


A doctor can often diagnose a musculoskeletal disorder based on the history and the results of a physical examination. Laboratory tests, imaging tests, or other diagnostic procedures are sometimes necessary to help the doctor make or confirm a diagnosis.
Laboratory Tests

Laboratory tests are often helpful in making the diagnosis of a musculoskeletal disorder. For example, blood tests are done to measure the level of C-reactive protein (CRP) in the blood and the erythrocyte sedimentation rate (ESR), the rate at which red blood cells settle to the bottom of a test tube containing blood. The ESR and the CRP are usually increased when inflammation is present. However, because inflammation occurs in so many conditions, both the ESR and the CRP levels alone do not establish a diagnosis.
The level of creatine kinase (a normal muscle enzyme that leaks out and is released into the bloodstream when muscle is damaged) may also be tested. Levels of creatine kinase are increased when there is widespread ongoing destruction of muscle.
In rheumatoid arthritis, a blood test to identify rheumatoid factor or anti-cyclic citrullinated peptide (anti-CCP) antibody is helpful in making the diagnosis.
In systemic lupus erythematosus (SLE or lupus), blood tests to identify autoimmune antibodies (autoantibodies), such as antinuclear antibodies and antibodies to double-stranded deoxyribonucleic acid (DNA), help in making the diagnosis.
A blood test can be done to identify people who have a certain gene (HLA-B27). People who have this gene are at increased risk of developing spondyloarthritis, a group of disorders that can cause inflammation of the back and other joints as well as other symptoms, such as eye pain and redness and rashes.
Some laboratory tests are also often useful to help monitor the progress of treatment. For example, the ESR can be particularly useful in helping to monitor the progress of treatment in rheumatoid arthritis or polymyalgia rheumatica. A decrease in the ESR suggests that treatment is working to reduce inflammation.
Imaging Tests
Various types of imaging tests can help doctors diagnose musculoskeletal disorders.
X-rays
X-rays are typically done first. They are most valuable for detecting abnormalities in bone and are taken to evaluate painful, deformed, or suspected abnormal areas of bone. Often, x-rays can help to diagnose fractures, tumors, injuries, infections, and deformities (such as developmental dysplasia of the hip). Also, sometimes x-rays are helpful in showing changes that confirm a person has a certain kind of arthritis (for example, rheumatoid arthritis or osteoarthritis). X-rays do not show soft tissues such as muscles, bursae, ligaments, tendons, or nerves.
To help determine whether the joint has been damaged by injury, a doctor may use an ordinary (non-stress) x-ray or one taken with the joint under stress caused by certain positions (stress x-ray).

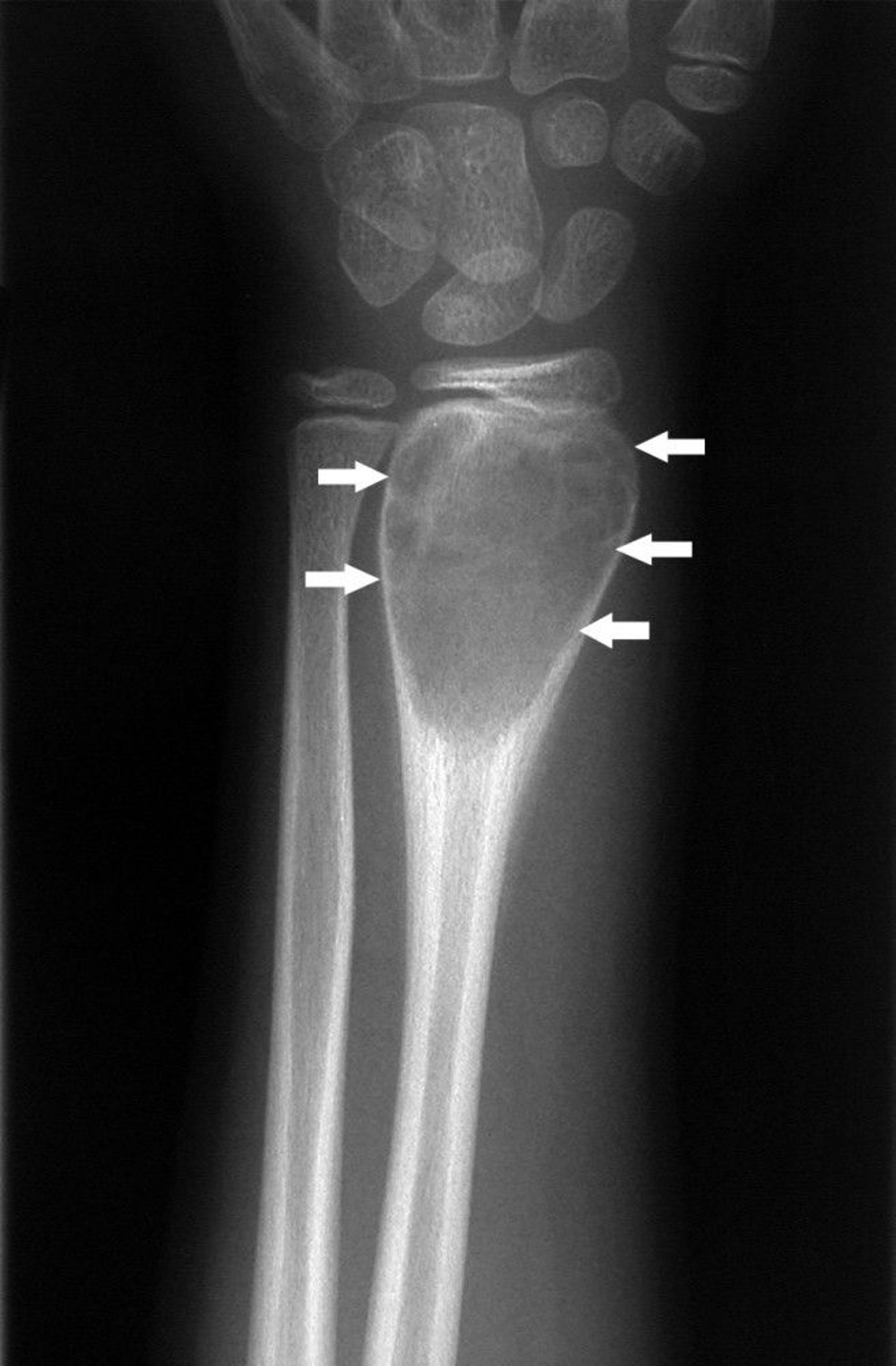
Image courtesy of Michael J. Joyce, MD, and Hakan Ilaslan, MD.
Arthrography is an x-ray procedure in which a radiopaque dye is injected into a joint space to outline the structures, such as ligaments inside the joint. Arthrography can be used to view torn ligaments and fragmented cartilage in the joint. However, magnetic resonance imaging (MRI) is now generally used in preference to arthrography.
Bone scanning
Bone scanning (a type of radionuclide scanning) is an imaging procedure that is occasionally used to diagnose a fracture, particularly if other tests, such as plain x-rays and computed tomography (CT) or magnetic resonance imaging (MRI), do not reveal the fracture. Bone scanning involves use of a radioactive substance (technetium-99m–labeled pyrophosphate) that is absorbed by any healing bone. The procedure can also be done when a bone infection or a tumor that has spread from a cancer elsewhere in the body is suspected.
Although a bone scan may show a problem in the bone, it may not show whether the problem is a fracture, tumor, or infection. The radioactive substance is given by vein (intravenously) and is detected by a bone-scanning device, which creates an image of the bone that can be viewed on a computer screen.
Computed tomography (CT) and magnetic resonance imaging (MRI)
Computed tomography (CT) and magnetic resonance imaging (MRI) give much more detail than plain x-rays and may be done to determine the extent and exact location of damage. These tests can also be used to detect fractures that are not visible on x-rays.



Image provided by Jon A Jacobson, MD.
MRI is especially valuable for imaging muscles, ligaments, and tendons. MRI can be used if the cause of pain is thought to be a severe soft-tissue problem (for example, rupture of a major ligament or tendon or damage to important structures inside the knee joint).
CT is useful if MRI is unavailable or not recommended. CT exposes people to ionizing radiation (see Risks of Radiation in Medical Imaging). CT best images bone compared with other structures. However, MRI is better than CT for imaging some bone abnormalities, such as small fractures of the hip and pelvis. The amount of time a person spends undergoing CT is much less than for MRI. MRI is more expensive than CT and, with the exception of when the open-sided units are used, many people feel claustrophobic inside the MRI unit.
Dual-energy x-ray absorptiometry (DXA)
The most accurate way to evaluate bone density is with dual-energy x-ray absorptiometry (DXA). DXA is necessary when screening for or diagnosing osteopenia (reduced bone density) or its progression to osteoporosis. DXA is also used to predict a person's risk of fracture and can be useful for monitoring the response to treatment as well. This test is quick and painless and involves very little radiation.
In this test, x-rays are used to examine bone density at the lower spine, hip, wrist, or entire body. Measurements of bone density are very accurate at these sites. When screening people for osteoporosis, doctors prefer taking measurements of the lower spine and hip. To help differentiate osteoporosis (the most common cause of an abnormal DXA scan result) from other bone disorders, doctors may need to consider the person's symptoms, medical conditions, medications, and certain blood or urine test results as well as the DXA results.
Ultrasonography
Ultrasonography is being used more and more frequently to identify abnormalities and inflammation in and around joints and tears or inflammation of tendons. Ultrasonography is also used as a guide when a needle needs to be put into a joint (for example, to inject medications or to remove joint fluid). As an alternative to computed tomography (CT) and magnetic resonance imaging (MRI), ultrasonography is less expensive and, unlike CT, involves no exposure to radiation.
Other Diagnostic Procedures
Other procedures and tests are sometimes needed to help doctors diagnose musculoskeletal disorders.
Arthroscopy
Arthroscopy is a procedure in which a small (diameter of a pencil) fiberoptic scope is inserted into a joint space, allowing the doctor to look inside the joint and to project the image onto a video monitor. The skin incision is very small. This procedure is done in a hospital or surgical center. The person is given local, spinal, or general anesthesia or a combination.
During arthroscopy, doctors can take a piece of tissue (such as joint cartilage or the joint capsule) for analysis (biopsy), and, if necessary, do surgery to correct the condition. Disorders commonly found during arthroscopy include
Inflammation of the synovium lining the joint (synovitis)
Ligament, tendon, or cartilage tears
Loose pieces of bone or cartilage
Such conditions affect people with arthritis or previous joint injuries as well as athletes. Most of these conditions can be repaired or removed during arthroscopy. There is a very small risk of joint infection with this procedure.
Recovery time after arthroscopic surgery is much faster than after traditional surgery. Most people do not need to stay overnight in the hospital.
Joint aspiration (arthrocentesis)
Joint aspiration is used to diagnose certain joint problems. For example, it is the most direct and accurate way to determine whether joint pain and swelling is caused by an infection or crystal-related arthritis (such as gout).
For this procedure, a doctor first injects an anesthetic to numb the area. Then the doctor inserts a larger needle into the joint space (sometimes guided by ultrasonography), draws out (aspirates) joint fluid (synovial fluid), and examines the fluid under a microscope. A doctor removes as much fluid as possible and notes its color and clarity. Other tests, such as white blood cell count and culture, are done on the fluid.
The doctor can often make a diagnosis after analyzing the fluid. For example, a sample of fluid may contain bacteria, which confirm a diagnosis of infection. Or, it may contain certain crystals. For example, finding uric acid crystals confirms a diagnosis of gout, and calcium pyrophosphate dihydrate crystals confirm a diagnosis of calcium pyrophosphate arthritis (pseudogout).
Usually done in the doctor's office or an emergency department, this procedure is typically quick, easy, and relatively painless. The risk of joint infection is minimal.
Nerve and muscle tests
Nerve conduction studies help determine whether the nerves supplying the muscles are functioning normally. Electromyography, usually done at the same time as nerve conduction studies, is a test in which electrical impulses in the muscles are recorded to help determine how well the impulses from the nerves are reaching the connection between nerves and muscles (neuromuscular junction) and, from there, the muscles.
Nerve conduction studies, together with electromyography, help indicate whether there is a problem primarily in the
Muscles (such as myositis or muscular dystrophy)
Nervous system (the brain, spinal cord, and nerves), which controls the muscles (such as a stroke, spinal cord problem, or polyneuropathy)
Neuromuscular junction (such as myasthenia gravis)
Nerve conduction studies are particularly useful for the diagnosis of peripheral nerve disorders, such as carpal tunnel syndrome and ulnar nerve palsy.







