


Lyme disease is a tick-transmitted infection caused by the spirochete Borrelia species. Early symptoms include an erythema migrans rash, which may be followed weeks to months later by neurologic, cardiac, or joint abnormalities. Diagnosis is primarily clinical in early-stage disease, but serologic testing can help diagnose cardiac, neurologic, and rheumatologic complications that occur later in the disease. Treatment is with antibiotics such as doxycycline or ceftriaxone.
Spirochetes are distinguished by the helical shape of the bacteria. Pathogenic spirochetes include Treponema, Leptospira, and Borrelia. Both Treponema and Leptospira are too thin to be seen using brightfield microscopy but are clearly seen using darkfield or phase microscopy. Borrelia are thicker and can also be stained and seen using brightfield microscopy (1).
General reference
1. Cleveland DW, Anderson CC, Brissette CA: Borrelia miyamotoi: A Comprehensive Review. Pathogens 12(2):267, 2023. doi:10.3390/pathogens12020267
Epidemiology of Lyme Disease
Lyme disease was recognized in 1976 because of close clustering of cases in Lyme, Connecticut, and it is the most commonly reported tick-borne illness in the United States. It has been reported in 49 states, but > 90% of cases occur from Maine to Virginia and in Wisconsin, Minnesota, and Michigan (1). On the West Coast, most cases occur in northern California and Oregon. Lyme disease also occurs in Europe, across the former Soviet Union, and in China and Japan.
In the United States, Lyme disease is caused primarily by Borrelia burgdorferi and to a lesser extent by B. mayonii, which has recently been found in the upper midwestern states. In Europe and Asia, Lyme disease is caused primarily by B. afzelii, B. garinii, and B. burgdorferi. Onset is usually in the summer and early fall. Most patients are children and young adults living in heavily wooded areas or who walk through tall grass or wooded areas.
Lyme disease is transmitted primarily by 4 Ixodes species worldwide:
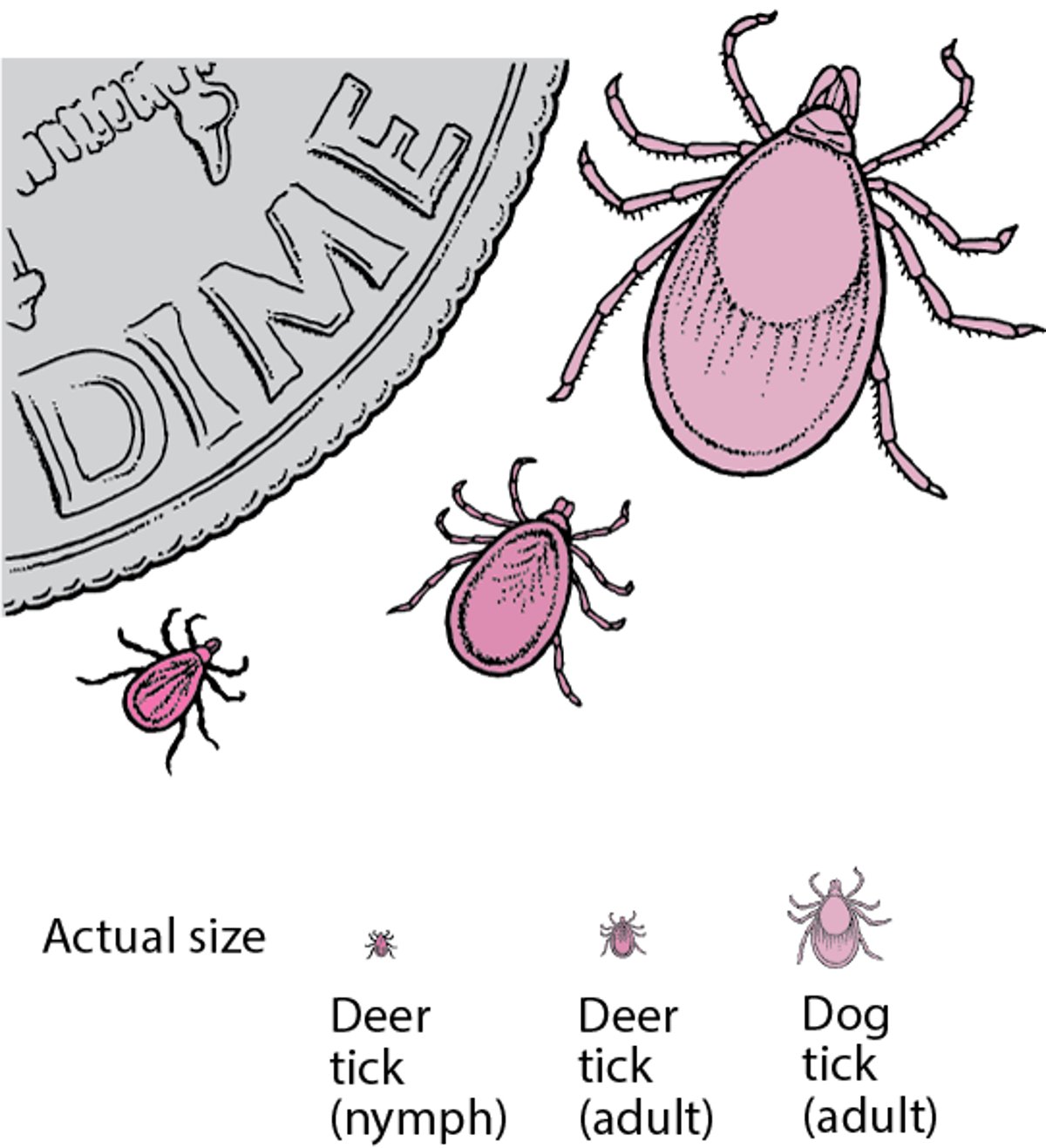
I. scapularis (the deer tick) in the northeastern and north central United States
I. pacificus in the western United States
I. ricinus in Europe
I. persulcatus in Asia
In the United States, the white-footed mouse is the primary animal reservoir for B. burgdorferi and the preferred host for nymphal and larval forms of the deer tick. Deer are hosts for adult ticks but do not carry Borrelia. Other mammals (eg, dogs) can be incidental hosts and can develop Lyme disease. In Europe, larger mammals such as sheep are hosts for the adult tick.


Image courtesy of James Gathany via the Public Health Image Library of the Centers for Disease Control and Prevention.
Deer Ticks

Epidemiology reference
1. Mead PS: Epidemiology of Lyme disease. Infect Dis Clin North Am 29(2):187–210, 2015. doi:10.1016/j.idc.2015.02.010
Pathophysiology of Lyme Disease
B. burgdorferi enters the skin at the site of the tick bite. After 3 to 32 days, the organisms migrate locally in the skin around the bite, spread via the lymphatics to cause regional adenopathy or disseminate in blood to organs or other skin sites. Initially, an inflammatory reaction (erythema migrans) occurs before significant antibody response to infection (serologic conversion).
Symptoms and Signs of Lyme Disease
Lyme disease has 3 stages:
Early localized
Early disseminated
Late
The early and late stages are usually separated by an asymptomatic interval.


Erythema migrans is the characteristic physical finding of early Lyme disease. It begins as a red macule at the site of the Ixodes tick bite. Classically, the macule expands with central clearing, as in this image, but, in many patients, no central clearing occurs. Some patients have central erythema surrounded by a pale ring, and a few develop vesicular or ulcerated centers.
Image courtesy of Thomas Habif, MD.


Erythema migrans may manifest as a rash with central erythema surrounded by a pale ring.
LARRY MULVEHILL/SCIENCE PHOTO LIBRARY


Erythema migrans can resemble a bull's eye, with central erythema surrounded by a pale ring and outer erythematous halo.
CDC/SCIENCE PHOTO LIBRARY
Erythema migrans is the characteristic physical finding of early Lyme disease. It begins as a red macule at the site of the Ixodes tick bite. Classically, the macule expands with central clearing, as in this image, but, in many patients, no central clearing occurs. Some patients have central erythema surrounded by a pale ring, and a few develop vesicular or ulcerated centers.
Image courtesy of Thomas Habif, MD.
Erythema migrans may manifest as a rash with central erythema surrounded by a pale ring.
LARRY MULVEHILL/SCIENCE PHOTO LIBRARY
Erythema migrans can resemble a bull's eye, with central erythema surrounded by a pale ring and outer erythematous halo.
CDC/SCIENCE PHOTO LIBRARY
Early-localized stage
Erythema migrans, the hallmark and best clinical indicator of Lyme disease, is the first sign of the disease. It occurs in at least 75% of patients, beginning as a red or dark macule or papule at the site of the tick bite, usually on the proximal portion of an extremity or the trunk (especially the thigh, buttock, or axilla), between 3 days and 32 days after a tick bite. Because tick nymphs are so small, most patients do not realize that they have been bitten.
The area expands, often with clearing between the center and periphery resembling a bull’s eye, to a diameter ≤ 50 cm. Darkening erythema may develop in the center, which may be hot to the touch and indurated. Without therapy, erythema migrans typically fades within 3 to 4 weeks.
Many patients with erythema migrans have a single lesion. Some patients develop multiple erythema migrans lesions, which are signs of early hematogenous dissemination (1). Mucosal lesions do not occur. Apparent recurrences of erythema migrans lesions after treatment are caused by reinfection, rather than relapse, because the genotype identified in the new lesion differs from that of the original infecting organism.
Early-disseminated stage
Symptoms of early-disseminated disease begin days or weeks after the appearance of the primary lesion, when the bacteria spread through the body. Soon after onset, nearly half of untreated patients develop multiple, usually smaller annular secondary skin lesions without indurated centers. Cultures of biopsy samples of these secondary lesions have been positive, indicating dissemination of infection.
Patients also develop a musculoskeletal, flu-like syndrome, consisting of malaise, fatigue, chills, fever, headache, stiff neck, myalgias, and arthralgias that may last for weeks. Because symptoms are often nonspecific, the diagnosis is frequently missed if erythema migrans is absent; a high index of suspicion is required. Frank arthritis is rare at this stage. Less common are backache, nausea and vomiting, sore throat, lymphadenopathy, and splenomegaly.
Symptoms are characteristically intermittent and changing, but malaise and fatigue may linger for weeks. Resolved skin lesions may reappear faintly, sometimes before recurrent attacks of arthritis, in late-stage disease.
Neurologic abnormalities develop in about 15% of patients within weeks to months of erythema migrans (generally before arthritis occurs), commonly last for months, and usually resolve completely. Most common are lymphocytic meningitis (cerebrospinal fluid [CSF] pleocytosis of about 100 cells/mcL) or meningoencephalitis, cranial neuritis (especially Bell palsy, which may be bilateral), and sensory or motor radiculoneuropathies, alone or in combination.
Myocardial abnormalities occur in about 8% of patients within weeks of erythema migrans. They include fluctuating degrees of atrioventricular block (first-degree, Wenckebach, or third-degree) and, rarely, myopericarditis with chest pain, reduced ejection fractions, and cardiomegaly.
Late-stage disease
In untreated Lyme disease, the late stage begins months to years after initial infection. Arthritis develops in about 60% of patients within several months, occasionally up to 2 years, of disease onset (as defined by erythema migrans). Intermittent swelling and pain in a few large joints, especially the knees, typically recur for several years. Affected knees commonly are much more swollen than painful; they are often hot but rarely erythematous. Baker cysts may form and rupture. Malaise, fatigue, and low-grade fever may precede or accompany arthritis attacks. In about 10% of patients, knee involvement is chronic (unremittent for ≥ 6 months).
Other late findings (occurring years after onset) include an antibiotic-sensitive skin lesion (acrodermatitis chronica atrophicans) and chronic central nervous system abnormalities, either polyneuropathy or a subtle encephalopathy with mood, memory, and sleep disorders.
Some patients have symptoms such as fatigue, headache, joint and muscle aches, and cognitive problems after successful antibiotic treatment. These symptoms are collectively referred to as post-treatment Lyme disease syndrome (PTLDS) (2). Although some patients with such subjective symptoms are assigned the diagnosis of chronic Lyme disease, there is no clear evidence that these patients have viable Borrelia remaining in their body. The cause of these continuing symptoms is unclear, and treatment with more antibiotics does not help.
Symptoms and signs references
1. Nadelman RB, Hanincová K, Mukherjee P, et al: Differentiation of reinfection from relapse in recurrent Lyme disease. N Engl J Med 367(20):1883–1890, 2012. doi: 10.1056/NEJMoa1114362
2. Maksimyan S, Syed MS, Soti V: Post-Treatment Lyme Disease Syndrome: Need for Diagnosis and Treatment. Cureus 13(10):e18703, 2021. doi:10.7759/cureus.18703
Diagnosis of Lyme Disease
Clinical evaluation, supported by acute and convalescent serologic testing
Erythema migrans is usually diagnosed clinically because it develops before serologic tests become positive (1, 2, 3).
Cultures of blood and relevant body fluids (eg, CSF, joint fluid) may be obtained, primarily to diagnose other pathogens.
Acute (IgM) and convalescent (IgG) antibody titers 2 weeks apart may be helpful (4); positive enzyme-linked immunosorbent assay (C6 ELISA) titers should be confirmed by a second enzyme immunoassay (EIA) or Western blot test. However, seroconversion may be late (eg, > 4 weeks) or occasionally absent (eg, if patients received prior antibiotic therapy), and positive IgG titers alone represent previous exposure (4). If only IgM bands are detected on Western blot, especially long after exposure, the results are often false positive. Polymerase chain reaction (PCR) testing of CSF or synovial fluid is often positive when those sites are involved.
Consequently, diagnosis of Lyme disease depends on both test results and the presence of typical findings. A classic erythema migrans rash strongly suggests Lyme disease, particularly when supported by other elements (eg, recent tick bite, exposure to endemic area, typical systemic symptoms).
In areas where Lyme disease is endemic, many patients report arthralgias, fatigue, difficulty concentrating, or other nonspecific symptoms. Few patients who have these symptoms but have had no history of erythema migrans or other symptoms of early-localized or early-disseminated Lyme disease actually have Lyme disease. In such patients, elevated IgG titers (with normal IgM titers) indicate past exposure, not current or persistent infection, and may, if misinterpreted, lead to long and unnecessary courses of antibiotic therapy. There is no evidence linking B. burgdorferi infection to this fibromyalgia-like or chronic fatigue–like syndrome.
Differential diagnosis
In the absence of rash, diagnosis is more difficult.
Early-disseminated disease may mimic juvenile idiopathic arthritis in children and reactive arthritis and atypical rheumatoid arthritis in adults. Findings that are often present in rheumatoid arthritis but not Lyme disease include morning stiffness, subcutaneous nodules, iridocyclitis, mucosal lesions, rheumatoid factor, and antinuclear antibodies. Late-stage Lyme disease lacks axial involvement, which distinguishes it from spondyloarthropathies with peripheral joint involvement.
In the United States, human granulocytic anaplasmosis (a rickettsial infection) and babesiosis as well as Borrelia miyamotoi relapsing fever and Powassan virus encephalitis are also transmitted by I. scapularis and have a common geographic distribution in the northeastern and upper Midwest. Patients ill with any one of the diseases transmitted by I. scapularis may be concurrently infected with the other diseases it transmits. A clinician should suspect that patients with Lyme disease also have
Babesiosis (if they have hemolytic anemia and thrombocytopenia)
Human granulocytic anaplasmosis (if they have elevated aminotransferase levels, leukopenia, inclusion bodies in neutrophils, and/or thrombocytopenia)
Acute rheumatic fever is considered in the occasional patient with migratory polyarthralgias and either an increased PR interval or chorea (as a manifestation of meningoencephalitis). However, patients with Lyme disease rarely have heart murmurs or evidence of a preceding streptococcal infection.
Human monocytotropic ehrlichiosis, which is caused by Ehrlichia chaffeensis and transmitted by Amblyomma americanum (the Lone Star tick), occurs mainly in the southeastern and south central United States and is unlikely to be confused with Lyme disease.
In southern and mid-Atlantic states, bites from the A. americanum tick may result in an erythema migrans–like rash accompanied by nonspecific self-limited systemic symptoms and signs. No specific infectious agent has yet been identified as the cause of this disorder (called southern tick-associated rash illness [STARI]).
Lyme disease may cause Bell palsy and, in summer, can manifest with a musculoskeletal aseptic meningitis syndrome that mimics other causes of lymphocytic meningitis or that mimics peripheral neuropathies.
Diagnosis references
1. Sanchez E, Vannier E, Wormser GP, et al: Diagnosis, treatment, and prevention of Lyme disease, human granulocytic anaplasmosis, and babesiosis: A review. JAMA 315 (16):1767–1777, 2016. doi: 10:1001/jama.2016.2284
2. Bush LM, Vazquez-Pertejo MT: Tick borne illness—Lyme disease. Dis Mon 64(5):195–212, 2018. doi: 10.1016/j.disamonth.2018.01.007
3. Lantos PM, Rumbaugh J, Bockenstedt LK, et al: Clinical Practice Guidelines by the Infectious Diseases Society of America (IDSA), American Academy of Neurology (AAN), and American College of Rheumatology (ACR): 2020 Guidelines for the Prevention, Diagnosis and Treatment of Lyme Disease. Clin Infect Dis 72(1):e1–e48, 2021. doi:10.1093/cid/ciaa1215
4. Branda JA, Steere AC: Laboratory diagnosis of Lyme borreliosis. Clin Microbiol Rev 34(2):34:e00018–19. doi: 101128/CMR.00018-19
Treatment of Lyme Disease
Multiple alternatives that vary with stage of disease but typically include amoxicillin, doxycycline, and ceftriaxoneMultiple alternatives that vary with stage of disease but typically include amoxicillin, doxycycline, and ceftriaxone
Most features of Lyme disease respond to antibiotics, but treatment of early disease is most successful. In late-stage disease, antibiotics eradicate the bacteria, relieving the arthritis in most people. However, a few genetically predisposed people have persistent arthritis even after the infection has been eliminated because of continued inflammation. The table Guidelines for Antibiotic Treatment of Lyme Disease in Adults shows antibiotics used in adults for various manifestations of Lyme disease. Treatment in children is similar except that doxycycline is avoided in children shows antibiotics used in adults for various manifestations of Lyme disease. Treatment in children is similar except that doxycycline is avoided in children< 8 years of age.
For symptomatic relief, nonsteroidal anti-inflammatory drugs (NSAIDs) may be used.
Complete heart block may require a temporary pacemaker.
Tense knee joints due to effusions require aspiration. Some genetically predisposed patients with arthritis of the knee that persists despite antibiotic therapy may respond to arthroscopic synovectomy.
Guidelines for Antibiotic Treatment of Lyme Disease in Adults*
Medication | Dosage |
|---|---|
Early Lyme disease† | |
AmoxicillinAmoxicillin | 500 mg orally 3 times a day for 14 days |
DoxycyclineDoxycycline | 100 mg orally twice a day for 10 days |
Cefuroxime axetilCefuroxime axetil | 500 mg orally twice a day for 14 days |
Azithromycin (for patients unable to take doxycycline or beta-lactam antibiotics)Azithromycin (for patients unable to take doxycycline or beta-lactam antibiotics) | 500 mg orally once a day for 7 days |
Neurologic manifestations | |
Bell palsy (no other neurologic abnormalities): | |
DoxycyclineDoxycycline | 100 mg orally twice a day for 14–21 days |
Meningitis (with or without radiculoneuropathy or encephalitis)‡: | |
CeftriaxoneCeftriaxone | 2 g IV once a day for 14–21 days |
CefotaximeCefotaxime | 2 g IV every 8 hours for 14–21 days |
Penicillin GPenicillin G | 3–4 million units IV every 4 hours for 14–21 days |
Doxycycline (for early neurologic disease)Doxycycline (for early neurologic disease) | 100–200 mg orally twice a day for 14–21 days |
Cardiac manifestations | |
CeftriaxoneCeftriaxone | 2 g IV once a day for 14–21 days |
Penicillin GPenicillin G | 3–4 million units IV every 4 hours for 14–21 days |
Doxycycline§Doxycycline§ | 100 mg orally twice a day for 14–21 days§ |
Amoxicillin§Amoxicillin§ | 500 mg orally 3 times a day for 14–21 days§ |
Cefuroxime§Cefuroxime§ | 500 mg orally 2 times a day for 14–21 days§ |
Arthritis (no neurologic involvement)║ | |
AmoxicillinAmoxicillin | 500 mg orally 3 times a day for 28 days |
DoxycyclineDoxycycline | 100 mg orally twice a day for 28 days |
Cefuroxime axetilCefuroxime axetil | 500 mg orally twice a day for 28 days |
CeftriaxoneCeftriaxone | 2 g IV once a day for 14–28 days |
Acrodermatitis chronica atrophicans | |
AmoxicillinAmoxicillin | 500 mg orally 3 times a day for 21–28 days |
DoxycyclineDoxycycline | 100 mg orally twice a day for 21–28 days |
CefuroximeCefuroxime | 500 mg orally 2 times a day for 21–28 days |
* Pregnant women may receive amoxicillin 500 mg 3 times a day for 14 days. No treatment is necessary for pregnant patients who are seropositive but asymptomatic.* Pregnant women may receive amoxicillin 500 mg 3 times a day for 14 days. No treatment is necessary for pregnant patients who are seropositive but asymptomatic. | |
† Without neurologic, cardiac, or joint involvement. For early Lyme disease limited to a single erythema migrans lesion, 10 days is sufficient. | |
‡ Optimal duration of therapy has not been established. There are no controlled trials of therapy > 4 weeks for any neurologic manifestation of Lyme disease. | |
§ For mild carditis with first-degree heart block in which PR interval is < 300 milliseconds, and ventricular function is normal. | |
║ Treatment begins with an oral regimen, which is repeated if response is inadequate. If there was no response or symptoms worsen, parenteral ceftriaxone is given.║ Treatment begins with an oral regimen, which is repeated if response is inadequate. If there was no response or symptoms worsen, parenteral ceftriaxone is given. | |
Adapted from Lantos PM, Rumbaugh J, Bockenstedt LK, et al: Clinical practice guidelines by the Infectious Diseases Society of America (IDSA), American Academy of Neurology (AAN), and American College of Rheumatology (ACR): 2020 Guidelines for the prevention, diagnosis and treatment of Lyme disease. Clin Infect Dis 72(1):e1–e48, 2021. doi: 10.1093/cid/ciaa1215 | |
Prevention of Lyme Disease
Precautions against tick bites (see sidebar Tick Bite Prevention) should be taken by people in endemic areas (1). Deer tick nymphs, which attack humans, are small and difficult to see. Once attached to the skin, they gorge on blood for days. Transmission of B. burgdorferi does not usually occur until the infected tick has been in place for > 36 hours. Thus, searching for ticks after potential exposure and removing them promptly can help prevent infection.
Tick Bite Prevention
Preventing tick access to skin includes
DEET should be used cautiously in very young children because toxic reactions have been reported. Permethrin on clothing effectively kills ticks. Frequent searches for ticks, particularly in hairy areas and on children, are essential in endemic areas.DEET should be used cautiously in very young children because toxic reactions have been reported. Permethrin on clothing effectively kills ticks. Frequent searches for ticks, particularly in hairy areas and on children, are essential in endemic areas. Engorged ticks should be removed with care and not crushed between the fingers because crushing the tick may result in disease transmission. The tick’s body should not be grasped or squeezed. Gradual traction on the head with a small forceps dislodges the tick. The point of attachment should be swabbed with alcohol. Petroleum jelly, alcohol, lit matches, and other irritants are not effective ways to remove ticks and should not be used. (See How to Remove a Tick.) No practical means are available to rid entire areas of ticks, but tick populations may be reduced in endemic areas by controlling small-animal populations. |
Although a single dose of oral doxycycline 200 mg has been shown to reduce the likelihood of Lyme disease after a deer tick bite, routine antibiotic prophylaxis to prevent Lyme disease after a recognized tick bite is not recommended. Patients with a known tick bite can easily be instructed to monitor the bite site and seek care if rash or other symptoms occur; the diagnostic dilemma of Lyme is most prominent when there is no history of tick bite. According to the 2020 Infectious Diseases Society of America (IDSA) guidelines, antibiotic prophylaxis should be offered only when all the following circumstances exist (Although a single dose of oral doxycycline 200 mg has been shown to reduce the likelihood of Lyme disease after a deer tick bite, routine antibiotic prophylaxis to prevent Lyme disease after a recognized tick bite is not recommended. Patients with a known tick bite can easily be instructed to monitor the bite site and seek care if rash or other symptoms occur; the diagnostic dilemma of Lyme is most prominent when there is no history of tick bite. According to the 2020 Infectious Diseases Society of America (IDSA) guidelines, antibiotic prophylaxis should be offered only when all the following circumstances exist (1, 2):
The attached tick can be reliably identified as an adult or nymphal I. scapularis tick.
The tick is estimated to have been attached ≥ 36 hours (based on degree of engorgement of the tick with blood or time of exposure).
Prophylaxis can be started within 72 hours of tick removal. (See How to Remove a Tick.)
Patients live in or have visited an area where ≥ 20% of these ticks are infected with B. burgdorferi (generally only in parts of New England, parts of the mid-Atlantic states, and parts of Minnesota and Wisconsin).
Doxycycline is not contraindicated; it is contraindicated only in pregnant or lactating women, children < 8 years of age, and people who have had an allergic reaction to a tetracycline antibiotic.Doxycycline is not contraindicated; it is contraindicated only in pregnant or lactating women, children tetracycline antibiotic.
Prevention references
1. Lantos PM, Rumbaugh J, Bockenstedt LK, et al: Clinical practice guidelines by the Infectious Diseases Society of America (IDSA), American Academy of Neurology (AAN), and American College of Rheumatology (ACR): 2020 Guidelines for the prevention, diagnosis and treatment of Lyme disease. Clin Infect Dis 72(1):e1–e48, 2021. doi: 10.1093/cid/ciaa1215
2. Nguyen CT, Cifu AS, Pitrak D: Prevention and Treatment of Lyme Disease. JAMA 327(8):772–773, 2022. doi: 10.1001/jama.2021.25302.
Key Points
In the United States, > 90% of Lyme disease cases occur from Maine to Virginia and in Wisconsin, Minnesota, and Michigan; Ixodes scapularis (the deer tick) is the primary vector in these areas.
In the United States, the white-footed mouse is the primary animal reservoir for Borrelia burgdorferi and the preferred host for nymphal and larval forms of the deer tick; deer are hosts for adult ticks but do not carry Borrelia.
Lyme disease has 3 stages: early localized, early disseminated, and late.
Erythema migrans is the first and best clinical indicator; it occurs in ≥ 75% of patients.
In endemic areas, few patients who have arthralgias, fatigue, difficulty concentrating, or other nonspecific symptoms but who have had no history of erythema migrans or other symptoms of early-localized or early-disseminated Lyme disease actually have Lyme disease.
Diagnose clinically if typical rash is present; otherwise, do acute and convalescent serologic testing (C6 ELISA confirmed by enzyme immunoassay or Western blot).
Treat with oral or parenteral antibiotics, depending on disease manifestations.







