


Rheumatoid arthritis is an inflammatory arthritis in which joints, usually including those of the hands and feet, are inflamed, resulting in swelling, pain, and often destruction of joints.
The immune system damages the joints and connective tissues.
Joints (typically the small joints of the limbs) become painful and have stiffness that persists for more than 60 minutes on awakening and after inactivity.
Fever, weakness, and damage to other organs may occur.
Diagnosis is based mainly on symptoms but also on blood tests for rheumatoid factor and anti-cyclic citrullinated peptide (anti-CCP) and on x-rays.
Treatment can include exercises and splinting, medications (nonsteroidal anti-inflammatory drugs, disease-modifying antirheumatic drugs, and immunosuppressive drugs), and sometimes surgery.
Worldwide, rheumatoid arthritis develops in about 0.5% of the population, regardless of race or country of origin, affecting women 2 to 3 times more often than men. Usually, rheumatoid arthritis first appears between 35 years and 50 years of age, but it may occur at any age. A disorder similar to rheumatoid arthritis can occur in children. The disease is then called juvenile idiopathic arthritis. However, the prognosis for juvenile idiopathic arthritis is often somewhat different.
The exact cause of rheumatoid arthritis is not known. It is considered an autoimmune disease. Components of the immune system attack the soft tissue that lines the joints (synovial tissue) and can also attack connective tissue in many other parts of the body, such as the blood vessels and lungs. Eventually, the cartilage, bone, and ligaments of the joint erode (wear away), causing deformity, instability, and scarring within the joint. The joints deteriorate at a variable rate. Many factors, including genetic predisposition, may influence the pattern of the disease. Unknown environmental factors (such as viral infections and cigarette smoking) are thought to play a role.
Risk factors for rheumatoid arthritis include the following:
Smoking
Obesity
Changes in the microbiome (the group of microorganisms that normally live in a particular part of the body, such as the digestive tract, mouth, and lungs)
Periodontal disease (periodontitis)
Did You Know...
|
Symptoms of Rheumatoid Arthritis
People with rheumatoid arthritis may have
Relatively mild symptoms
Occasional flare-ups with long periods of remission (in which the disease is inactive)
A severe, steadily progressive disease, which may be slow or rapid
Rheumatoid arthritis may start suddenly, with many joints becoming inflamed at the same time. More often, it starts subtly, gradually affecting different joints. Usually, the inflammation is symmetric, with joints on both sides of the body affected about equally. Rheumatoid arthritis can affect any joint, but most often the first inflamed are the small joints in the
Hands
Wrists
Fingers
Feet
Toes
Other commonly affected joints include the
Knees
Shoulders
Elbows
Ankles
Hips
Rheumatoid arthritis can also affect the neck. The lower spine and the joints at the tips of the fingers are not affected.
The inflamed joints are usually painful and often stiff, especially just after awakening (such stiffness generally lasts for more than 60 minutes) or after prolonged inactivity. Some people feel tired and weak, especially in the early afternoon. Rheumatoid arthritis may cause a loss of appetite with weight loss and a low-grade fever.
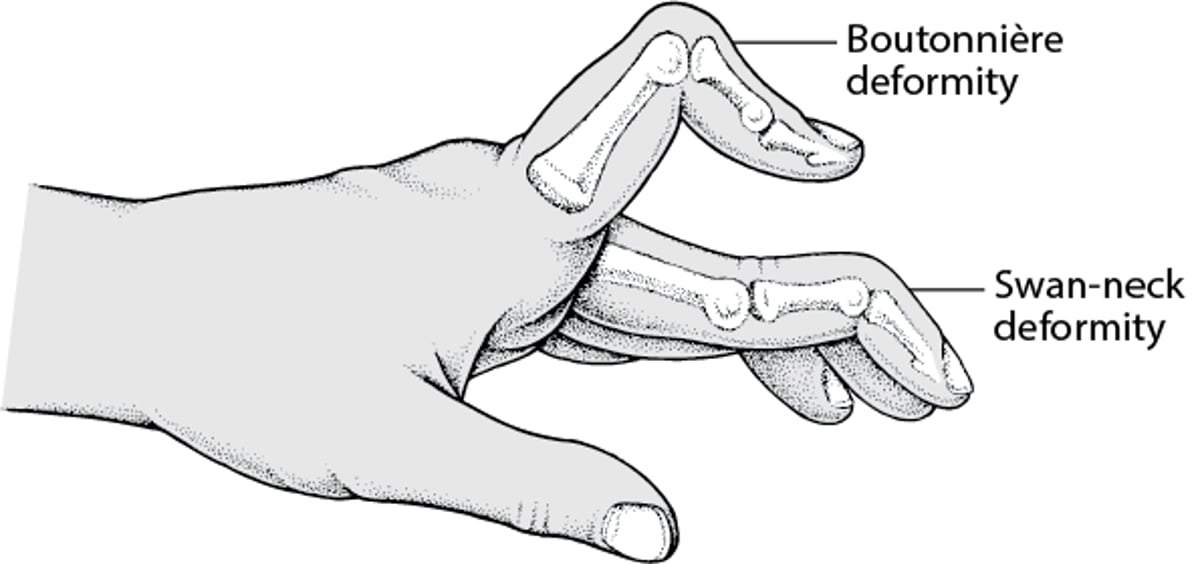
Affected joints are often tender, warm, and enlarged because of swelling of the soft tissue lining the joint (synovitis) and sometimes fluid within the joint (synovial fluid). Joints can quickly become deformed. Joints may freeze in one position so that they cannot bend or open fully, which leads to a limited range of motion. The fingers may tend to dislocate slightly from their normal position toward the little finger on each hand, causing tendons in the fingers to slip out of place, or may develop other deformities (see swan-neck deformity and boutonnière deformity).
When the Fingers Are Abnormally Bent
Some disorders, such as rheumatoid arthritis, and injuries can cause the fingers to bend abnormally. In swan-neck deformity, the joint at the base of the finger bends in (flexes), the middle joint straightens out (extends), and the outermost joint bends in (flexes). In boutonnière deformity, the middle finger joint is bent inward (toward the palm), and the outermost finger joint is bent outward (away from the palm). |

Swollen wrists can pinch a nerve and result in numbness or tingling due to carpal tunnel syndrome.
Cysts, which may develop behind affected knees, can rupture, causing pain and swelling in the lower legs. Up to 30% of people with rheumatoid arthritis have hard bumps just under the skin (called rheumatoid nodules), usually near sites of pressure (such as the back of the forearm near the elbow).
Rarely, rheumatoid arthritis causes an inflammation of blood vessels (vasculitis). Vasculitis reduces the blood supply to tissues and may cause nerve damage or leg sores (ulcers). Inflammation of the membranes that cover the lungs (pleura) or of the sac surrounding the heart (pericardium) or inflammation and scarring of the lungs or heart can lead to chest pain or shortness of breath. Some people develop swollen lymph nodes (lymphadenopathy), Felty syndrome (a low white blood cell count and an enlarged spleen), Sjögren syndrome (dry mouth and eyes), thinning of the white of the eye (sclera), or red, irritated eyes caused by inflammation (episcleritis).
Rheumatoid arthritis can also affect the neck, making the bones unstable and increasing the risk of the bones putting pressure on (compressing) the spinal cord . Neck involvement is common in longstanding, active rheumatoid arthritis and usually causes headaches and pain and stiffness, sometimes with pain that radiates down the arms or legs.
People with rheumatoid arthritis are at increased risk for early coronary artery disease and bone disease, such as osteopenia and osteoporosis.


In swan-neck deformity, the finger takes on a curved shape, like the neck of a swan.
SCIENCE PHOTO LIBRARY


This photo shows a boutonnière (buttonhole) deformity of the ring finger.
© Springer Science+Business Media


This photo shows multiple boutonnière deformities of the fingers and thumbs in this person with advanced rheumatoid arthritis.
By permission of the publisher. From Matteson E, Mason T: Atlas of Rheumatology. Edited by G Hunder. Philadelphia, Current Medicine, 2005.

This photo shows bumps (rheumatoid nodules) on the sole of the foot in a person who has rheumatoid arthritis.
DR P. MARAZZI/SCIENCE PHOTO LIBRARY


This photo shows a hard bump under the skin (rheumatoid nodule) over the joint in the hand of a person who has rheumatoid arthritis.
DR P. MARAZZI/SCIENCE PHOTO LIBRARY
In swan-neck deformity, the finger takes on a curved shape, like the neck of a swan.
SCIENCE PHOTO LIBRARY
This photo shows a boutonnière (buttonhole) deformity of the ring finger.
© Springer Science+Business Media
This photo shows multiple boutonnière deformities of the fingers and thumbs in this person with advanced rheumatoid arthritis.
By permission of the publisher. From Matteson E, Mason T: Atlas of Rheumatology. Edited by G Hunder. Philadelphia, Current Medicine, 2005.
This photo shows bumps (rheumatoid nodules) on the sole of the foot in a person who has rheumatoid arthritis.
DR P. MARAZZI/SCIENCE PHOTO LIBRARY
This photo shows a hard bump under the skin (rheumatoid nodule) over the joint in the hand of a person who has rheumatoid arthritis.
DR P. MARAZZI/SCIENCE PHOTO LIBRARY
Diagnosis of Rheumatoid Arthritis
Blood tests
Imaging tests (x-rays, ultrasound, or magnetic resonance imaging [MRI])
Examination of joint fluid
In addition to the important characteristic pattern of symptoms, doctors follow established criteria when evaluating a person for rheumatoid arthritis. Doctors suspect rheumatoid arthritis in people who have more than one joint with definite swelling of the joint's lining that is not caused by another disorder. Doctors diagnose rheumatoid arthritis if people have certain combinations of the following criteria:
Involvement of the joints that are most typical of rheumatoid arthritis
High blood levels of rheumatoid factor, anti-cyclic citrullinated peptide (anti-CCP) antibodies, or both
High blood levels of C-reactive protein, a high erythrocyte sedimentation rate (ESR), or both
Symptoms that have lasted at least 6 weeks
Doctors check blood tests to determine a person's levels of rheumatoid factor and anti-CCP antibodies and usually C-reactive protein, ESR, or both. They also frequently do x-rays of the hands, wrists, and affected joints. X-rays sometimes show characteristic changes in the joints caused by rheumatoid arthritis. Ultrasound and magnetic resonance imaging (MRI) are other imaging tests that can detect joint abnormalities at an earlier stage but are not always needed.
Doctors may also insert a needle into a joint to draw a sample of synovial fluid, the thick fluid that lubricates joints and reduces friction. The fluid is examined to determine whether it is consistent with features of rheumatoid arthritis and to rule out other disorders that cause symptoms similar to rheumatoid arthritis. Synovial fluid needs to be analyzed to establish that a person has rheumatoid arthritis but does not always need to be analyzed whenever a flare-up causes joints to become swollen.
Blood tests
Many people with rheumatoid arthritis have distinctive antibodies in their blood, such as rheumatoid factor and anti-CCP antibodies. However, doctors do not rely only on blood tests to diagnose rheumatoid arthritis.
Rheumatoid factor is present in 70% of people with rheumatoid arthritis. (Rheumatoid factor also occurs in several other diseases, such as cancers, systemic lupus erythematosus, hepatitis, and some other infections. Some people without any disorder, particularly older adults, have rheumatoid factor in their blood.)
Anti-CCP antibodies are present in over 75% of people who have rheumatoid arthritis and are almost always absent in people who do not have rheumatoid arthritis. The presence of anti-CCP and rheumatoid factor, especially in people who smoke cigarettes, predicts that their arthritis will be more severe.
C-reactive protein levels are often high in people with rheumatoid arthritis. Levels of C-reactive protein (a protein that circulates in the blood) dramatically increase when there is inflammation. High C-reactive protein levels can mean the disease is active.

The ESR is increased in 90% of people who have active rheumatoid arthritis. The ESR is another test for inflammation and measures the rate at which red blood cells settle to the bottom of a test tube containing blood. However, similar increases in the ESR, C-reactive protein level, or both occur in many other disorders. Doctors may monitor the ESR or C-reactive protein to help determine whether the disease is active.
Most people with rheumatoid arthritis have mild anemia (an insufficient number of red blood cells). Rarely, the white blood cell count becomes abnormally low. When a person with rheumatoid arthritis has a low white blood cell count and an enlarged spleen, the disorder is called Felty syndrome.
Treatment of Rheumatoid Arthritis
Medications
Lifestyle measures, such as rest, diet, exercise, and stopping smoking
Physical therapy and occupational therapy
Sometimes surgery
Treatments include simple, conservative measures in addition to medications and surgical treatments. Simple measures are meant to help the person’s symptoms and include rest, adequate nutrition, and physical treatments. People should take measures that decrease their risk of heart disease, such as stopping smoking and getting treated, if necessary, for high blood pressure and high blood lipids or cholesterol.
Medications
Because disease-modifying antirheumatic drugs (DMARDs) may actually slow progression of the disease as well as relieve symptoms, they are often started soon after the diagnosis of rheumatoid arthritis is made. For a complete discussion of DMARDs and other medications used to treat rheumatoid arthritis, see Medications for Rheumatoid Arthritis.
Lifestyle measures
Lifestyle measures play an important role in disease management. These measures include exercising regularly, maintaining a healthy diet, achieving and maintaining a healthy weight, keeping alcohol consumption moderate, stopping smoking, and modifying the worksite if needed for active work participation. Quality sleep is also important, because poor sleep increases pain.
Severely inflamed joints should be rested because using them can aggravate the inflammation. Regular rest periods often help relieve pain, and sometimes a short period of bed rest helps relieve a severe flare-up in its most active, painful stage.
A healthy diet, such as the Mediterranean diet (which is high in fruits and vegetables and low in processed foods), is generally appropriate. A diet rich in fish (omega-3 fatty acids) and plant oils but low in red meat can partially relieve symptoms in some people. Some people may have flare-ups after eating certain foods, and if so, these foods should be avoided, but such flare-ups occur rarely. No specific foods have been proved to cause flare-ups. Many diets have been proposed but have not proved helpful. Fad diets should be avoided.
Physical treatments
Along with medications to reduce joint inflammation, a treatment plan for rheumatoid arthritis should include nondrug therapies, such as exercise, physical therapy (which includes massage, traction, and deep heat treatments), and occupational therapy (which includes self-help or assistive devices).
Splints can be used to immobilize and rest one or several joints, but some systematic movement of the joints is needed to prevent nearby muscles from weakening and joints from freezing in place.
Inflamed joints should be gently stretched so they do not freeze in one position. Heat therapy can be helpful because heat improves muscle function by reducing stiffness and muscle spasm. As the inflammation subsides, regular, active exercises can help, although a person should not exercise to the point of excessive fatigue. For many people, exercise in warm water may be easier.
Treatment of tight joints consists of intensive exercises and occasionally the use of splints to gradually extend the joint. Cold may be applied to reduce pain caused by temporary worsening in one joint.
People who are disabled by rheumatoid arthritis can use several aids to accomplish daily tasks. For example, specially modified orthopedic or athletic shoes can make walking less painful, and assistive devices such as grippers reduce the need to squeeze the hand forcefully.
Surgery
If medications have not helped, surgical treatment may be needed. Surgical repair must always be considered in terms of the total disease. For example, deformed hands and arms limit a person’s ability to use crutches during rehabilitation, and seriously affected knees and feet limit the benefits of hip surgery. Reasonable objectives for each person must be determined, and ability to function must be considered. Surgical repair may be performed while the disease is active.
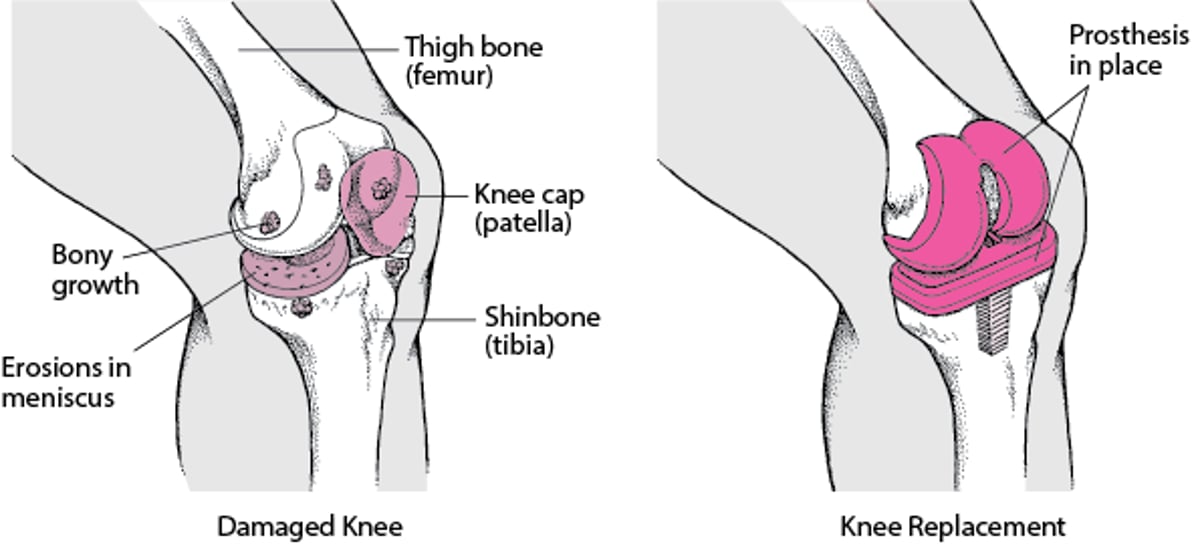
Surgically replacing knee or hip joints is the most effective way to restore mobility and function when the joint disease is advanced. Joints can also be removed or fused together, especially in the foot, to make walking less painful. The thumb can be fused to enable a person to pinch, and unstable vertebrae at the top of the neck can be fused to prevent them from compressing the spinal cord.
Joint repair with prosthetic joint replacement is indicated if damage severely limits function. Total hip replacements and knee replacements are generally successful.
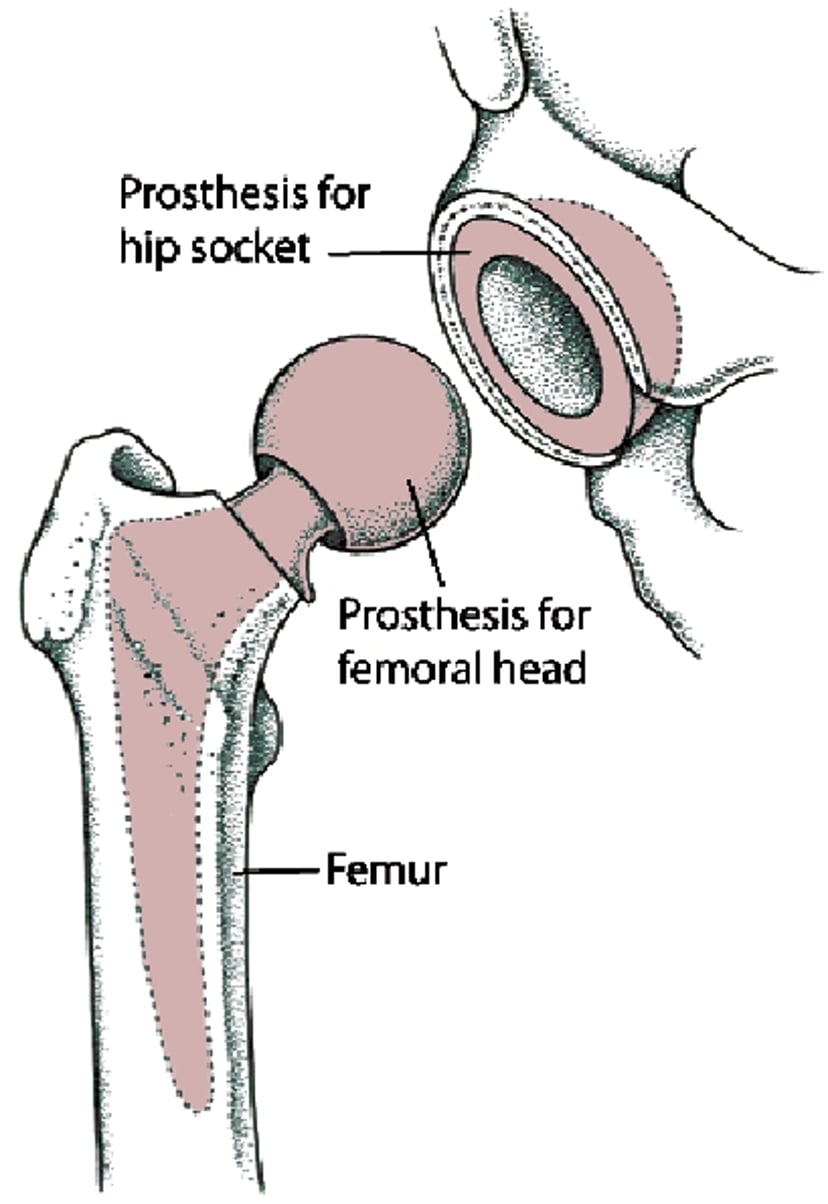
Replacing All of a Hip (Total Hip Replacement)
Sometimes the whole hip joint must be replaced. The whole hip joint is the top (head) of the thighbone (femur) and the surface of the socket into which the head of the thighbone fits. This procedure is called total hip replacement or total hip arthroplasty. The head of the thighbone is replaced with a ball-shaped part (prosthesis), made of metal. The prosthesis has a strong stem that fits within the center of the thighbone. The socket is replaced with a metal shell lined with durable plastic. |

Replacing a Knee
A knee joint damaged by osteoarthritis may be replaced with an artificial joint. After a general anesthetic is given, the surgeon makes an incision over the damaged knee. The knee cap (patella) may be removed, and the ends of the thigh bone (femur) and shinbone (tibia) are smoothed so that the parts of the artificial joint (prosthesis) can be attached more easily. One part of the artificial joint is inserted into the thigh bone, the other part is inserted into the shinbone, and then the parts are cemented in place. |

Medications for Rheumatoid Arthritis
The main goal of treatment with medications is to reduce inflammation and thereby prevent erosions, progression of the disease, and loss of joint function.
The main categories of medications used to treat rheumatoid arthritis are
Disease-modifying antirheumatic drugs (DMARDs), which include biologic agents
Many of these medications are used in combination. For example, doctors may prescribe two DMARDs together or a corticosteroid plus a DMARD. However, the best combinations of medications are not yet clear. Typically, biologic agents are not used in combination with other biologic agents because these combinations increase the frequency of infections.
All the categories of drugs have potentially serious side effects that must be looked for during treatment.
Disease-modifying antirheumatic drugs (DMARDs)
DMARDs can be broadly characterized into 3 types:
Conventional synthetic DMARDs, for example, methotrexate, sulfasalazine, and leflunomideConventional synthetic DMARDs, for example, methotrexate, sulfasalazine, and leflunomide
Biologic DMARDs, such as tumor necrosis factor [TNF] inhibitors, interleukin [IL]-6, and abataceptBiologic DMARDs, such as tumor necrosis factor [TNF] inhibitors, interleukin [IL]-6, and abatacept
Targeted synthetic DMARDs, such as tofacitinib and upadacitinibTargeted synthetic DMARDs, such as tofacitinib and upadacitinib
DMARDs, such as methotrexate, hydroxychloroquine, leflunomide, and sulfasalazine, slow the progression of rheumatoid arthritis and are given to nearly all people with rheumatoid arthritis. Doctors typically prescribe these medications as soon as the diagnosis of rheumatoid arthritis is made. Many take weeks to have an effect. Even if pain is decreased with NSAIDs, a doctor will likely prescribe a DMARD because the disease may otherwise progress even if symptoms are lessened. (See also table DMARDs, such as methotrexate, hydroxychloroquine, leflunomide, and sulfasalazine, slow the progression of rheumatoid arthritis and are given to nearly all people with rheumatoid arthritis. Doctors typically prescribe these medications as soon as the diagnosis of rheumatoid arthritis is made. Many take weeks to have an effect. Even if pain is decreased with NSAIDs, a doctor will likely prescribe a DMARD because the disease may otherwise progress even if symptoms are lessened. (See also tableMedications Used to Treat Rheumatoid Arthritis .)
Combinations of DMARDs may be more effective than single medications. For example, hydroxychloroquine, sulfasalazine, and methotrexate together are more effective than Combinations of DMARDs may be more effective than single medications. For example, hydroxychloroquine, sulfasalazine, and methotrexate together are more effective thanmethotrexate alone or the other two together. Also, combining biologic agents with a DMARD is often more effective than using a single medication or certain combinations of DMARDs. For example, methotrexate can be combined with a TNF inhibitor.
Conventional synthetic DMARDs
Conventional synthetic (nonbiologic) DMARDs slow the progression of rheumatoid arthritis and are given to nearly all people with rheumatoid arthritis. They differ from each other chemically and pharmacologically. There are risks with these medications, and people should be monitored closely for evidence of toxicity.
MethotrexateMethotrexate is taken by mouth once weekly. It is anti-inflammatory at the low doses used to treat rheumatoid arthritis. Methotrexate is very effective and begins to work within 3 to 4 weeks, which is relatively rapid for a DMARD. The liver can scar, but this scarring most often can be detected by monitoring with regular blood tests and reversed before major damage develops. People taking is taken by mouth once weekly. It is anti-inflammatory at the low doses used to treat rheumatoid arthritis. Methotrexate is very effective and begins to work within 3 to 4 weeks, which is relatively rapid for a DMARD. The liver can scar, but this scarring most often can be detected by monitoring with regular blood tests and reversed before major damage develops. People takingmethotrexate must refrain from drinking alcohol to minimize the risk of liver damage. Bone marrow suppression (suppression of the production of red blood cells, white blood cells, and platelets) may occur. Blood counts should be tested about every 2 to 3 months in all people taking the medication. Inflammation of the lung (pneumonitis) is rare. Inflammation in the mouth and nausea can also develop. Severe relapses of arthritis can occur after methotrexate is discontinued. Folate (folic acid) tablets may decrease some of the side effects, such as mouth ulcers. Rheumatoid nodules may enlarge with is discontinued. Folate (folic acid) tablets may decrease some of the side effects, such as mouth ulcers. Rheumatoid nodules may enlarge withmethotrexate therapy.
HydroxychloroquineHydroxychloroquine is given daily by mouth. Side effects, which are usually mild, include rashes, muscle aches, and eye problems. However, some eye problems can be permanent, so people taking hydroxychloroquine must have their eyes checked by an ophthalmologist before treatment begins and every 12 months during treatment. If the medication has not helped after 9 months, it is discontinued. Otherwise, hydroxychloroquine can be continued as long as necessary.
SulfasalazineSulfasalazine is initially given by mouth and can relieve symptoms and slow the development of joint damage. Sulfasalazine can also be used in people who have less severe rheumatoid arthritis or added to other medications to boost their effectiveness. The dose is increased gradually, and improvement usually is seen within 3 months. Because sulfasalazine may quickly cause a person's white blood cell count to become very low (neutropenia), blood tests are done after the first 2 weeks and then about every 12 weeks while the person is taking the medication. Like the other DMARDs, it can cause stomach upset, diarrhea, liver problems, blood cell disorders, and rashes. In males, sulfasalazine may cause a low sperm count, which is reversible.
LeflunomideLeflunomide is taken daily by mouth and has benefits that are similar to those of methotrexate but it is less likely to cause suppression of blood cell production in the bone marrow, abnormal liver tests, or inflammation of the lungs (pneumonitis). It can be given at the same time as methotrexate. The major side effects are rashes, liver dysfunction, hair loss, diarrhea, and rarely nerve damage (neuropathy).
Biologic DMARDs
A biologic agent is something made from a living organism, often using cells in a laboratory. Many biologic agents used to treat rheumatoid arthritis are antibodies. Biologic agents used to treat rheumatoid arthritis include abatacept, rituximab, tumor necrosis factor (TNF) inhibitors (adalimumab, certolizumab pegol, etanercept, golimumab, and infliximab), an interleukin-1 receptor blocker (anakinra), and interleukin-6 receptor blockers (tocilizumab and sarilumab). (See also table A biologic agent is something made from a living organism, often using cells in a laboratory. Many biologic agents used to treat rheumatoid arthritis are antibodies. Biologic agents used to treat rheumatoid arthritis include abatacept, rituximab, tumor necrosis factor (TNF) inhibitors (adalimumab, certolizumab pegol, etanercept, golimumab, and infliximab), an interleukin-1 receptor blocker (anakinra), and interleukin-6 receptor blockers (tocilizumab and sarilumab). (See also tableMedications Used to Treat Rheumatoid Arthritis.)
Biologic agents may suppress the inflammation so that corticosteroids can be avoided or given in lower doses. But by interfering with the immune system, biologic agents may increase the risks of infection and certain cancers. Because treatment with biologic agents increases the risk of infection, before starting treatment with a biologic agent people should be up to date on vaccinations (see table Protecting Adults Through Vaccines).
TNF is an important part of the body’s immune system, so inhibition of TNF can impair the body’s ability to fight infections, particularly a reactivated tuberculosis infection. These medications should be avoided in people who have active infections and should be discontinued before major surgery. Etanercept, infliximab, and adalimumab can be and are often used with methotrexate. People who have severe TNF is an important part of the body’s immune system, so inhibition of TNF can impair the body’s ability to fight infections, particularly a reactivated tuberculosis infection. These medications should be avoided in people who have active infections and should be discontinued before major surgery. Etanercept, infliximab, and adalimumab can be and are often used with methotrexate. People who have severeheart failure should not take high doses of infliximab.should not take high doses of infliximab.
Side effects of TNF inhibitors include the potential risk of reactivation of infection (particularly tuberculosis and fungal infections), skin cancers other than melanoma, and reactivation of hepatitis B.
TocilizumabTocilizumab, an IL-6 receptor blocker, is given to people who have not been helped by or who cannot tolerate conventional synthetic DMARDs. It can be used alone or sometimes in combination with methotrexate. Side effects include infection (such as , an IL-6 receptor blocker, is given to people who have not been helped by or who cannot tolerate conventional synthetic DMARDs. It can be used alone or sometimes in combination with methotrexate. Side effects include infection (such astuberculosis), suppression of blood cell production in the bone marrow (neutropenia), anaphylaxis (a life-threatening allergic reaction), and increased liver enzymes. There may be an increased risk of bowel perforation when people who have had diverticulitis use tocilizumab.
SarilumabSarilumab is an IL-6 receptor blocker, which means it interrupts one of the major chemical pathways involved in inflammation. This medication is given to people who have not been helped by or who cannot tolerate conventional synthetic DMARDs. Sarilumab can cause suppression of blood cell production in the bone marrow (neutropenia), suppression of platelet production in the bone marrow (sometimes with increased susceptibility to bleeding), and increased liver enzymes. Like tocilizumab, there may also be an increased risk of bowel perforation in people who have had diverticulitis.can cause suppression of blood cell production in the bone marrow (neutropenia), suppression of platelet production in the bone marrow (sometimes with increased susceptibility to bleeding), and increased liver enzymes. Like tocilizumab, there may also be an increased risk of bowel perforation in people who have had diverticulitis.
AbataceptAbatacept is another biologic agent that interferes with the communication between cells that coordinates inflammation. This medication is given to people who have not been helped by or who cannot tolerate conventional synthetic DMARDs. Side effects include lung problems, headache, increased susceptibility to infection, and upper respiratory infection.
RituximabRituximab is a biologic agent that decreases the number of B-cell lymphocytes, one of the white blood cells responsible for causing inflammation and for fighting infection. Rituximab is usually reserved for people who do not improve enough after taking methotrexate and a TNF inhibitor. Side effects, as with other immunosuppressive drugs, may include increased risk of infections. In addition, is usually reserved for people who do not improve enough after taking methotrexate and a TNF inhibitor. Side effects, as with other immunosuppressive drugs, may include increased risk of infections. In addition,rituximab can cause effects while it is being given, such as rashes, nausea, back pain, itching, and high or low blood pressure. It can cause severe liver damage by reactivating hepatitis B in people who had previously been infected with this virus.
The COVID-19 vaccine may be less effective in people taking rituximab, and people on rituximab may have poorer outcomes if infected with COVID-19. Therefore, doctors now try to reserve rituximab for people who did not respond to other biologic DMARDs and to those with certain lymphatic disorders and cancers.
AnakinraAnakinra is an interleukin-1 (IL-1) receptor blocker, which means it interrupts one of the major chemical pathways involved in inflammation. Side effects include infection and neutropenia. It is rarely used because it is not as effective as other biologics and because it is a daily injection.
Targeted synthetic DMARDs
Janus kinase inhibitors are small molecule agents that interfere with the communication between cells that coordinate inflammation by inhibiting the enzyme JAK. JAK inhibitors include the following (see also table Medications Used to Treat Rheumatoid Arthritis):
TofacitinibTofacitinib is used if a person has taken methotrexate and has not improved enough. is used if a person has taken methotrexate and has not improved enough.Tofacitinib can be used at the same time as methotrexate.
UpadacitinibUpadacitinib is given to adults with moderately to severely active rheumatoid arthritis when methotrexate has not been effective enough. is given to adults with moderately to severely active rheumatoid arthritis when methotrexate has not been effective enough.
BaricitinibBaricitinib is given to people who have not been helped by or who cannot tolerate TNF inhibitors.
Because treatment with JAK inhibitors increases the risk of infection, including herpes zoster infection, people should be vaccinated against zoster before starting treatment with a JAK inhibitor. Doctors should also discuss the potentially increased risk of major cardiovascular events associated with this class of drugs. Major cardiovascular events include heart attack, stroke, deep vein thrombosis, and pulmonary embolism. Some patients are at higher risk for these side effects, and the risks and benefits should be weighed before using these medications. These medications also increase the risk of nonmelanoma skin cancers and possibly other types of cancers. They can also cause high cholesterol levels.
Other immunosuppressive agents
Other immunosuppressive agents, including azathioprine or cyclosporine (an immunomodulatory medication), are less effective and are rarely used because of an increased risk of toxicity. Thus, they are used only for people in whom treatment with more traditional DMARDs has not adequately controlled their symptoms.Other immunosuppressive agents, including azathioprine or cyclosporine (an immunomodulatory medication), are less effective and are rarely used because of an increased risk of toxicity. Thus, they are used only for people in whom treatment with more traditional DMARDs has not adequately controlled their symptoms.
Nonsteroidal anti-inflammatory drugs (NSAIDs)
NSAIDs can be used to treat the symptoms of rheumatoid arthritis. They do not prevent the damage caused by rheumatoid arthritis from progressing and thus should not be considered the primary treatment. (See also table Medications Used to Treat Rheumatoid Arthritis .)
NSAIDs can reduce the swelling in affected joints and relieve pain and stiffness. They can be taken by mouth or applied directly to the skin over painful joints. Rheumatoid arthritis, unlike osteoarthritis, causes considerable inflammation. Thus, medications that decrease inflammation, including NSAIDs, have an important advantage over medications such as acetaminophen that reduce pain but not inflammation. However, NSAIDs should generally not be taken by people who have a history of NSAIDs can reduce the swelling in affected joints and relieve pain and stiffness. They can be taken by mouth or applied directly to the skin over painful joints. Rheumatoid arthritis, unlike osteoarthritis, causes considerable inflammation. Thus, medications that decrease inflammation, including NSAIDs, have an important advantage over medications such as acetaminophen that reduce pain but not inflammation. However, NSAIDs should generally not be taken by people who have a history ofdigestive tract (peptic) ulcers—including stomach ulcers or duodenal ulcers—because NSAIDs can upset the stomach and cause ulcers to bleed. Medications called proton pump inhibitors (such as esomeprazole, lansoprazole, omeprazole, pantoprazole, and rabeprazole) can reduce the risk of stomach or duodenal ulcers (see table —including stomach ulcers or duodenal ulcers—because NSAIDs can upset the stomach and cause ulcers to bleed. Medications called proton pump inhibitors (such as esomeprazole, lansoprazole, omeprazole, pantoprazole, and rabeprazole) can reduce the risk of stomach or duodenal ulcers (see tableMedications Used to Treat Stomach Acid).
Other possible side effects of NSAIDs may include headache, confusion, elevation of blood pressure, worsening of kidney function, swelling, and decreased platelet function, causing bruising or bleeding. People who get hives, inflammation and swelling in the nose, or asthma after they take aspirin may have the same symptoms after taking other NSAIDs. NSAIDs may increase the risk of heart attacks and strokes. The risk appears to be higher if the medication is used at higher doses and for longer periods of time. Other possible side effects of NSAIDs may include headache, confusion, elevation of blood pressure, worsening of kidney function, swelling, and decreased platelet function, causing bruising or bleeding. People who get hives, inflammation and swelling in the nose, or asthma after they take aspirin may have the same symptoms after taking other NSAIDs. NSAIDs may increase the risk of heart attacks and strokes. The risk appears to be higher if the medication is used at higher doses and for longer periods of time.
Aspirin is no longer used to treat rheumatoid arthritis because effective doses are often toxic.
The cyclooxygenase (COX-2) inhibitors (coxibs, such as celecoxib) are NSAIDs that act similarly to the other NSAIDs but are slightly less likely to damage the stomach and do not affect platelet function and cause bruising or bleeding like the other NSAIDs. However, if a person also takes (coxibs, such as celecoxib) are NSAIDs that act similarly to the other NSAIDs but are slightly less likely to damage the stomach and do not affect platelet function and cause bruising or bleeding like the other NSAIDs. However, if a person also takesaspirin, stomach damage is almost as likely to occur as with other NSAIDs. Caution should be taken with use of coxibs and probably all NSAIDs for long periods or by people with risk factors for heart attack and stroke.
Corticosteroids
Corticosteroids are potent anti-inflammatory drugs that suppress the immune system. Corticosteroids, such as prednisone, are the most dramatically effective medications for reducing inflammation and symptoms of rheumatoid arthritis anywhere in the body. (See also table Corticosteroids are potent anti-inflammatory drugs that suppress the immune system. Corticosteroids, such as prednisone, are the most dramatically effective medications for reducing inflammation and symptoms of rheumatoid arthritis anywhere in the body. (See also tableMedications Used to Treat Rheumatoid Arthritis.)
There is some controversy as to whether corticosteroids can slow the progression of rheumatoid arthritis. Furthermore, the long-term use of corticosteroids almost invariably leads to side effects, potentially involving almost every organ in the body (see Corticosteroids: Uses and Side Effects). Consequently, doctors usually reserve corticosteroids for short-term use in the following situations:
When beginning treatment for severe symptoms (until a DMARD has taken effect)
In severe flare-ups when many joints are affected
They are also useful in treating rheumatoid inflammation outside of joints, for example, in the membranes covering the lungs (pleura) or in the sac surrounding the heart (pericardium).
Because of the risk of side effects, the lowest effective dose is almost always used. When corticosteroids are injected into a joint, the person does not get the same side effects as when taking a corticosteroid by mouth (orally) or vein (intravenously). Corticosteroids can be injected directly into affected joints for fast, short-term relief of pain and swelling.
When used for a long time, corticosteroids may cause weight gain, high blood pressure, diabetes, thinning and bruising of the skin, glaucoma and other eye problems such as cataracts, and increase the risk of certain infections.
Corticosteroids: Uses and Side Effects
Corticosteroids are the strongest medications available for reducing inflammation in the body. They are useful in any condition in which inflammation occurs, including rheumatoid arthritis and other connective tissue disorders, multiple sclerosis, and in emergencies such as brain swelling due to cancer, asthma attacks, and severe allergic reactions. When inflammation is severe, use of these medications is often lifesaving. Corticosteroids can be
For example, corticosteroids can be used as an inhaled preparation for treatment of asthma. They can be used as a nasal spray to treat hay fever (allergic rhinitis). They can be used as eye drops to treat eye inflammation (uveitis). They may be applied directly to an affected area for treatment of certain skin conditions such as eczema and psoriasis. They can be injected into joints inflamed by rheumatoid arthritis or another disorder. Corticosteroids are prepared synthetically to have the same action as cortisol (or cortisone), a steroid hormone produced by the outer layer (cortex) of the adrenal glands—hence the name “corticosteroid.” Many synthetic corticosteroids are, however, more powerful than cortisol, and most are longer acting. Corticosteroids are chemically related to, but have different effects than, anabolic steroids (such as testosterone) that are produced by the body and sometimes abused by athletes. Examples of corticosteroids are prednisone, dexamethasone, triamcinolone, betamethasone, beclomethasone, flunisolide, and fluticasone. All of these medications are very strong (although strength depends on the dose used). Hydrocortisone is a milder corticosteroid that is available in over-the-counter skin creams.Examples of corticosteroids are prednisone, dexamethasone, triamcinolone, betamethasone, beclomethasone, flunisolide, and fluticasone. All of these medications are very strong (although strength depends on the dose used). Hydrocortisone is a milder corticosteroid that is available in over-the-counter skin creams. Corticosteroids reduce the body’s ability to fight infections by reducing inflammation, typically when they are taken by mouth or given by vein. Because of this side effect, they are used with extreme care when infections are present. Oral and intravenous use may cause or worsen high blood pressure, heart failure, diabetes, peptic ulcers, and osteoporosis. Therefore, corticosteroids are used in such conditions only when their benefit is likely to exceed their risk. When they are taken by mouth or by injection for more than about 2 weeks, corticosteroids should not be stopped abruptly. This is because corticosteroids inhibit the production of cortisol by the adrenal glands, and this production must be given time to recover. Thus, at the end of a course of corticosteroids, the dose is gradually reduced. It is important for a person who takes corticosteroids to follow the doctor’s instructions on dosage very carefully. The long-term use of corticosteroids, particularly at higher doses and particularly when given by mouth or vein, invariably leads to many side effects, involving almost every organ in the body. Common side effects include thinning of the skin with stretch marks and bruising, high blood pressure, elevated blood sugar levels, cataracts, puffiness in the face (moon face) and abdomen, thinning of the arms and legs, poor wound healing, stunted growth in children, loss of calcium from the bones (which can lead to osteoporosis), hunger, weight gain, and mood swings. Inhaled corticosteroids and corticosteroids that are applied directly to the skin have far fewer side effects than corticosteroids given by mouth, vein, or injection. |
Prognosis for Rheumatoid Arthritis
Rheumatoid arthritis decreases life expectancy; however, this effect has been decreasing over time as treatments improve, and the difference appears to be very small. The major causes of death among patients with rheumatoid arthritis appear to be respiratory conditions (for example, interstitial lung disease and pneumonia), cardiovascular disease, and cancer. Side effects of treatment with immunosuppressive agents (for example, infection and increased cancer risk) may be responsible. Rarely, rheumatoid arthritis resolves spontaneously.
Although the majority of people experience improvement with treatment, less than half of people are likely to experience sustained remissions. At least 10% of people with rheumatoid arthritis are eventually severely disabled despite full treatment. Factors that tend to predict a poorer prognosis include the following:
Being White, a woman, or both
Having rheumatoid nodules
Being older when the disorder begins
Having inflammation in 20 or more joints
Being a cigarette smoker
Obesity
Having a high erythrocyte sedimentation rate (ESR)
Having high levels of rheumatoid factor or anti-cyclic citrullinated peptide (anti-CCP) antibodies
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
Arthritis Foundation: Information about rheumatoid arthritis and other types of arthritis and available treatments, lifestyle tips, and other resources







