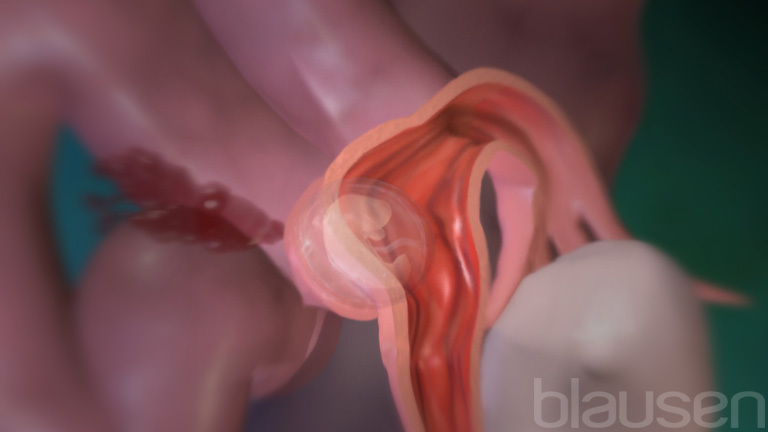
Ectopic pregnancy is attachment (implantation) of a fertilized egg in an abnormal location, such as a fallopian tube.
Topic Resources


In an ectopic pregnancy, the fetus cannot survive.
Women with an ectopic pregnancy often have vaginal bleeding and abdominal pain starting in the first trimester.
An ectopic pregnancy needs immediate medical care, because if an ectopic pregnancy continues to grow, it may rupture (burst open) the part of the body where it is implanted (such as a fallopian tube), causing severe bleeding that can be fatal to the pregnant woman.
Doctors base the diagnosis on results of ultrasonography to determine the location of the fetus and blood tests; often, tests need to be repeated over several days.
Usually, an ectopic pregnancy can be treated with one or more doses of a medication (methotrexate), or sometimes surgery is necessary.Usually, an ectopic pregnancy can be treated with one or more doses of a medication (methotrexate), or sometimes surgery is necessary.
After an egg is released by the ovary (ovulation), it becomes fertilized if it comes into contact with sperm. Fertilization usually happens in the fallopian tube. The fertilized egg then travels through the fallopian tube, enters the uterus, and becomes implanted in the wall of the uterus. However, if the tube is narrowed or blocked, the fertilized egg may not be able to reach the uterus. Sometimes the fertilized egg then implants in tissues outside of the uterus, resulting in an ectopic pregnancy. Ectopic pregnancies most commonly implant in one of the fallopian tubes (this is called a tubal pregnancy) but may implant in other locations (such as the ovary or cervix).
An ectopic pregnancy usually starts to develop, but growth is abnormal and development slows down or stops. Because tissues outside the uterus cannot provide the necessary blood supply and support, the fetus does not survive.
As an ectopic pregnancy grows, it may rupture (burst open) the structure (part of the body) where it is implanted, such as a fallopian tube. The structure containing the ectopic pregnancy typically ruptures after about 6 to 16 weeks. When an ectopic pregnancy ruptures, bleeding may be severe and even threaten the life of the woman. The later the structure ruptures, the worse the blood loss, and the higher the risk of death for the pregnant woman. However, if an ectopic pregnancy is detected before it ruptures, it can usually be treated safely.
Ectopic pregnancy occurs in about 1 to 2% of pregnancies.
Risk factors (conditions that increase the risk of a disorder) that are highest risk for an ectopic pregnancy include
Prior ectopic pregnancy
Prior pelvic surgery, particularly fallopian tube surgery, including tubal sterilization (also called tubal ligation or tying the tubes)
Fallopian tube abnormalities or damage (for example, from an infection or surgery)
Assisted reproductive technologies (fertility treatments) used during the current pregnancy
Other risk factors for ectopic pregnancy include
Previous pelvic inflammatory disease or sexually transmitted infections (particularly infection due to Chlamydia trachomatis)
Cigarette smoking
Usually, people who have had tubal sterilization or have an intrauterine device (IUD) in place do not become pregnant, because these are effective methods of birth control. In rare cases, when pregnancy does occur in these people, the risk of ectopic pregnancy is increased.
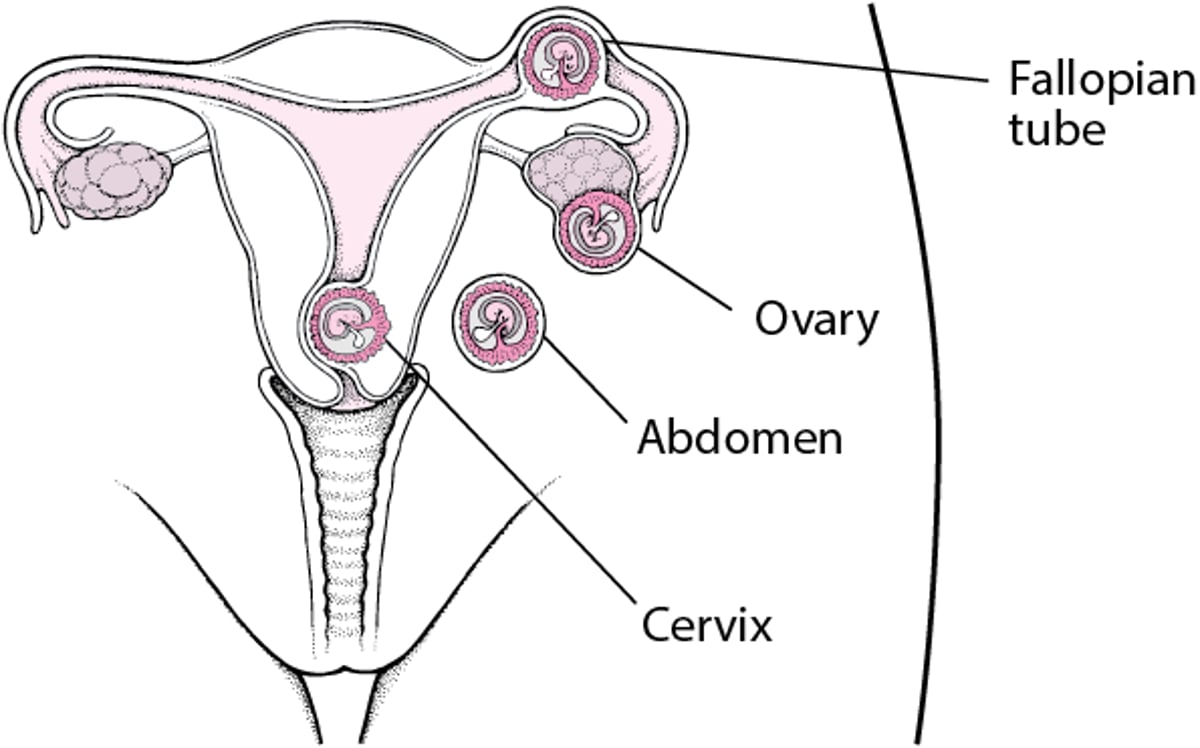
Ectopic Pregnancy: A Mislocated Pregnancy
Normally, an egg is fertilized in the fallopian tube and becomes implanted in the uterus. However, if the tube is narrowed or blocked, the egg may move slowly or become stuck in the fallopian tube. The fertilized egg may never reach the uterus, resulting in an ectopic (mislocated) pregnancy. An ectopic pregnancy may be located in many different places, including a fallopian tube, an ovary, the cervix, and the abdomen. |

Symptoms of Ectopic Pregnancy
Symptoms of ectopic pregnancy vary and may not occur until the structure containing the ectopic pregnancy ruptures. Most women have vaginal bleeding or spotting and/or lower abdominal pain, which may be dull, sharp, or crampy. Some women may think the bleeding is a menstrual period and so may not suspect that they are pregnant.
If the part of the female anatomy where the ectopic pregnancy is located ruptures, the woman usually feels sudden, severe, constant pain in the lower abdomen. Women with severe blood loss may feel light-headed or may faint. These symptoms may indicate that so much blood has been lost that blood pressure is dangerously low (shock). Peritonitis (inflammation of the membrane that lines the abdominal cavity) may also develop.
Diagnosis of Ectopic Pregnancy
A pregnancy test
Ultrasonography
Blood tests
Sometimes laparoscopy
Because a ruptured ectopic pregnancy can be life-threatening for a pregnant woman, prompt diagnosis is essential.
Doctors suspect an ectopic pregnancy in a woman who is pregnant or might be pregnant and if she has lower abdominal pain or vaginal bleeding. If an ectopic pregnancy ruptures, a woman may faint or go into shock. A pregnancy test is done to check if the symptoms are related to pregnancy.
If a pregnancy test is positive or, rarely, if the test is negative but symptoms still suggest ectopic pregnancy, ultrasonography is done using a device inserted into the vagina (called transvaginal ultrasonography). For a normal pregnancy, the fetus is in the uterus. If ultrasonography detects a fetus in a location other than the uterus, the diagnosis of ectopic pregnancy is confirmed. Early in pregnancy, ultrasonography often does not detect a fetus anywhere, because the pregnancy is too early to be seen. Ultrasonography is then repeated, usually about every 1 to 2 weeks until the location of the pregnancy can be confirmed. In the meantime, doctors monitor women closely to make sure that symptoms are not getting worse.
Doctors also do blood tests to measure the level of a hormone produced by the placenta early in pregnancy called human chorionic gonadotropin (hCG). A diagnosis of ectopic pregnancy cannot be made by measuring hCG just once; hCG is usually measured every 2 days until an ectopic pregnancy can be confirmed or another reason for the symptoms is identified. The hCG level in the blood normally increases fairly rapidly during pregnancy. If hCG levels do not increase as expected or if they decrease, an ectopic pregnancy (or miscarriage) is likely.
If needed to confirm the diagnosis, doctors may use a viewing tube called a laparoscope, inserted through a small incision just below the navel. This procedure enables them to view an ectopic pregnancy directly.
Treatment of Ectopic Pregnancy
Usually, a medication (methotrexate) for small, unruptured ectopic pregnanciesUsually, a medication (methotrexate) for small, unruptured ectopic pregnancies
Sometimes, surgery
An ectopic pregnancy must be treated as soon as possible to save the life of the pregnant woman.
Small ectopic pregnancies that have not ruptured may be treated with one dose of the medication methotrexate, given by injection. Methotrexate causes the ectopic pregnancy to shrink and disappear. After methotrexate is given, doctors do blood tests to measure hCG levels every few days or once a week to determine whether treatment was successful. If hCG cannot be detected, treatment is considered successful. If one dose of methotrexate was unsuccessful, a second dose of methotrexate or surgery is needed.Small ectopic pregnancies that have not ruptured may be treated with one dose of the medication methotrexate, given by injection. Methotrexate causes the ectopic pregnancy to shrink and disappear. After methotrexate is given, doctors do blood tests to measure hCG levels every few days or once a week to determine whether treatment was successful. If hCG cannot be detected, treatment is considered successful. If one dose of methotrexate was unsuccessful, a second dose of methotrexate or surgery is needed.
The ectopic pregnancy is removed surgically if doctors suspect the ectopic pregnancy has ruptured or if treatment with methotrexate cannot be given—for example, if the ectopic pregnancy is large or if a woman has abnormal blood test results for kidney or liver function.The ectopic pregnancy is removed surgically if doctors suspect the ectopic pregnancy has ruptured or if treatment with methotrexate cannot be given—for example, if the ectopic pregnancy is large or if a woman has abnormal blood test results for kidney or liver function.
If a woman is treated with surgery, doctors usually insert a viewing tube (laparoscope) into the abdominal cavity through a small incision just below the navel and use instruments threaded through the laparoscope to remove the ectopic pregnancy. In some cases, doctors have to make a larger incision in the abdomen (laparotomy).
During surgery for a tubal ectopic pregnancy, doctors remove the ectopic pregnancy by making an incision in the fallopian tube. Often, making an incision in the tube is all that is needed and the tube heals normally. Sometimes all or part of the tube may be removed, depending on how severely the tube is damaged and the woman's plans for future pregnancies. The entire fallopian tube may be removed if the woman requests tubal sterilization (both tubes would need surgery) or if the tube is abnormal and she is planning in vitro fertilization for a future pregnancy.
Women who have an Rh-negative blood type, whether they are given methotrexate or require surgery, are given Women who have an Rh-negative blood type, whether they are given methotrexate or require surgery, are givenRho(D) immune globulin to prevent Rh incompatibility (erythroblastosis fetalis), which occurs when a pregnant woman has Rh-negative blood and the fetus has Rh-positive blood.