



Bejel, pinta, and yaws (endemic treponematoses) are chronic, tropical spirochetal infections spread by body contact. Symptoms of bejel are mucous membrane and cutaneous lesions, followed by bone and skin gummas. Yaws causes periostitis and dermal lesions. Pinta lesions are confined to the dermis. Diagnosis is clinical and epidemiologic. Treatment is with azithromycin.
Topic Resources



Spirochetes are distinguished by the helical shape of the bacteria. Pathogenic spirochetes include Treponema, Leptospira, and Borrelia. Both Treponema and Leptospira are too thin to be seen using brightfield microscopy but are clearly seen using darkfield or phase microscopy. Borrelia are thicker and can also be stained and seen using brightfield microscopy.
The causative agents of bejel, pinta, and yaws are
Bejel: Treponema pallidum subspecies endemicum
Yaws: T. pallidum subspecies pertenue
Pinta: Treponema carateum
The Treponema species causing bejel and yaws are morphologically and serologically indistinguishable from the agent of syphilis, T. pallidum subspecies pallidum. As in syphilis, the typical course is an initial mucocutaneous lesion followed by diffuse secondary lesions, a latent period, and late destructive disease.
Transmission of bejel, yaws, and pinta is by close skin contact primarily between children living in conditions of poor hygiene.
Bejel (endemic syphilis) occurs mainly in hot, dry regions of the eastern Mediterranean and Saharan West Africa. Transmission also results from mouth-to-mouth contact or sharing eating and drinking utensils.
Yaws (frambesia) is the most prevalent of the endemic treponematoses and occurs in humid equatorial countries. Transmission requires direct skin contact and is favored by skin trauma.
Pinta, which is more limited in geographical distribution, occurs among the natives of Mexico, Central America, and South America and is not very contagious. Transmission probably requires contact with broken skin.
Unlike T. pallidum subspecies pallidum, other treponemal subspecies that infect humans are not transmitted via blood or transplacentally.
Symptoms and Signs of Bejel, Pinta, and Yaws
Bejel begins in childhood as a mucous patch (usually on the buccal mucosa), which may go unnoticed, or as stomatitis at the angles of the lips. These painless lesions may resolve spontaneously but are usually followed by papulosquamous and erosive papular lesions of the trunk and extremities that are similar to yaws. Periostitis of the leg bones is common. Later, gummatous lesions of the nose and soft palate develop.
Yaws, after an incubation period of several weeks, begins at the site of inoculation as a yellow-to-red papule that enlarges, erodes, and ulcerates (primary yaws). The surface resembles a strawberry, and the exudate is rich in spirochetes. Local lymph nodes may be enlarged and tender. The lesion heals but is followed after months to a year by successive generalized eruptions that resemble the primary lesion (secondary yaws). These lesions often develop in moist areas of the axillae, skinfolds, and mucosal surfaces; they heal slowly and may recur. Keratotic lesions may develop on the palms and soles, causing painful ulcerations (crab yaws). Five to 10 years later, destructive lesions (tertiary yaws) may develop; they include the following:
Periostitis (particularly of the tibia)
Proliferative exostoses of the nasal portion of the maxillary bone (goundou)
Juxta-articular nodules
Gummatous skin lesions
Ultimately, mutilating facial ulcers, particularly around the nose (gangosa)

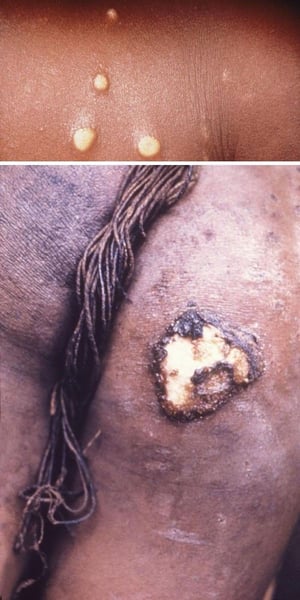
Primary yaws manifests as a large papule or papillomata at the site of inoculation. Papules are highly infectious (top). This image shows the buttocks of a girl with primary yaws. Primary yaws lesions may also develop a crusted surface (bottom).
Top image courtesy of Dr. Peter Perine via the Public Health Image Library of the Centers for Disease Control and Prevention. Bottom image courtesy of K McLennon, Tulane University Medical School, via the Public Health Image Library of the Centers for Disease Control and Prevention.


After the lesion of primary yaws heals, a generalized eruption of soft granulomata on the face, extremities (top), or buttocks occurs. Another feature of secondary yaws is soft, keratotic, tumor-like masses that develop on the soles of the feet (bottom). The masses force patients to walk on the sides of their feet, giving rise to the nickname crab yaws.
Top image courtesy of Dr. Peter Perine via the Public Health Image Library of the Centers for Disease Control and Prevention. Bottom image courtesy of Dr. Susan Lindsley via the Public Health Image Library of the Centers for Disease Control and Prevention.


About 10% of untreated patients develop tertiary yaws, which causes disfiguring bone and soft-tissue lesions.
Image courtesy of Dr. Peter Perine via the Public Health Image Library of the Centers for Disease Control and Prevention.
Primary yaws manifests as a large papule or papillomata at the site of inoculation. Papules are highly infectious (top). This image shows the buttocks of a girl with primary yaws. Primary yaws lesions may also develop a crusted surface (bottom).
Top image courtesy of Dr. Peter Perine via the Public Health Image Library of the Centers for Disease Control and Prevention. Bottom image courtesy of K McLennon, Tulane University Medical School, via the Public Health Image Library of the Centers for Disease Control and Prevention.
After the lesion of primary yaws heals, a generalized eruption of soft granulomata on the face, extremities (top), or buttocks occurs. Another feature of secondary yaws is soft, keratotic, tumor-like masses that develop on the soles of the feet (bottom). The masses force patients to walk on the sides of their feet, giving rise to the nickname crab yaws.
Top image courtesy of Dr. Peter Perine via the Public Health Image Library of the Centers for Disease Control and Prevention. Bottom image courtesy of Dr. Susan Lindsley via the Public Health Image Library of the Centers for Disease Control and Prevention.
About 10% of untreated patients develop tertiary yaws, which causes disfiguring bone and soft-tissue lesions.
Image courtesy of Dr. Peter Perine via the Public Health Image Library of the Centers for Disease Control and Prevention.
Pinta lesions are confined to the dermis. They begin at the inoculation site as a small papule that enlarges and becomes hyperkeratotic; they develop mainly on the extremities, face, and neck. After 3 to 9 months, further thickened and flat lesions (pintids) appear all over the body and over bony prominences. Still later, some lesions become slate blue or depigmented, resembling vitiligo. Pinta lesions typically persist if not treated.
Diagnosis of Bejel, Pinta, and Yaws
History and physical examination
Serological and polymerase chain reaction (PCR) testing
Diagnosis of endemic treponematoses is based on the typical appearance of lesions in people from endemic areas.
There are no specific serologic assays available to diagnose endemic treponematosis.
Both nontreponemal and treponemal serologic tests for syphilis (the Venereal Disease Research Laboratory [VDRL], rapid plasma reagin [RPR], and fluorescent treponemal antibody absorption tests [FTA-ABS]) are positive; thus, differentiation from sexually transmitted syphilis is clinical. Early lesions are often darkfield-positive for spirochetes and are indistinguishable from T. pallidum subspecies pallidum.
Point-of-care (POC) tests have been developed for rapid real-time diagnosis of endemic treponematoses and syphilis. These assays detect IgM and IgG antibodies to T. pallidum and non-treponemal antigens and can be performed on whole blood, plasma, or serum.
Polymerase chain reaction (PCR) tests can detect nonvenereal T. pallidum subspecies but have limited availability and may not be obtainable in resource-limited areas.
Radiographic imaging modalities are not useful for diagnosing endemic treponematoses but may demonstrate periosteal bone abnormalities in late-stage cases of bejel and yaws.
Treatment of Bejel, Pinta, and Yaws
Azithromycin
Penicillin G benzathine
Penicillin G benzathine has been the preferred medication for the treatment of the endemic treponematoses. It is given as 1.2 million units IM for patients 10 years of age and older and 600,000 units IM for children younger than 10 years of age (Penicillin G benzathine has been the preferred medication for the treatment of the endemic treponematoses. It is given as 1.2 million units IM for patients 10 years of age and older and 600,000 units IM for children younger than 10 years of age (1, 2).
The World Health Organization (WHO) recommends treating with a single dose of azithromycin 30 mg/kg (maximum 2 g). Azithromycin has demonstrated equivalent efficacy as penicillin G benzathine (The World Health Organization (WHO) recommends treating with a single dose of azithromycin 30 mg/kg (maximum 2 g). Azithromycin has demonstrated equivalent efficacy as penicillin G benzathine (3, 4).
Doxycycline 100 mg orally twice daily for 14 days is an accepted alternative for patients who are allergic to or intolerant of azithromycin and penicillin.Doxycycline 100 mg orally twice daily for 14 days is an accepted alternative for patients who are allergic to or intolerant of azithromycin and penicillin.
Response to treatment is assessed by observing resolution of early stage lesions or non-progression of late lesions. Serologic response to therapy is determined by decline in RPR or VDRL titers with a 4-fold decrease in titer by one-year in most treated patients, however, these titers may not become negative.
For patients with late manifestations of bejel, a second dose of penicillin administered one week after the first is recommended.
All contacts of patients, whether or not they have symptoms, should receive the same treatment as patients. All patients with latent disease (individuals who have no symptoms but with positive serologic test for syphilis) in endemic zones should also be treated the same way.
Patients should undergo repeat nontreponemal testing at 6 and 12 months after treatment; in most cases, titers decline 4-fold within less than 1 year.
Treatment references
1. Giacani L, Lukehart SA: The endemic treponematoses. Clin Microbiol Rev 27(1):89–115, 2014. doi: 10.1128/CMR.00070-13
2. Marks M, Solomon AW, Mabey DC: Endemic treponemal diseases [published correction appears in Trans R Soc Trop Med Hyg. 2015 Sep;109(9):604. doi: 10.1093/trstmh/trv052]. Trans R Soc Trop Med Hyg 108(10):601–607, 2014, https://doi.org/10.1093/trstmh/tru128
3. Mitjà O, Hays R, Ipai A, et al: Single-dose azithromycin versus benzathine benzylpenicillin for treatment of yaws in children in Papua New Guinea: an open-label, non-inferiority, randomised trial. Lancet 379(9813):342–347, 2012. doi:10.1016/S0140-6736(11)61624-3
4. Mitjà O, Houinei W, Moses P, et al: Mass treatment with single-dose azithromycin for yaws. N Engl J Med 372(8):703–710, 2015. doi:10.1056/NEJMoa1408586
Key Points
The Treponema species that cause bejel, pinta, and yaws are morphologically and serologically indistinguishable from the agent of syphilis, T. pallidum subspecies pallidum.
Disease is spread by close body contact, typically between children living in conditions of poor hygiene.
As in syphilis, the typical course is an initial mucocutaneous lesion, followed by diffuse secondary lesions, a latent period, and late destructive disease.
Serologic tests for syphilis (including fluorescent treponemal antibody absorption tests) are positive; thus, differentiation from venereal syphilis is clinical.
Give one dose of azithromycin or one dose of penicillin G benzathine or in those allergic to or intolerant of azithromycin and penicillin, give 2 weeks of doxycycline.Give one dose of azithromycin or one dose of penicillin G benzathine or in those allergic to or intolerant of azithromycin and penicillin, give 2 weeks of doxycycline.
Treat close contacts with antibiotics.







