



- Overview of Infertility
- Assisted Reproductive Technologies (ARTs)
- Infertility Problems With Ovulation
- Infertility Problems With Eggs
- Infertility Problems With the Fallopian Tubes and Abnormalities in the Pelvis
- Infertility Problems With Cervical Mucus
- Problems With Sperm
- Unexplained Infertility
- Recurrent Miscarriage
Assisted reproductive technologies (ARTs) involve working with sperm and eggs or embryos in a laboratory (in vitro) with the goal of producing a pregnancy.
Topic Resources

If infertility treatment with only medications has not or is not likely to result in pregnancy, ARTs, such as in vitro fertilization, may be considered. These techniques are more successful in women under age 35.
ARTs may result in multiple gestation (such as twins or triplets) but are less likely to do so than when treatment is with only fertility medications.
Sometimes during IVF, if the risk of genetic abnormalities is high, the embryo can often be tested before it is implanted in a woman’s uterus. This testing is called preimplantation genetic testing.
(See also Overview of Infertility.)
Did You Know...
|
Intrauterine insemination
Intrauterine insemination involves selecting the most active sperm, then placing them directly in the uterus through a tube inserted into the cervix. The most active sperm are selected by washing a semen sample. Doctors try to place these sperm in the uterus at the same time as ovulation.
Intrauterine insemination used alone is far less effective than in vitro fertilization but is often tried first because it is much less invasive and less expensive.
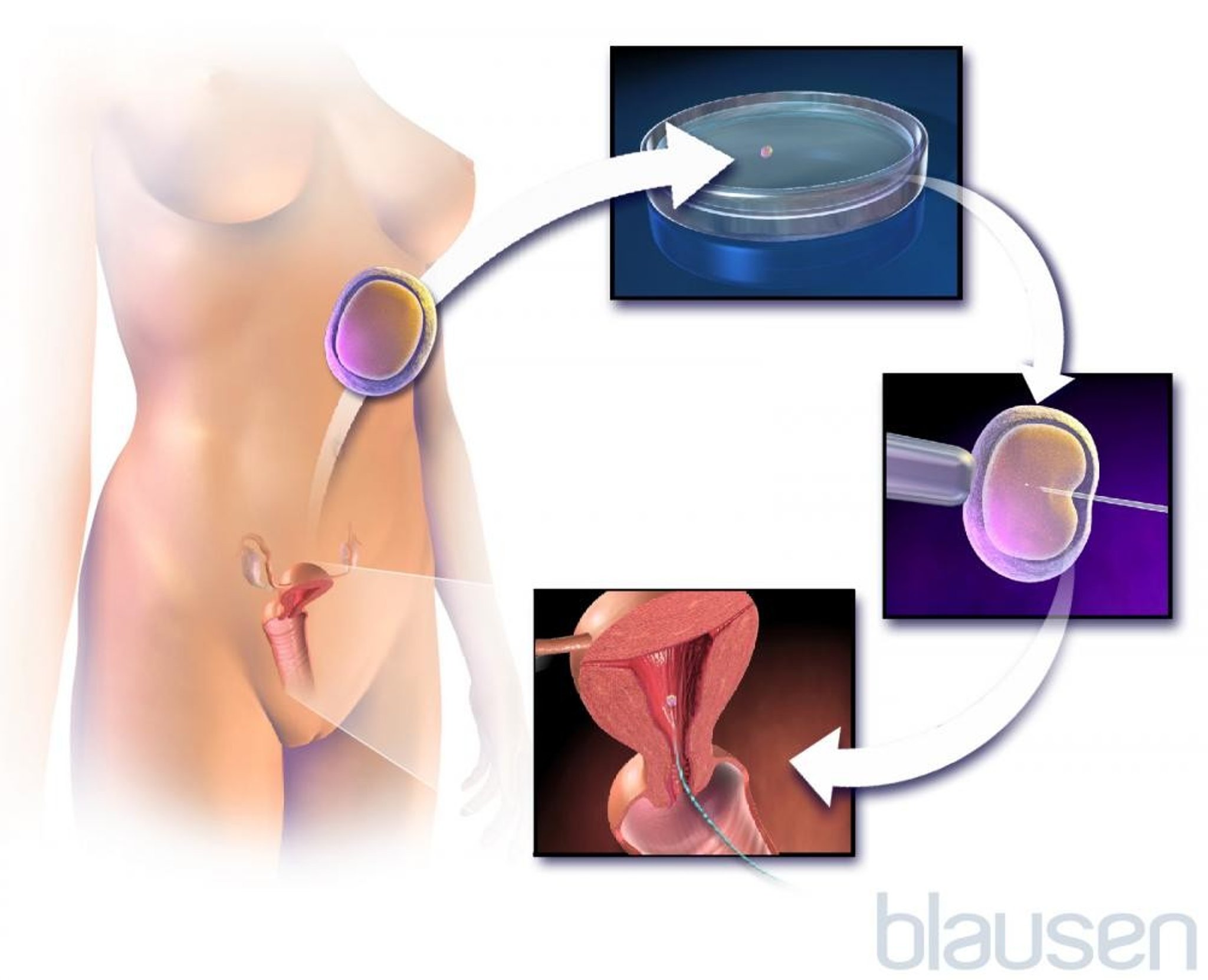
In vitro (test tube) fertilization (IVF)
In vitro fertilization (IVF) can be used to treat infertility regardless of the cause (including when it is unidentified).
IVF typically involves the following:
Stimulating the ovaries: Typically, several types of medication are given to stimulate a woman’s ovaries to produce more than 1 egg. Letrozole, Typically, several types of medication are given to stimulate a woman’s ovaries to produce more than 1 egg. Letrozole,clomiphene, and/or human gonadotropins are used to stimulate the development of follicles (sacs in the ovary that contain eggs). A gonadotropin-releasing hormone (GnRH) agonist or antagonist is often given to prevent ovulation from occurring until after several eggs have matured. As a result, many eggs usually mature. Then, human chorionic gonadotropin is given to stimulate ovulation. Alternatively, a GnRH agonist is used to stimulate ovulation in women with a high risk of developing ovarian hyperstimulation syndrome. In some cases, an egg that develops normally during a menstrual cycle (that is, without using fertility medications) is used during IVF.
Retrieving released eggs: About 34 hours later, a procedure is done to retrieve the eggs from the ovaries. A health care professional, guided by ultrasonography, inserts a needle through the vagina into the ovary and removes the eggs that have grown and developed. Sometimes the eggs are removed through a small tube (laparoscope) inserted through a small incision just below the navel.
Fertilizing the eggs: In a specialized fertility laboratory, the eggs are placed in a culture dish with sperm selected as the most active, so that fertilization can occur. Sometimes, a single sperm is injected into each oocyte (called intracytoplasmic sperm injection), particularly if sperm production is abnormal in the male partner.
Growing the resulting embryos: After sperm are added, the eggs are allowed to grow for about 2 to 5 days.
Implanting the embryos in the uterus: One or a few of the resulting embryos are transferred from the culture dish into the uterus by inserting a tube through the vagina and into the cervix. The number of embryos implanted is determined by the condition of the embryos, the likelihood that treatment will be successful, and the preferences of the prospective parents. Embryos are typically implanted 2 to 6 days after fertilization.
Because of improvements in infertility treatment and a preference for having only 1 baby, often only 1 embryo is used at each transfer. If there are additional embryos, they can be frozen to be used later if pregnancy does not occur or to be used for future pregnancies.
The chances of having a baby with in vitro fertilization depend on many factors, but a woman’s age may be most important. In the United States, the chances of having a successful pregnancy for each egg retrieved is estimated to be about 45% for women under age 35 and slightly over 9% for women aged 41 to 42. For women over 42 years old, using eggs from another woman (donor) is recommended, because the live birth rate with the their own eggs is so low (about 3%).
The greatest risk of in vitro fertilization is
Having a multiple gestation (such as twins or triplets)
A multiple gestation has increased risks to a woman and the fetuses (and eventually to the newborns). Complications may be related to the pregnancy. For example, a woman may develop high blood pressure or diabetes or have excessive bleeding. There is a higher risk of miscarriage, preterm delivery, and low birth weight. Because of these potential complications, doctors transfer only 1 or a small number of embryos to the uterus.
Birth defects are slightly more common among babies conceived through IVF. However, experts are unclear whether the reason is related to the technique or to the fertility problems that made IVF necessary. Also, millions of babies have been conceived through IVF, and the overwhelming majority of these babies have had no birth defects.
Additional options related to ARTs
Intracytoplasmic sperm injection
Intracytoplasmic sperm injection may be used when
A severe problem with sperm is present.
Other techniques are likely to be unsuccessful.
It is a common technique used to fertilize the egg by injecting only 1 sperm. If needed, it is done as part of the in vitro fertilization.
Birth defects may be more likely after this procedure, possibly because of the following:
The procedure can damage the egg, sperm, or embryo.
If sperm from men with an abnormal Y chromosome (one of the sex chromosomes) are used in this procedure, the development of reproductive organs in a male fetus may be affected, typically resulting in fertility problems like those of the father. Most birth defects in babies conceived by intracytoplasmic sperm injection involve the reproductive organs.

Egg or sperm donation
Sometimes the infertility evaluation shows that infertility treatments are not likely to be successful or treatments are not successful after several cycles. Depending on the reasons for this, prospective parents may choose to use donated eggs or sperm. Donated eggs or sperm may come from a donor the prospective parents know or from an anonymous donor.
For donor eggs, the donor goes through the first few steps of IVF. In the fertility laboratory, the eggs are placed in a culture dish with the sperm of the prospective male parent. The fertilized eggs are then transferred to uterus of the prospective female partner.
Donor sperm from anonymous donors is often frozen and stored in sperm banks. During fertility treatment, the donor sperm is placed in a culture dish with the eggs of the prospective female parent and then transferred to the uterus.
Gestational carrier
If a woman has an abnormality of the uterus or a medical condition that makes it not feasible to carry a pregnancy, then a gestational carrier is an option. A gestational carrier is a woman who carries the pregnancy in her uterus but is not the genetic parent (the egg does not come from the carrier). The fertilized eggs of the prospective parents are transferred to the uterus of the gestational carrier.
A surrogate is different from a gestational carrier. In a surrogate pregnancy, the egg comes from the woman who is the surrogate, so she is the genetic parent. This option is used less frequently because it can be more complicated emotionally and legally than using a gestational carrier.
Being a gestational carrier or a surrogate is illegal in many countries.







