidocaine into the skin, subcutaneous tissue, rib periosteum (of the rib below the insertion site), and the parietal pleura. Inject a large amount of local anesthetic around the highly pain-sensitive periosteum and parietal pleura. Aspirate with the syringe before injecting lidocaine to check for blood; this step is needed to avoid injection into a blood vessel. Proper location is confirmed by return of air or fluid in the anesthetic syringe when the pleural space is entered.
Estimate how deep the tube needs to be inserted so that all of the tube’s openings are inside the pleural space, accounting for all subcutaneous and fat tissue, particularly in patients with obesity (in whom a deeper insertion may be necessary). Note or record the mark on the tube that should then be visible at the skin.
For chest tube placement ( ≥ 16 Fr):
Make a 1.5- to 2-cm skin incision, and then bluntly dissect the intercostal soft tissue down to the pleura by advancing a clasped hemostat or Kelly clamp and opening it once inside the chest wall. Identify the rib below the insertion site and move the clamp over the rib to find the pleural space above the rib. Then perforate the pleura with the clamp (usually indicated by a pop and/or sudden decrease in resistance) and open in the same way.
Insert a finger into the skin incision to manually widen the tract and confirm entry into the pleural space and ensure the absence of adhesions.
Clamp the chest tube in 2 places: one on the outside end, and one on the tip.
Insert the chest tube, with the clamp grasping the tip, through the tract and direct it inferoposteriorly for effusions, or apically for a pneumothorax, until all of the tube’s openings are inside the chest wall.
For chest catheter placement (≤ 14 Fr):
Insert the needle along the upper border of the rib while aspirating and advance it into the effusion or pneumothorax.
When fluid or air is aspirated, remove the syringe from the needle and pass the guidewire deep enough to clear the needle.
Remove the needle, leaving the guidewire in place.
Make a skin nick using a scalpel.
Pass the dilator over the guidewire and into the pleural space and remove the dilator.
Place the catheter and its trocar over the guidewire, making sure that the last side-hole is within the pleural space.
Remove both the trocar and guidewire.
For both chest tube and catheter, after placement:
Suture the chest tube to the skin of the chest wall using one of many suture methods. One way is to use a purse-string suture. In addition, place an interrupted suture next to the tube across the incision and tie the suture around the tube. Another method is to substitute a second interrupted suture across the incision on the other side of the tube for the purse string suture and tie that suture to the tube as well.
Place a sterile dressing with petroleum gauze to help seal the wound over the site.
Cut 2 sterile gauze pads halfway across and place them around the tube.
Remove the draping.
Tape the dressing in place using pressure dressings. To increase stability, consider taping the outside part of the tube to the dressing or the patient separately.
Connect the tube or catheter to the water seal suction apparatus to prevent air from entering the chest through the tube and to allow drainage with or without suction. Gravity assists drainage without suction.
Aftercare for Surgical Tube and Catheter Thoracostomy
An anteroposterior chest radiograph should be obtained at the bedside to check the tube’s position. If there are concerns about positioning or functioning of the chest tube, posteroanterior and lateral radiographs or chest CT should be done.
The chest tube is removed when the condition for which it was placed resolves. With a pneumothorax, suction is stopped and the tube is placed on just water seal for several hours to ensure that the air leak has stopped and that the lung remains expanded. Chest radiograph is often repeated 12 to 24 hours after the last evidence of an air leak before removing the tube. For pleural effusions or hemothorax, the tube is typically removed when the drainage is < 100 to 200 mL/day of serous fluid.
Removal of a chest tube in patients on mechanical ventilation, especially those with high oxygen requirements, positive pressure ventilation, chronic lung disease, or increased risk of recurrent pneumothorax, should be done only after consultation with a pulmonary specialist.
To remove the tube, the patient should be semi-erect. After removal of the sutures, at the moment of removal, the patient is asked to take a deep breath and then to forcibly exhale; the tube is removed during exhalation and the site is covered with petroleum gauze, a sequence that reduces the chance of pneumothorax during removal.
The purse-string suture, if inserted during tube insertion, is closed, and/or additional sutures may be needed to close the incision.
A chest radiograph should be done several hours after chest tube removal. If no pneumothorax is seen on the radiograph after chest tube removal, there is no need for further chest radiographs except as dictated by clinical changes in the patient's condition.
Warnings and Common Errors for Surgical Tube and Catheter Thoracostomy
Do not use a small chest catheter (≤ 14 Fr) if there is a bloody effusion because clots can clog the catheter.
The water seal suction apparatus must be kept 100 cm (40 inches) below the patient to avoid retrograde flow of fluid or air back into the pleural space.
Some clinicians recommend withdrawing no more than 1.5 L of pleural fluid in 24 hours due to a concern about causing re-expansion pulmonary edema. However, there is little evidence that the risk of re-expansion pulmonary edema is directly proportional to the volume of fluid removed (2). Thus, in properly monitored patients, it may be reasonable for experienced operators to completely drain effusions that have not been long-standing.
If the chest radiograph shows that the chest tube is not far enough into the chest and the aspiration holes in the tube are not in the chest cavity, the chest tube will need to be replaced. Simply advancing the chest tube can introduce non-sterile tubing into the chest.
Common insertion errors include inadequate quantities of local anesthetic and an initial incision that is too small.
Lock the stretcher before inserting the tube because insertion may take significant force and move the stretcher.
Tips and Tricks for Surgical Tube and Catheter Thoracostomy
Conscious sedation prior to the procedure can be used in selected cases (eg, pediatric patients or patients who are anxious, uncooperative, or require pain relief due to chronic pain).
When marking the insertion point, use a skin marking pen or make an impression with a pen so that the skin cleansing preparation will not remove the mark.
References
1. Tran J, Haussner W, Shah K: Traumatic Pneumothorax: A Review of Current Diagnostic Practices And Evolving Management. J Emerg Med 61(5):517–528, 2021. doi:10.1016/j.jemermed.2021.07.006
2. Feller-Kopman D, Berkowitz D, Boiselle P, et al: Large-volume thoracentesis and the risk of reexpansion pulmonary edema. Ann Thoracic Surg 84:1656–1662, 2007.







