



- Overview of Fractures
- Pediatric Physeal (Growth Plate) Fractures
- Clavicle Fractures
- Proximal Humeral Fractures
- Distal Humeral Fractures
- Radial Head Fractures
- Ulnar and Radial Shaft Fractures
- Distal Radius Fractures
- Isolated Olecranon Fractures
- Scaphoid (Navicular) Fractures
- Metacarpal Neck Fractures
- Fingertip Fractures
- Vertebral Compression Fractures
- Pelvic Fractures
- Hip Fractures
- Femoral Shaft Fractures
- Ankle Fractures
- Calcaneal Fractures
- Fracture-Dislocation of the Midfoot (Lisfranc Injury)
- Fractures of the 5th Metatarsal Bone
- Toe Fractures
- Compartment Syndrome
Hip fractures may occur in the head, neck, or area between or below the trochanters (prominences) of the femur. These fractures are most common among older patients, particularly those with osteoporosis, and usually result from ground level falls. Diagnosis is by radiographs or, if needed, MRI. Treatment is usually with open reduction with internal fixation (ORIF) or sometimes hemiarthroplasty or total hip arthroplasty.


")
(See also Overview of Fractures.)
Most hip fractures result from falls, but in older people, seemingly minimal force (eg, rolling over in bed, getting up from a chair, walking) can result in fracture, usually because osteoporosis has weakened the bone.
Fracture locations include
Femoral head
Femoral neck (subcapital)
Intertrochanteric
Subtrochanteric
Subcapital and intertrochanteric fractures are the most common types.
Complications of hip fractures include
Osteonecrosis of the femoral head
Fracture nonunion
Complications are more common among older patients with a displaced femoral neck fracture.
In patients with femoral neck fractures, risk of osteonecrosis is increased because the fracture often disrupts the blood supply to the femoral head.
Symptoms and Signs of Hip Fractures
Hip fractures most often result in groin pain and inability to ambulate. Sometimes pain is referred to the knee and is thus misinterpreted as a knee abnormality. Similarly, pubic ramus fractures can cause groin pain.
Patients with displaced fractures cannot walk and have significant pain; the affected leg may appear shortened and externally rotated. In contrast, patients with impacted fractures may be able to walk and have only mild pain and no visible deformity. However, such patients are usually unable to flex the entire lower limb against resistance with the knee extended.
Passive hip rotation with the knee flexed aggravates the pain, helping to distinguish hip fracture from extra-articular disorders such as trochanteric bursitis.
Diagnosis of Hip Fractures
Radiographs
Rarely MRI or CT


CAVALLINI JAMES/BSIP/SCIENCE PHOTO LIBRARY


SCIENCE PHOTO LIBRARY
Diagnosis of a suspected hip fracture begins with an anteroposterior pelvis radiograph and a cross-table lateral view. If a fracture is identified, radiographs of the entire femur should be done. Subtle evidence of fracture (eg, as when fractures are minimally displaced or impacted) can include irregularities in femoral neck trabecular density or bone cortex. However, radiographs are occasionally normal, particularly in patients with subcapital fractures or severe osteoporosis.
If a fracture is not seen on radiographs but is still suspected clinically, MRI is the preferred next imaging study. MRI is more sensitive than CT, which can miss up to 30% of acute fractures.
Pearls & Pitfalls
|
Treatment of Hip Fractures
Usually open reduction with internal fixation (ORIF)
Sometimes femoral head replacement or total hip replacement
The vast majority of hip fractures are treated surgically to minimize the duration of pain and to avoid prolonged bed rest, which is required after nonsurgical treatment and which increases the risk of serious complications (eg, deep venous thrombosis, pressure ulcers, deconditioning, pneumonia, death), particularly in older patients.
Rehabilitation is started as soon as possible after treatment of a hip fracture.
Prophylactic anticoagulation may reduce the incidence of venous thrombosis after hip fracture (1).
In the emergency department, older patients with hip fractures may be in pain while they are waiting for cardiac clearance for hip surgery. Femoral nerve blocks and fascia iliaca compartment blocks can be used to control pain in older patients with isolated hip fractures. Pain can be controlled for up to 6 to 8 hours, and patients do not need opioids, which have more systemic adverse effects (eg, respiratory depression). Contraindications to regional nerve blocks include bleeding disorders and coagulopathies (2).
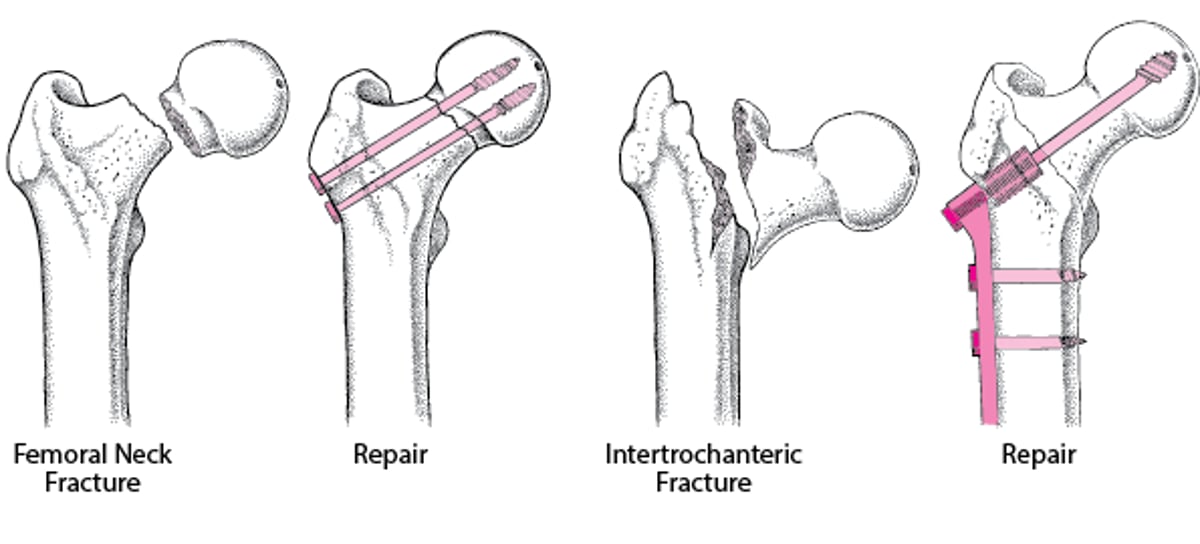
Femoral Neck Fractures
Nondisplaced and impacted femoral neck fractures in older patients and all femoral neck fractures in younger patients are typically treated with ORIF.
Displaced femoral neck fractures in older patients are usually treated with hip arthroplasty (replacement) to allow early unrestricted weight-bearing and to minimize the likelihood that additional surgery will be required. Older patients who walk very little and thus put little stress on the hip joint are usually treated with hemiarthroplasty (only the proximal femur is replaced); more active older patients are increasingly being treated with total hip arthroplasty (the proximal femur is replaced, and the acetabulum is resurfaced). Total hip arthroplasty surgery is more extensive and poses greater risk but results in better function.
Intertrochanteric fractures
Intertrochanteric fractures are usually treated with ORIF (see figure Open Reduction With Internal Fixation [ORIF]).
Open Reduction With Internal Fixation (ORIF)

Treatment references
1. Steele N, Dodenhoff RM, Ward AJ, Morse MH. Thromboprophylaxis in pelvic and acetabular trauma surgery. The role of early treatment with low-molecular-weight heparin. . Thromboprophylaxis in pelvic and acetabular trauma surgery. The role of early treatment with low-molecular-weight heparin.J Bone Joint Surg Br. 2005;87(2):209-212. doi:10.1302/0301-620x.87b2.14447
2. Haines L, Dickman E, Ayvazyan S, et al. Ultrasound-guided fascia iliaca compartment block for hip fractures in the emergency department. J Emerg Med. 43 (4):692–697, 2012. doi: 10.1016/j.jemermed.2012.01.050
Key Points
Hip (particularly subcapital and intertrochanteric) fractures are common among older patients with osteoporosis.
Osteonecrosis of the femoral head, fracture nonunion, and osteoarthritis are common complications.
If circumstances suggest a hip fracture and patients cannot flex the entire lower limb against resistance with the knee extended, suspect an impacted fracture, even if patients have only mild pain and can walk.
For all patients with unexplained hip or knee pain and difficulty walking due to pain, rotate their hip with their knee flexed; if this maneuver aggravates the pain, hip fracture is possible.
If a fracture is suspected based on clinical findings but is not seen on radiographs, obtain MRI.
Treat most fractures surgically (ORIF or hip arthroplasty) so that patients can walk as soon as possible.
Consider using femoral nerve blocks and fascia iliaca compartment blocks instead of opioids for short-term pain control, particularly in older patients with isolated hip fractures.







