


Ehrlichiosis and anaplasmosis are caused by rickettsial-like bacteria. Ehrlichiosis is caused mainly by Ehrlichia chaffeensis; anaplasmosis is caused by Anaplasma phagocytophilum. Both are transmitted to humans by ticks. Symptoms resemble those of Rocky Mountain spotted fever except that a rash is much less common. Onset of illness, with fever, chills, headache, and malaise, is abrupt.
Topic Resources

(See also Overview of Rickettsial and Related Infections.)
Ehrlichiosis and anaplasmosis are related to rickettsial diseases.
E. chaffeensis causes human monocytic ehrlichiosis. Most cases of monocytic ehrlichiosis have been identified in the southeastern and south central United States, where its arthropod vector (the lone star tick) is endemic. (See Centers for Disease Control and Prevention: Ehrlichiosis–epidemiology and statistics.)
Anaplasma phagocytophilum (formerly E. phagocytophila) causes human granulocytic anaplasmosis, which occurs in the Northeast, mid-Atlantic, upper Midwest and West Coast of the United States, where its arthropod vector (ixodid ticks) is endemic. Lyme disease, babesiosis, and Powassan virus have the same tick vector and endemic area, and occasionally patients acquire coinfections after being bitten by a tick infected with more than one type of organism. Several cases of anaplasmosis have been reported after blood transfusions from asymptomatic or acutely infected donors. (See Centers for Disease Control and Prevention: Anaplasmosis–epidemiology and statistics.)
Pearls & Pitfalls
|
The difference in the primary target cell (monocytes for ehrlichiosis and granulocytes for anaplasmosis) results in only minor differences in clinical manifestations.


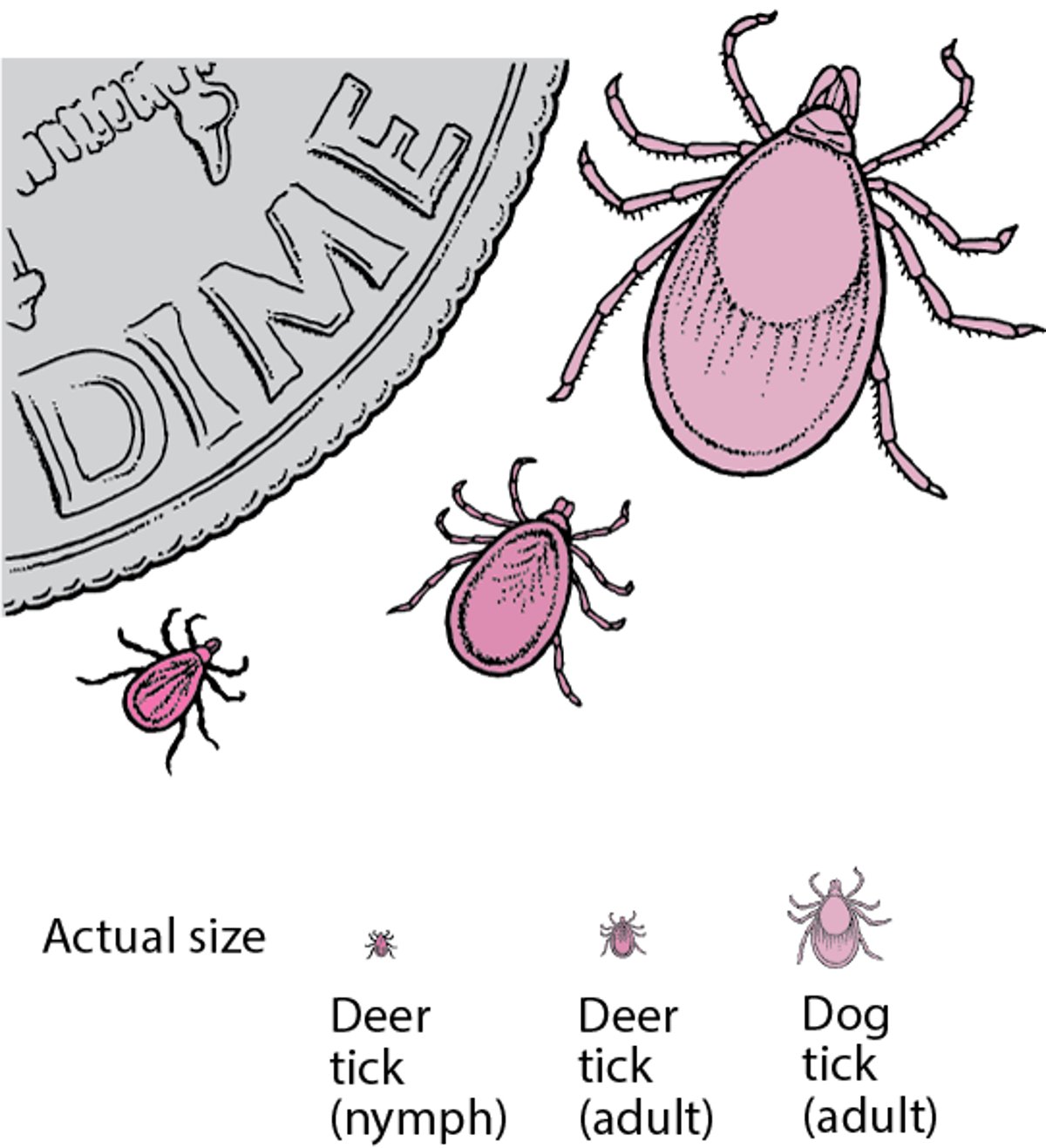
Image courtesy of James Gathany via the Public Health Image Library of the Centers for Disease Control and Prevention.
Symptoms and Signs of Ehrlichiosis and Anaplasmosis
Clinical features of ehrlichiosis and anaplasmosis are similar. Although some infections are asymptomatic, most cause abrupt onset of an influenza-like illness with nonspecific symptoms such as fever, chills, myalgias, weakness, nausea, vomiting, cough, headache, and malaise, usually beginning about 12 days after the tick bite.
Rash is uncommon in anaplasmosis. Some patients infected with E. chaffeensis develop a maculopapular or petechial rash on the trunk and extremities.
Ehrlichiosis and anaplasmosis may result in disseminated intravascular coagulation, multiorgan failure, seizures, and coma.
Both infections appear to be more severe and have a higher mortality rate in patients with compromised immunity caused by immunosuppressants (eg, corticosteroids, cancer chemotherapy, long-term treatment with immunosuppressants after organ transplantation), HIV infection, or splenectomy.
Diagnosis of Ehrlichiosis and Anaplasmosis
Polymerase chain reaction (PCR) testing of a blood sample
Diagnostic serologic tests are available for ehrlichiosis and anaplasmosis, but PCR of blood is more sensitive and specific and can result in an earlier diagnosis because serologic tests require comparison of serial titers. Cytoplasmic inclusions in monocytes (ehrlichiosis) or in neutrophils (anaplasmosis) may be detected, but cytoplasmic inclusions are more commonly seen in anaplasmosis.
Blood and liver tests may detect hematologic and hepatic abnormalities, such as leukopenia, thrombocytopenia, and elevated aminotransferase levels.
Treatment of Ehrlichiosis and Anaplasmosis
DoxycyclineDoxycycline
Treatment of ehrlichiosis and anaplasmosis is best started before laboratory results return. When treatment is started early, patients generally respond rapidly and well. A delay in treatment may lead to serious complications, including viral and fungal superinfections and death in 2 to 5%.
Primary treatment is doxycycline until the patient improves and has been afebrile for 24 to 48 hours but is continued for at least 7 days. For patients who do not tolerate doxycycline, desensitization is recommended. Primary treatment is doxycycline until the patient improves and has been afebrile for 24 to 48 hours but is continued for at least 7 days. For patients who do not tolerate doxycycline, desensitization is recommended.
Although some tetracyclines can cause tooth staining in children < 8 years of age, the Centers for Disease Control and Prevention (CDC) advise that a course of doxycycline is warranted (Although some tetracyclines can cause tooth staining in children doxycycline is warranted (1). Research indicates that short courses of doxycycline (5 to 10 days, as used for rickettsial disease) can be used in children without causing tooth staining or weakening of tooth enamel (). Research indicates that short courses of doxycycline (5 to 10 days, as used for rickettsial disease) can be used in children without causing tooth staining or weakening of tooth enamel (2; see also CDC: Research on doxycycline and tooth staining).
Chloramphenicol is not effective.Chloramphenicol is not effective.
Some patients continue to experience headache, weakness, and malaise for weeks after adequate treatment.
Treatment references
1. Centers for Disease Control and Prevention: Ehrlichiosis
2. Todd SR, Dahlgren FS, Traeger MS, et al: No visible dental staining in children treated with doxycycline for suspected Rocky Mountain Spotted Fever. : No visible dental staining in children treated with doxycycline for suspected Rocky Mountain Spotted Fever.J Pediatr 166(5):1246-51, 2015. doi: 10.1016/j.jpeds.2015.02.015
Prevention of Ehrlichiosis and Anaplasmosis
No vaccine is available to prevent ehrlichiosis or anaplasmosis. Measures can be taken to prevent tick bites. (See also Centers for Disease Control and Prevention: Preventing tick bites.)
Deer Ticks

Preventing tick access to skin includes
Staying on paths and trails
Tucking trousers into boots or socks
Wearing long-sleeved shirts
Applying repellents with diethyltoluamide (DEET) to skin surfacesApplying repellents with diethyltoluamide (DEET) to skin surfaces
DEET should be used cautiously in very young children because toxic reactions have been reported. Permethrin on clothing effectively kills ticks. Frequent searches for ticks, particularly in hairy areas and on children, are essential in endemic areas.DEET should be used cautiously in very young children because toxic reactions have been reported. Permethrin on clothing effectively kills ticks. Frequent searches for ticks, particularly in hairy areas and on children, are essential in endemic areas.
Engorged ticks should be removed with care and not crushed between the fingers because crushing the tick may result in disease transmission. The tick’s body should not be grasped or squeezed. Gradual traction on the head with a small forceps dislodges the tick. The point of attachment should be swabbed with alcohol. Petroleum jelly, lit matches, and other irritants are not effective ways to remove ticks and should not be used.
No practical means are available to rid entire areas of ticks, but tick populations may be reduced in endemic areas by controlling small-animal populations.
Key Points
Ehrlichiosis and anaplasmosis are tick-borne infections related to rickettsial diseases.
Clinical features of ehrlichiosis and anaplasmosis are similar, usually with abrupt onset of an influenza-like illness; rash is uncommon in anaplasmosis.
Ehrlichiosis and anaplasmosis may result in disseminated intravascular coagulation, multiorgan failure, seizures, and coma.
Do PCR testing of blood, which is more sensitive and specific than serologic tests and can result in an early diagnosis.
Treat with doxycycline, best started before laboratory results return.Treat with doxycycline, best started before laboratory results return.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
Centers for Disease Control and Prevention: Information about preventing tick bites
Centers for Disease Control and Prevention: Information and statistics regarding the epidemiology of ehrlichiosis and anaplasmosis







