


Osteoarthritis is a chronic arthropathy characterized by disruption and potential loss of joint cartilage along with other joint changes, including bone hypertrophy (periarticular osteophyte formation and sclerosis). Symptoms include gradually developing pain aggravated or triggered by activity, stiffness lasting < 30 minutes on awakening and after inactivity, and occasional joint swelling. Diagnosis is confirmed by radiographs. Treatment includes joint protection, rehabilitation with muscle strengthening, and medications to reduce pain.

Osteoarthritis, the most common joint disorder, often becomes symptomatic in the 40s and 50s and is nearly universal (although not always symptomatic) by age 80. Only half of patients with pathologic changes of osteoarthritis have symptoms (1). Below age 40, most large-joint osteoarthritis occurs in men and often results from trauma or anatomic variation (eg, hip dysplasias). Women predominate from age 40 to 70, after which men and women are equally affected (2).

References
1. Hannan MT, Felson DT, Pincus T. Analysis of the discordance between radiographic changes and knee pain in osteoarthritis of the knee. J Rheumatol. 2000;27(6):1513-1517.
2. Allen KD, Thoma LM, Golightly YM. Epidemiology of osteoarthritis. Osteoarthritis Cartilage. 2022;30(2):184-195. doi:10.1016/j.joca.2021.04.020
Classification of Osteoarthritis
Osteoarthritis is classified as primary (idiopathic) or secondary to some known cause.
Primary osteoarthritis may be localized to specific joints (eg, hands, knee, hip). If primary osteoarthritis involves multiple joints, it is classified as generalized osteoarthritis.
Secondary osteoarthritis results from conditions that change the microenvironment of the cartilage or joint structure. These conditions include significant trauma, congenital joint abnormalities, metabolic defects (eg, hemochromatosis, Wilson disease), infections (causing postinfectious arthritis), endocrine and neuropathic diseases, and disorders that alter the normal structure and function of hyaline cartilage (eg, rheumatoid arthritis, psoriatic arthritis, calcium crystal deposition disease).
Pathophysiology of Osteoarthritis
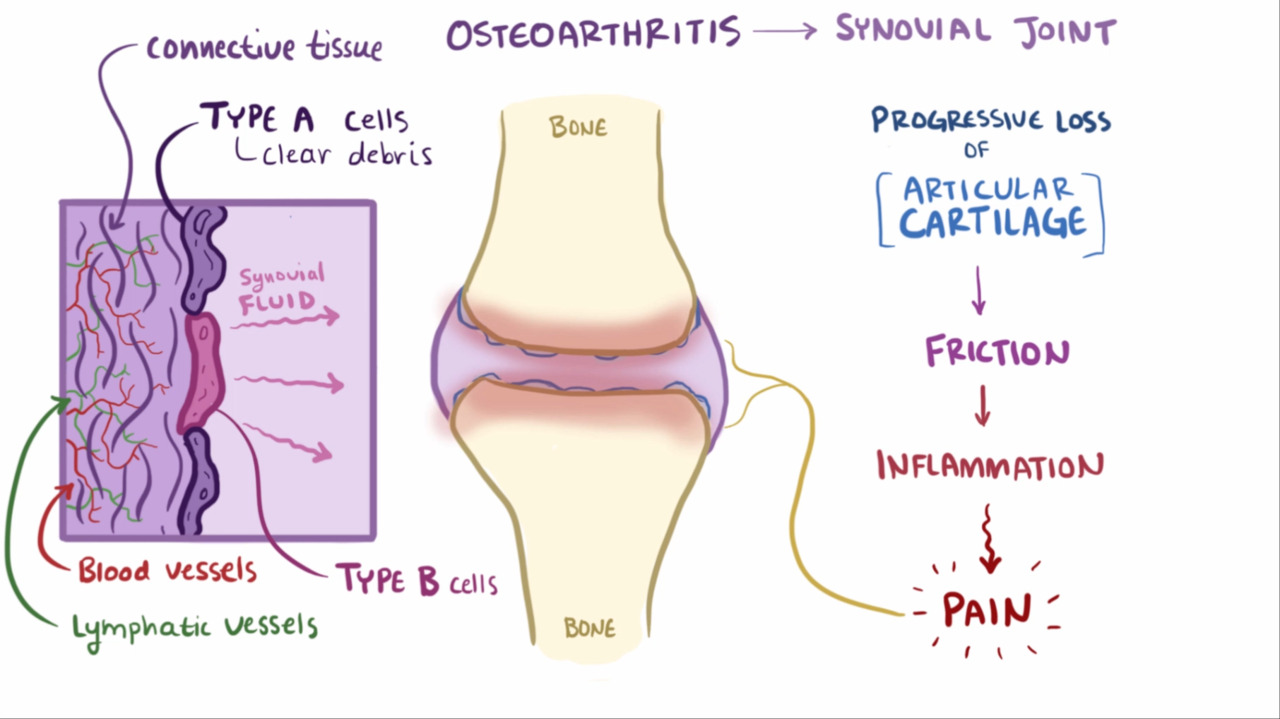
Normal joints have little friction with movement and do not wear out with typical use, overuse, or most trauma. Hyaline cartilage is avascular, aneural, and alymphatic. It is 95% water and extracellular cartilage matrix and only 5% chondrocytes. Chondrocytes have the longest cell cycle in the body (similar to central nervous system and muscle cells). Cartilage health and function depend on compression and release from weight bearing and use (ie, compression pumps fluid from the cartilage into the joint space and into capillaries and venules, whereas release allows the cartilage to reexpand, hyperhydrate, and absorb necessary electrolytes and nutrients).
The trigger of osteoarthritis is most often unknown, but osteoarthritis sometimes begins with abnormal mechanics from an injury (eg, torn meniscus), transmission of inflammatory mediators from the synovium into cartilage, or defects in cartilage metabolism. Obesity triggers some of these defects in cartilage metabolism, leading to cartilage matrix damage and subchondral bone remodeling mediated by adipokines, such as leptin and adipsin, and compounded by mechanical factors due to excess weight. The tissue damage stimulates chondrocytes to attempt repair, which increases production of proteoglycans and collagen. However, efforts at repair also stimulate the enzymes that degrade cartilage, as well as inflammatory cytokines, which are normally present in small amounts. Inflammatory mediators trigger an inflammatory cycle that further stimulates the chondrocytes and synovial lining cells, eventually breaking down the cartilage. Chondrocytes undergo programmed cell death (apoptosis). Once cartilage is destroyed, exposed bone becomes eburnated and sclerotic.
All articular and some periarticular tissues can become involved in osteoarthritis. Subchondral bone stiffens, then undergoes infarction, and develops subchondral cysts. Attempts at bony repair cause subchondral sclerosis and osteophytes at the joint margins. The osteophytes seem to develop in an attempt to stabilize the joint. Cartilage may initially become hypertrophic but then deteriorates. The synovium becomes mildly inflamed and thickened and produces synovial fluid with less viscosity and greater volume. Periarticular tendons and ligaments become stressed, resulting in tendinitis and contractures. As the joint becomes less mobile, surrounding muscles weaken and become less supportive. Knee menisci, which are innervated, fissure and may fragment and contribute to the pain.
Osteoarthritis of the spine can, at the disc level, cause marked thickening and proliferation of the posterior longitudinal ligaments, which are posterior to the vertebral body but anterior to the spinal cord. The result can be transverse bars that encroach on the anterior spinal cord. Hypertrophy and hyperplasia of the ligamenta flava, which are posterior to the spinal cord, often compress the posterior canal, causing lumbar spinal stenosis. In contrast, the anterior and posterior nerve roots, ganglia, and common spinal nerve are relatively well protected in the intervertebral foramina, where they occupy only 25% of the available and well-cushioned space.
Symptoms and Signs of Osteoarthritis
Onset of osteoarthritis is most often gradual, usually beginning with one or a few joints.
Pain is the earliest symptom of osteoarthritis, sometimes described as a deep ache. Pain is usually worsened by weight bearing and relieved by rest but can eventually become constant.
Stiffness follows awakening or inactivity but lasts < 30 minutes and lessens with movement. As osteoarthritis progresses, joint motion becomes restricted, and tenderness and crepitus or grating sensations develop. In larger joints, particularly the knees, joint effusions are common. Synovial fluid is usually noninflammatory (ie, ≤ 2000 WBC/mcL).
Flexion contractures may develop. Acute or severe synovitis is rare.


By permission of the publisher. From Myers S: Atlas of Rheumatology. Edited by G Hunder. Philadelphia, Current Medicine, 2005.
Tenderness on palpation and pain on passive motion are relatively late signs. Muscle spasm and contracture add to the pain. Mechanical block by intra-articular loose bodies or displaced or torn menisci can occur and cause locking or catching. Deformity and subluxations can also develop.
Osteoarthritis is usually sporadically progressive but occasionally, with no predictability, stops.
The joints most often affected by osteoarthritis include the following:
Distal interphalangeal (DIP) and proximal interphalangeal (PIP) joints (causing Heberden and Bouchard nodes, respectively)
Thumb carpometacarpal joint (the most commonly painful hand joint)
Intervertebral disks and zygapophyseal joints in the cervical and lumbar vertebrae
First metatarsophalangeal joint
Hip
Knee


© Springer Science+Business Media
Cervical and lumbar spinal osteoarthritis may lead to myelopathy or radiculopathy. However, the clinical signs of myelopathy are usually mild. Lumbar spinal stenosis may cause lower back or leg pain that is worsened by walking (neurogenic claudication, sometimes called pseudoclaudication) or back extension. Radiculopathy can be prominent but is less common because the nerve roots and ganglia are well protected. Insufficiency of the vertebral arteries, infarction of the spinal cord, and dysphagia due to esophageal impingement by cervical osteophytes occasionally occur. Symptoms and signs caused by osteoarthritis in general may also derive from subchondral bone, ligamentous structures, synovium, periarticular bursae, capsules, muscles, tendons, disks, and periosteum, all of which are pain sensitive. Venous pressure may increase within the subchondral bone marrow and cause pain (sometimes called bone angina).


DR P. MARAZZI/SCIENCE PHOTO LIBRARY
Hip osteoarthritis causes gradual loss of range of motion and is most often symptomatic during weight-bearing activities or full rotation (eg, as when putting on socks or entering vehicles). Pain may be felt in the inguinal area or greater trochanter or referred to the thigh and knee.
Knee osteoarthritis causes cartilage to be lost (medial loss occurs in the majority of cases). The ligaments become lax and the joint becomes less stable, with local pain arising from the ligaments and tendons.
Hand osteoarthritis causes joint space narrowing accompanied by pain, stiffness, and functional limitations. Synovitis may be observed. Hand osteoarthritis primarily affects the DIP joints, PIP joints, and, the thumb carpometacarpal joints. The 2nd and 3rd metacarpophalangeal joints are less commonly involved, but the wrists are relatively spared. Nodal osteoarthritis is characterized by Heberden and Bouchard nodes. Erosive osteoarthritis is characterized by severe, erosive lesions observed on radiograph. At this time, it is uncertain whether erosive osteoarthritis is a variant of hand osteoarthritis or whether it represents a separate entity, such as microcrystalline disease (eg, calcium pyrophosphate arthritis).


Image courtesy of Kinanah Yaseen, MD.
Diagnosis of Osteoarthritis
Radiographs


By permission of the publisher. From Myers S: Atlas of Rheumatology. Edited by G Hunder. Philadelphia, Current Medicine, 2005.
Osteoarthritis should be suspected in patients with gradual onset of symptoms and signs, particularly in older adults. If osteoarthritis is suspected, radiographs should be taken of the most symptomatic joints. Radiographs generally reveal marginal osteophytes, narrowing of the joint space, increased density of the subchondral bone, subchondral cyst formation, bony remodeling, and sometimes joint effusions. Standing weight-bearing Merchant view (tangential view with knee flexed 30°) radiographs of the knees are more sensitive in detecting joint space narrowing. Discrepancy between severity of symptoms and severity of changes in imaging is common (1).

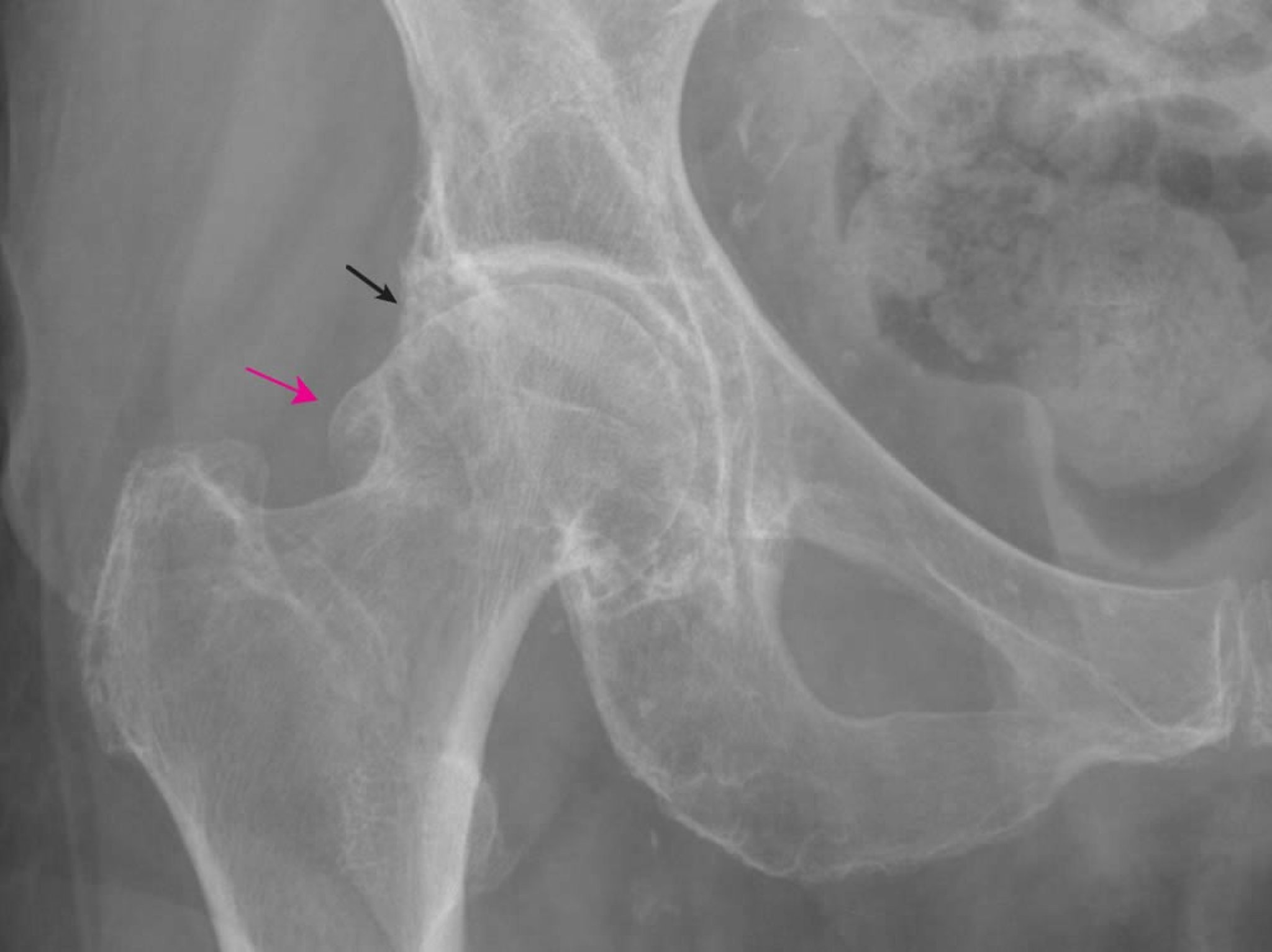
Image provided by Roy Altman, MD.
Laboratory studies are normal in osteoarthritis but occasionally may be required to rule out other disorders or to diagnose an underlying disorder causing secondary osteoarthritis. If osteoarthritis causes joint effusions, synovial fluid analysis can help differentiate it from inflammatory arthritides; in osteoarthritis, synovial fluid is usually clear, viscous, and has ≤ 2000 WBC/mcL.
Osteoarthritis with significant involvement outside the usual joints (eg, metacarpophalangeal [MCP] joint, ankle) suggests secondary osteoarthritis; further evaluation may be required to determine the underlying primary disorder (eg, endocrine, metabolic, neoplastic, or biomechanical disorder).
Diagnosis reference
1. Bijsterbosch J, Watt I, Meulenbelt I, et al: Clinical and radiographic disease course of hand osteoarthritis and determinants of outcome after 6 years. Ann Rheum Dis 70(1):68-73, 2011. doi:10.1136/ard.2010.133017
Treatment of Osteoarthritis
Nonpharmacologic therapy (eg, education, appropriate weight loss, rehabilitative and supportive measures)
Pharmacologic therapy
Osteoarthritis treatment goals are relieving pain, maintaining joint flexibility, and optimizing joint and overall function. Primary treatments include physical measures that involve rehabilitation; support devices; exercise for strength, flexibility, and endurance; patient education; and modifications in activities of daily living. Adjunctive therapies include pharmacologic treatment and surgery. (See also the 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee for nonpharmacologic management of hip and knee osteoarthritis.)
Physical measures
Moderate weight loss in patients with overweight often reduces pain and may even reduce progression of knee osteoarthritis (1). Rehabilitation techniques are best begun before disability develops.
Exercises (range of motion, isometric, isotonic, isokinetic, postural, strengthening—see Physical Therapy) maintain range of motion and increase the capacity for tendons and muscles to absorb stress during joint motion. Exercise may slow the disease progression and improve joint symptoms, mobility, and quality of life in patients with knee and/or hip osteoarthritis (2, 3). Although there is insufficient evidence to recommend one specific exercise regimen over another, aquatic exercises are particularly useful for patients with more severe pain and functional limitations who may benefit from lower impact exercise. Stretching exercises should be done daily.
Immobilization for any prolonged period of time can promote contractures and worsen the clinical course. However, a few minutes of rest (every 4 to 6 hours in the daytime) is reasonable if balanced with exercise and use.
Modifying activities of daily living can help. For example, a patient with lumbar spine, hip, or knee osteoarthritis should avoid soft deep chairs and recliners in which posture is poor and from which rising is difficult. The regular use of pillows under the knees while reclining encourages contractures and should also be avoided. However, pillows placed between the knees can often help relieve radicular back pain. Patients should sit in straight-back chairs without slumping, sleep on a firm bed (perhaps with a bed board), use a car seat shifted forward and designed for comfort, do postural exercises, wear well-supported shoes or athletic shoes, and continue employment and physical activity.
In osteoarthritis of the spine, knee, or thumb carpometacarpal joint, various supports can relieve pain and increase function, but to preserve flexibility, they should be accompanied by specific exercise programs. For medial knee osteoarthritis, orthoses designed to reduce knee load are preferred to lateral wedge insoles, which have yielded equivocal outcomes (4).
Pharmacologic therapy
Pharmacologic therapy is an adjunct to the physical program.
Nonsteroidal anti-inflammatory drugs (NSAIDs) are the mainstay of pharmacologic therapy for osteoarthritis. Topical medications are preferred as initial therapy for knee and hand joints (ie, superficial joints) given their possible efficacy and limited systemic exposure, thereby minimizing the risk of adverse drug effects (5). Oral NSAIDs, including selective cyclooxygenase-2 (COX-2) inhibitors (coxibs), may be considered if patients have refractory pain or signs of inflammation (eg, erythema, warmth); they should be used for the shortest possible duration given the risk of potential adverse gastrointestinal, cardiovascular, and renal effects. Gastric protection should be considered when using NSAIDs in older adults.
Topical capsaicinTopical capsaicin may be helpful in relieving pain in superficial joints (eg, knees and hands) by disrupting pain transmission (6). However, it is mainly used for knee rather than hand osteoarthritis because of the lack of direct evidence for hand osteoarthritis and the increased risk of contamination of the eyes (when applied to the hands).
DuloxetineDuloxetine, a serotonin norepinephrine reuptake inhibitor, may modestly reduce pain caused by osteoarthritis (, a serotonin norepinephrine reuptake inhibitor, may modestly reduce pain caused by osteoarthritis (7). It may be used for patients who have not responded adequately to NSAIDs or have contraindications preventing their use.
AcetaminophenAcetaminophen may be tried in patients without hepatic disease or considerable alcohol intake who do not tolerate other therapies. Its use, however, should be limited based on evidence suggesting negligible effects on pain (8).
Intra-articular depot corticosteroids can provide short-term pain relief in some patients (9); however, a strong placebo effect has been shown in clinical trials. Frequently administered intra-articular injections of corticosteroids increase the risk of cartilage loss (10). There is generally no role for systemic corticosteroids in the treatment of osteoarthritis, although some patients report decreased pain when taking corticosteroids for other reasons.
More potent analgesics, such as tramadol or rarely other opioids, have few benefits in the management of noncancerous disorders and a high risk of adverse effects (More potent analgesics, such as tramadol or rarely other opioids, have few benefits in the management of noncancerous disorders and a high risk of adverse effects (11); thus, their use should generally be avoided.
Surgery
Laminectomy, osteotomy, and total joint replacement should be considered if nonsurgical approaches fail.
Other adjunctive and investigational therapies
Various adjunctive measures are available for the treatment of osteoarthritis, but their routine use is not recommended due to limited evidence of their efficacy. However, some may reasonably be tried, particularly for patients with refractory symptoms, after consideration of other factors, such as personal preferences, potential harms, and cost.
Some therapies that may reduce pain include massage, heating pads, and acupuncture.
Intraarticular hyaluronic acid formulations have been used to treat knee osteoarthritis refractory to other measures. However, efficacy of these formulations in patients with knee osteoarthritis is limited and may not be clinically meaningful (12); therefore, they are not recommended unless all other options have failed to provide benefit. Hyaluronic acid formulations are not recommended in hip or shoulder osteoarthritis (13). In some patients, local injection can cause an acute severe inflammatory synovitis. Randomized trials have shown a strong placebo effect of any intraarticular injection for the treatment of osteoarthritis (14). These injections have no demonstrated disease-modifying effect.
Intraarticular platelet-rich plasma injections are not routinely recommended given the lack of evidence of efficacy compared with intraarticular hyaluronic acid, corticosteroid, or saline injections (15).
Glucosamine sulfate 1500 mg orally once a day has been suggested to relieve pain and slow joint deterioration; chondroitin sulfate 1200 mg once a day has also been suggested for pain relief. Studies to date have shown mixed efficacy in terms of pain relief, with onset of pain relief often delayed, and no strong effect on preservation of cartilage (16, 17). The use of other nutritional supplements, such as curcumin (turmeric) and Boswellia serrata, are not routinely recommended because robust evidence of benefit is lacking (18). These supplements, however, are reasonable to try if patients are interested in doing so and are able achieve pain relief. Flavocoxid, a plant-derived compound, should not be used because serious liver injury has been reported (19).
Transcutaneous electrical nerve stimulation (TENS) is not recommended for knee osteoarthritis based on randomized trials that suggest a lack of benefit (20).
It is not clear whether using a topical lidocaine 5% patch relieves pain. It is not clear whether using a topical lidocaine 5% patch relieves pain.
Experimental therapies that may preserve cartilage or allow chondrocyte grafting are being studied. Mesenchymal stem cell therapy for cartilage repair is claimed to yield positive outcomes, especially in knee osteoarthritis (21), but this approach is still considered experimental, with scant evidence supporting its clinical use (22). Monoclonal antibodies against nerve growth factor are being studied for chronic pain due to osteoarthritis. However, several trials resulting in accelerated osteoarthritis and osteonecrosis have limited the development of these agents (23).
Treatment references
1. Messier SP, Resnik AE, Beavers DP, et al: Intentional weight loss in overweight and obese patients with knee osteoarthritis: Is more better?. Arthritis Care Res (Hoboken) 70(11):1569-1575, 2018. doi:10.1002/acr.23608
2. Juhl C, Christensen R, Roos EM, et al: Impact of exercise type and dose on pain and disability in knee osteoarthritis: a systematic review and meta-regression analysis of randomized controlled trials. Arthritis Rheumatol 66(3):622-636, 2014. doi:10.1002/art.38290
3. Lo GH, Vinod S, Richard MJ, et al: Association Between Walking for Exercise and Symptomatic and Structural Progression in Individuals With Knee Osteoarthritis: Data From the Osteoarthritis Initiative Cohort. Arthritis Rheumatol. 2022;74(10):1660-1667. doi:10.1002/art.42241
4. Parkes MJ, Maricar N, Lunt M, et al: Lateral wedge insoles as a conservative treatment for pain in patients with medial knee osteoarthritis: a meta-analysis. JAMA 310(7):722–730, 2013. doi:10.1001/jama.2013.243229
5. Derry S, Conaghan P, Da Silva JA, et al: Topical NSAIDs for chronic musculoskeletal pain in adults. Cochrane Database Syst Rev 4(4):CD007400, 2016. Published 2016 Apr 22. doi:10.1002/14651858.CD007400.pub3
6. De Silva V, El-Metwally A, Ernst E, Lewith G, Macfarlane GJ; Arthritis Research UK Working Group on Complementary and Alternative Medicines: Evidence for the efficacy of complementary and alternative medicines in the management of osteoarthritis: a systematic review. Rheumatology (Oxford) 50(5):911-920, 2011. doi:10.1093/rheumatology/keq379
7. Wang ZY, Shi SY, Li SJ, et al: Efficacy and safety of duloxetine on osteoarthritis knee pain: a meta-analysis of randomized controlled trials. Pain Med 16(7):1373-1385, 2015. doi:10.1111/pme.12800
8. Machado GC, Maher CG, Ferreira PH, et al: Efficacy and safety of paracetamol for spinal pain and osteoarthritis: systematic review and meta-analysis of randomised placebo controlled trials. BMJ. 2015;350:h1225. Published 2015 Mar 31. doi:10.1136/bmj.h1225
9. Jüni P, Hari R, Rutjes AW, et al: Intra-articular corticosteroid for knee osteoarthritis. Cochrane Database Syst Rev 2015(10):CD005328, 2015. Published 2015 Oct 22. doi:10.1002/14651858.CD005328.pub3
10. McAlindon TE, LaValley MP, Harvey WF, et al: Effect of intra-articular triamcinolone vs saline on knee cartilage volume and pain in patients with knee osteoarthritis: randomized clinical trial. JAMA 317(19):1967–1975, 2017. doi:10.1001/jama.2017.5283
11. Busse JW, Wang L, Kamaleldin M, et al: Opioids for chronic noncancer pain: a systematic review and meta-analysis. JAMA 320(23):2448-2460, 2018. doi:10.1001/jama.2018.18472
12. Jevsevar D, Donnelly P, Brown GA, Cummins DS. Viscosupplementation for osteoarthritis of the knee: a systematic review of the evidence. J Bone Joint Surg Am 97(24):2047-2060, 2015. doi:10.2106/JBJS.N.00743
13. Kolasinski SL, Neogi T, Hochberg MC, et al: 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Care Res (Hoboken) 72(2):149–162, 2020. doi:10.1002/acr.24131
14. Previtali D, Merli G, Di Laura Frattura G, et al: The long-lasting effects of "placebo injections" in knee osteoarthritis: a meta-analysis. Cartilage 13(1_suppl):185S-196S, 2021. doi:10.1177/1947603520906597
15. Costa LAV, Lenza M, Irrgang JJ, Fu FH, Ferretti M: How does platelet-rich plasma compare clinically to other therapies in the treatment of knee osteoarthritis? A systematic review and meta-analysis. Am J Sports Med 51(4):1074-1086, 2023. doi:10.1177/03635465211062243
16. Eriksen P, Bartels EM, Altman RD, et al: Risk of bias and brand explain the observed inconsistency in trials on glucosamine for symptomatic relief of osteoarthritis: a meta-analysis of placebo-controlled trials. Arthritis Care Res (Hoboken) 66(12):1844-1855, 2014. doi:10.1002/acr.22376
17. Lee YH, Woo JH, Choi SJ, Ji JD, Song GG: Effect of glucosamine or chondroitin sulfate on the osteoarthritis progression: a meta-analysis. Rheumatol Int 30(3):357-363, 2010. doi:10.1007/s00296-009-0969-5
18. Liu X, Machado GC, Eyles JP, Ravi V, Hunter DJ: Dietary supplements for treating osteoarthritis: a systematic review and meta-analysis. Br J Sports Med 52(3):167-175, 2018. doi:10.1136/bjsports-2016-097333
19. Chalasani N, Vuppalanchi R, Navarro V, et al: Acute liver injury due to flavocoxid (Limbrel), a medical food for osteoarthritis: a case series. Ann Intern Med 156(12):857-W300, 2012. doi:10.7326/0003-4819-156-12-201206190-00006
20. Reichenbach S, Jüni P, Hincapié CA, et al: Effect of transcutaneous electrical nerve stimulation (TENS) on knee pain and physical function in patients with symptomatic knee osteoarthritis: the ETRELKA randomized clinical trial. Osteoarthritis Cartilage 30(3):426-435, 2022. doi:10.1016/j.joca.2021.10.015
21. Yubo M, Yanyan L, Li L, et al: Clinical efficacy and safety of mesenchymal stem cell transplantation for osteoarthritis treatment: a meta-analysis. PLoS ONE 12(4):e0175449, 2017. doi: 10.1371/journal.pone.0175449. eCollection 2017
22. Pas HI, Winters M, Haisma HJ, et al: Stem cell injections in knee osteoarthritis: a systematic review of the literature. Br J Sports Med 51(15):1125–1133, 2017. doi:10.1136/bjsports-2016-096793
23. Sanga P, Katz N, Polverejan E, et al: Long-term safety and efficacy of fulranumab in patients with moderate-to-severe osteoarthritis pain: a phase II randomized, double-blind, placebo-controlled extension study. Arthritis Rheumatol 69(4):763-773, 2017. doi:10.1002/art.39943
Key Points
Osteoarthritis, the most common joint disorder, becomes particularly common with aging.
Key pathophysiologic features include disruption and loss of joint cartilage and bony hypertrophy.
Osteoarthritis can affect particular joints (sometimes secondary to injury or another joint problem) or be generalized.
Symptoms include gradual onset of joint pain that is worsened by weight-bearing or mechanical stress and relieved by rest, and stiffness that lessens with activity.
Confirm the diagnosis with radiographic findings such as marginal osteophytes, narrowing of the joint space, increased density of the subchondral bone, bony remodeling, and sometimes subchondral cyst formation and joint effusion.
Discrepancy between severity of symptoms and severity of changes on imaging is common.
Treat primarily with physical measures that involve rehabilitation; support devices; exercise for strength, flexibility, and endurance; patient education; and modifications in activities of daily living.
Treat adjunctively with medications (eg, nonsteroidal anti-inflammatory drugs, duloxetine) and surgery.Treat adjunctively with medications (eg, nonsteroidal anti-inflammatory drugs, duloxetine) and surgery.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
European League Against Rheumatism: EULAR Recommendations for the Management of Rheumatoid Arthritis with Synthetic and Biological Disease-Modifying Antirheumatic Drugs: 2019 Update
Sharma L: Osteoarthritis of the knee. N Engl J Med 2021 Jan 7;384(1):51-59. doi: 10.1056/NEJMcp1903768







