



Topic Resources











A dislocation is complete separation of the 2 bones that form a joint. Subluxation is partial separation. Often, a dislocated joint remains dislocated until reduced (realigned) by a clinician, but sometimes it reduces spontaneously.
In addition to dislocations, musculoskeletal injuries include the following:
Musculoskeletal injuries are common and vary greatly in mechanism, severity, and treatment. The extremities, spine, and pelvis can all be affected.
Musculoskeletal injuries may occur in isolation or as part of multisystem trauma (see Approach to the Trauma Patient). Most musculoskeletal injuries result from blunt trauma, but penetrating trauma can also damage musculoskeletal structures.
Spinal trauma can cause dislocations or subluxation; nontraumatic spinal subluxation can also occur. Mandibular dislocation can occur spontaneously.
Dislocations may be open (in communication with the environment via a skin wound) or closed.
Prognosis and treatment vary greatly depending on the location and severity of the dislocation.
Complications
Serious complications of dislocations are unusual but may threaten life or limb viability or cause permanent limb dysfunction. Risk of complications is high with open dislocations (which predispose to infection) and with dislocations that disrupt blood vessels, tissue perfusion, and/or nerves. Dislocations, particularly if not rapidly reduced, tend to have a higher risk of vascular and nerve injuries than do fractures. Closed dislocations that do not involve blood vessels or nerves, particularly those that are quickly reduced, are least likely to result in serious complications.
Acute complications (associated injuries) of dislocations include the following:
Fractures: Fractures may accompany a dislocation (eg, shoulder dislocation and fracture of the greater tuberosity).
Bleeding: Bleeding accompanies all significant soft-tissue injuries.
Vascular injuries: Some closed dislocations, particularly knee or hip dislocations, disrupt the vascular supply sufficiently to cause distal limb ischemia; this vascular disruption may be clinically occult for hours after the injury.
Nerve injuries: Nerves may be injured when stretched by a dislocated joint. Depending on the cause of the dislocation, nerves may be bruised, crushed, or torn. When nerves are bruised (called neurapraxia), nerve conduction is blocked, but the nerve is not torn. Neurapraxia causes temporary motor and/or sensory deficits; neurologic function returns completely in about 6 to 8 weeks. When nerves are crushed (called axonotmesis), the axon is injured, but the myelin sheath is not. This injury is more severe than neurapraxia. Depending on the extent of the damage, the nerve can regenerate over weeks to years. Usually, nerves are torn (called neurotmesis) only in open dislocations. Torn nerves do not heal spontaneously and may have to be repaired surgically.
Infection: Any injury can become infected, but risk is highest with those that are open or surgically treated. Acute infection can lead to osteomyelitis, which is a bone infection that can be difficult to cure.
Long-term complications of dislocations include the following:
Instability: Various dislocations can lead to joint instability. Instability can be disabling and increases the risk of osteoarthritis.
Stiffness and impaired range of motion: Stiffness is more likely if a joint needs prolonged immobilization. The knee, elbow, and shoulder are particularly prone to posttraumatic stiffness, especially in older patients.
Osteonecrosis: Osteonecrosis occurs primarily when the vascular supply is damaged. Dislocations of a native (not prosthetic) hip are prone to osteonecrosis. The incidence of osteonecrosis after hip dislocation is related to the severity of the initial injury and is higher if the dislocation is not promptly reduced.
Osteoarthritis: Dislocations that disrupt the weight-bearing surfaces of joints or that result in joint malalignment and instability predispose to joint cartilage degeneration and osteoarthritis.
Evaluation of Dislocations
Evaluation for serious injuries
History and physical examination
X-rays
Sometimes MRI or CT
Sometimes a dislocation is clinically obvious, but in other cases (eg, a shoulder deformity in an adolescent), dislocations must be distinguished from fractures and other injuries.
In the emergency department, if the mechanism of injury suggests potentially severe or multiple injuries (as in a high-speed motor vehicle crash or fall from a height), patients are first evaluated from head to toe for serious injuries to all organ systems and, if needed, are resuscitated (see Approach to the Trauma Patient). Patients, especially if a hip dislocation is suspected, are evaluated for hemorrhagic shock due to occult blood loss. If a limb is injured, it is immediately evaluated for open wounds and symptoms or signs of neurovascular injury (numbness, paresis, poor perfusion) and compartment syndrome (eg, pain out of proportion to injuries, pallor, paresthesias, coolness, pulselessness).
Patients should be checked for fractures and other musculoskeletal injuries as well as dislocations; sometimes parts of this evaluation are deferred until fracture is excluded.
The joint above and below the dislocated joint should also be examined.
Some dislocations can be diagnosed clinically, but x-rays are usually still taken.
History
The mechanism (eg, the direction and magnitude of force) may suggest the type of injury. However, many patients do not remember or cannot describe the exact mechanism.
If a patient reports a deformity that has resolved before the patient is medically evaluated, the deformity should be assumed to be a true deformity that spontaneously reduced.
Physical examination
Examination includes
Vascular and neurologic assessment
Inspection for open wounds, deformity, swelling, ecchymoses, and decreased or abnormal motion
Palpation for tenderness, crepitation, and gross defects in bone or tendon
Examination of the joints above and below the injured area
Sometimes for subluxations, stress testing of the affected joints for instability
If muscle spasm and pain limit physical examination (particularly for stress testing), examination is sometimes easier after the patient is given a systemic analgesic or local anesthetic. Or the injury can be immobilized until muscle spasm subsides, usually for a few days, and then the patient can be reexamined.
Certain findings may indicate a dislocation or another musculoskeletal injury.
If a wound is near a dislocation, the dislocation is assumed to be open.
Deformity may indicate dislocation or subluxation (partial separation of bones in a joint), but it may also indicate fracture.
Swelling commonly indicates a significant musculoskeletal injury but may require several hours to develop.
Tenderness accompanies nearly all musculoskeletal injuries, and for many patients, palpation anywhere around the injured area causes discomfort.
Gross joint instability suggests dislocation or severe ligamentous disruption.
Stress testing may be done to evaluate the stability of an injured joint; however, if a fracture is suspected, stress testing is deferred until x-rays exclude fracture. Bedside stress testing involves passively opening the joint in a direction usually perpendicular to the normal range of motion (stressing). Because muscle spasm during acutely painful injuries may mask joint instability, the surrounding muscles are relaxed as much as possible, and examinations are begun gently, then repeated, with slightly more force each time. Findings are compared with those for the opposite, normal side but can be limited by their subjective nature. For all proximal interphalangeal (PIP) joint dislocations, stress testing is done after the dislocation is reduced.
If muscle spasm is severe despite use of analgesia or anesthetic injection, the examination should be repeated a few days later, when the spasm has subsided.
Attention to certain areas during examination can help detect commonly missed injuries (see table Examination for Some Commonly Missed Dislocations and Upper-Extremity Musculoskeletal Injuries).
Examination for Some Commonly Missed Dislocations and Upper-Extremity Musculoskeletal Injuries
Symptom | Characteristic History | Physical Finding | Injury |
|---|---|---|---|
Shoulder pain | Seizure Electric shock | Restriction of passive external rotation with the elbow flexed | Posterior shoulder (glenohumeral) dislocation, possibly bilateral |
History of shoulder dislocation, trauma, or overuse in patients > 40 | Inability to maintain a position at 90° of abduction when slight downward pressure is applied (drop-arm test) | Acute complete rotator cuff tear | |
Various mechanisms (eg, pile-on injury in football, direct blow to joint) | Tenderness over the sternoclavicular joint | Sternoclavicular joint injury | |
Most often, fall on the point of the shoulder | Tenderness over the acromioclavicular area | Acromioclavicular strain or disruption (shoulder separation) | |
Wrist pain or swelling | Fall on an outstretched hand | Tenderness over the anatomic snuffbox (located just distal to the radius, between the extensor pollicis longus, extensor pollicis brevis, and abductor pollicis longus tendons) | |
Various mechanisms | Tenderness over the lunate fossa (in the wrist at the base of the 3rd metacarpal) and pain with axial compression of the 3rd metacarpal | Lunate fracture | |
For other commonly missed injuries, see tables Examination for Some Commonly Missed Fractures and Examination for Some Commonly Missed Soft-Tissue Injuries. | |||
If physical examination is normal in a joint that patients identify as painful, the cause may be referred pain. For example, patients with a slipped capital femoral epiphysis (or less often hip fracture) may feel pain in their knee.
Imaging
Not all limb injuries require imaging. If imaging is needed, x-rays are usually done first.
Plain x-rays show primarily bone and thus are useful for diagnosing dislocations. They should include at least 2 views taken in different planes (usually anteroposterior and lateral views).
Additional views (eg, oblique) may be done when
The evaluation suggests fracture and 2 projections are negative.
They are routine for certain joints (eg, a mortise view for evaluating an ankle, an oblique view for evaluating a foot).
Certain abnormalities are suspected (eg, Y view of the shoulder when posterior dislocation is suspected).
For lateral views of digits, the digit of interest should be separated from the others.
MRI or CT may be done to check for subtle fractures, which may accompany a dislocation.
Other tests are done to check for related injuries:
Arteriography or CT angiography to check for suspected arterial injuries (eg, possible popliteal artery injury in patients with a knee dislocation)
Electromyography and/or nerve conduction studies to check for suspected nerve damage (usually done as an outpatient procedure and not done in the acute setting)
Treatment of Dislocations
Treatment of associated injuries
Reduction as indicated, splinting, and analgesia
RICE (rest, ice, compression, and elevation) or PRICE (including protection) as indicated
Usually immobilization
Sometimes surgery
Most joint dislocations can be reduced (returned to the normal anatomic position) without surgery. Occasionally, dislocations cannot be reduced using closed manipulative techniques, and open surgery is required. Once a joint is reduced, additional surgery is often not necessary, However, surgery is sometimes required to manage associated fractures, debris in the joint, or residual instability.
Initial treatment
Serious associated problems, if present, are treated first.
Injuries to arteries are surgically repaired unless they affect only small arteries with good collateral circulation. Compartment syndrome is treated.
Severed nerves are surgically repaired; for neuropraxia and axonotmesis, initial treatment is usually observation, supportive measures, and sometimes physical therapy.
Suspected open dislocations require sterile wound dressings, tetanus prophylaxis, broad-spectrum antibiotics (eg, a 2nd-generation cephalosporin plus an aminoglycoside), and surgery to irrigate and debride them (and thus prevent infection).
Most moderate and severe dislocations, particularly grossly unstable ones, are immobilized immediately by splinting (immobilization with a nonrigid or noncircumferential device) to decrease pain and to prevent further injury to soft tissues by unstable injuries.
Pain is treated as soon as possible, typically with opioids and/or nonsteroidal anti-inflammatory drugs (NSAIDs).
After initial treatment, dislocations are reduced, immobilized, and treated symptomatically as indicated.
Dislocations may require surgical repair if
Structures supporting the joint are damaged.
A joint remains unstable after reduction.
Reduction
Dislocations are reduced.
Closed reduction (by manipulation, without skin incision) is done when possible; sedation may be required. If closed reduction is not possible, open reduction (with skin incision) is done; anesthesia is required.
Dislocations typically require a cast, splint, sling, or another device (eg, external fixator for the knee) to maintain reduction.
PRICE
Patients with a joint dislocation may benefit from PRICE (protection, rest, ice, compression, elevation), although this practice is not supported by strong evidence.
Protection helps prevent further injury. It may involve limiting the use of an injured part, applying a splint or cast, or using crutches.
Rest may prevent further injury and speed healing.
Ice and compression may minimize swelling and pain. Ice is enclosed in a plastic bag or towel and applied intermittently during the first 24 to 48 hours (for 15 to 20 minutes, as often as possible). Injuries can be compressed by a splint, an elastic bandage, or, for certain injuries likely to cause severe swelling, a Jones compression dressing. The Jones dressing is 4 layers; layers 1 (the innermost) and 3 are cotton batting, and layers 2 and 4 are elastic bandages.
Elevating the injured limb above the heart for the first 2 days in a position that provides an uninterrupted downward path; such a position allows gravity to help drain edema fluid and minimize swelling.
After 48 hours, periodic application of warmth (eg, a heating pad) for 15 to 20 minutes may relieve pain and speed healing.
Immobilization
Immobilization decreases pain and facilitates healing by preventing further injury. Joints proximal and distal to the injury should be immobilized.
A cast is usually used for fractures or other injuries that require weeks of immobilization. Rarely, swelling under a cast is severe enough to contribute to compartment syndrome. If clinicians suspect severe swelling under a cast, the cast (and all padding) is cut open from end to end medially and laterally (bivalved).
Patients with casts should be given written instructions, including the following:
Keep the cast dry.
Never put an object inside the cast.
Inspect the cast’s edges and skin around the cast every day and report any red or sore areas.
Pad any rough edges with soft adhesive tape, cloth, or other soft material to prevent the cast’s edges from injuring the skin.
When resting, position the cast carefully, possibly using a small pillow or pad, to prevent the edge from pinching or digging into the skin.
Elevate the cast whenever possible to control swelling.
Seek medical care immediately if pain persists or the cast feels excessively tight.
Seek medical care immediately if an odor emanates from within the cast or if a fever, which may indicate infection, develops.
Seek care immediately for progressively worsening pain or any new numbness or weakness (which may indicate compartment syndrome).
Good hygiene is important.
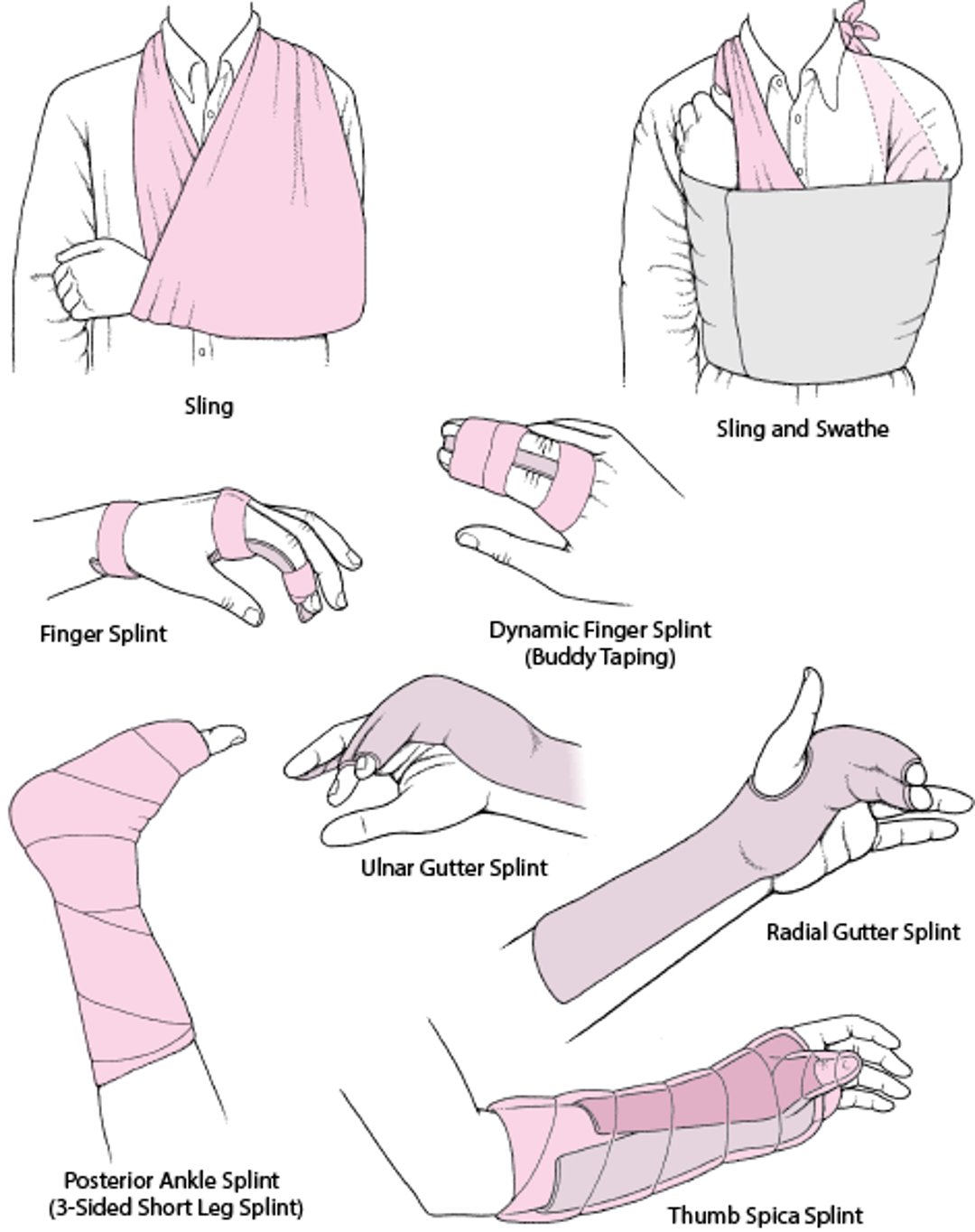
Joint Immobilization as Acute Treatment: Some Commonly Used Techniques



© Elsevier Inc. All Rights Reserved.
This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.

© Elsevier Inc. All Rights Reserved.
This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.









© Elsevier Inc. All Rights Reserved.
This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.

© Elsevier Inc. All Rights Reserved.
This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.






A splint (see figure Joint immobilization as acute treatment: Some commonly used techniques) can be used to immobilize some stable dislocations. A splint is noncircumferential; thus, it enables patients to apply ice and to move to some degree. Also, it allows for some swelling, so it does not contribute to compartment syndrome. Some dislocations that ultimately require casting are immobilized initially with a splint until most of the swelling resolves.
A sling provides some degree of support and limits mobility; it can be useful for dislocations that are adversely affected by complete immobilization (eg, for shoulder dislocations, which, if completely immobilized, can rapidly lead to adhesive capsulitis [frozen shoulder]).
A swathe (a piece of cloth or a strap) may be used with a sling to prevent the arm from swinging outward, especially at night. The swathe is wrapped around the back and over the injured part.
Prolonged immobilization (>3 to 4 weeks for young adults) of a joint can cause stiffness, contractures, and muscle atrophy. These complications may develop rapidly and may be permanent, particularly in older patients. Resumption of active motion within the first few days or weeks may minimize contractures and muscle atrophy, thus accelerating functional recovery. Physical therapists can advise patients about what they can do during immobilization to maintain as much function as possible (eg, elbow, wrist, and hand range-of-motion exercises if the shoulder is immobilized). After immobilization, physical therapists can provide patients with exercises to improve range of motion and muscle strength, strengthen and stabilize the injured joint, and thus help prevent recurrence and long-term impairment.
Geriatrics Essentials
Older patients are predisposed to dislocations (and other musculoskeletal injuries) because of the following:
A tendency to fall frequently (eg, due to age-related loss of proprioception, adverse effects of drugs on proprioception or postural reflexes, or orthostatic hypotension)
Impaired protective reflexes during falls
For any musculoskeletal injury in older patients, the goal of treatment is rapid return to activities of daily living.
Immobility (eg, joint immobilization) is more likely to have adverse effects in older patients. Early mobilization and physical therapy are essential to recovery of function.
Coexisting disorders (eg, arthritis) can interfere with recovery.
Key Points
Dislocations that disrupt arterial supply and compartment syndrome threaten limb viability and may ultimately threaten life.
Check for fractures and ligament, tendon, and muscle injuries as well as dislocations (sometimes part of this evaluation is deferred until fracture is excluded).
Examine the joints above and below the injured area.
Consider referred pain, particularly if physical findings are normal in a joint that patients identify as painful (eg, shoulder pain in patients with sternoclavicular injuries).
Take x-rays to diagnose associated fractures as well as dislocations.
Immediately treat any serious associated injuries, splint unstable dislocations, and, as soon as possible, treat pain and reduce dislocations.
Immobilize all dislocations as soon as they are reduced using a cast, splint, sling, or other device.
Provide patients with explicit, written instructions about cast care.
Choose treatments that make early mobilization possible, and encourage patients, especially those who are older, to do the recommended exercises to improve range of motion and muscle strength and to prevent future dislocations.







