



Preseptal cellulitis (periorbital cellulitis) is infection of the eyelid and surrounding skin anterior to the orbital septum. Orbital cellulitis is infection of the orbital tissues posterior to the orbital septum. Either can be caused by an external focus of infection (eg, a wound), infection that extends from the nasal sinuses or teeth, or metastatic spread from infection elsewhere. Symptoms include eyelid pain, discoloration, and swelling; orbital cellulitis also causes fever, malaise, proptosis, impaired ocular movement, and impaired vision. Diagnosis is based on history, examination, and CT or MRI. Treatment is with antibiotics and sometimes surgical drainage.




Preseptal cellulitis and orbital cellulitis are distinct diseases that share a few clinical symptoms and signs. Preseptal cellulitis usually begins superficial to the orbital septum, the membranous sheet that extends from the orbital rim into the upper and lower eyelid. Orbital cellulitis usually begins deep to the orbital septum. Both are more common among children; preseptal cellulitis is far more common than orbital cellulitis.
Etiology of Preseptal and Orbital Cellulitis
Preseptal cellulitis is usually caused by contiguous spread of infection from local facial or eyelid injuries, insect or animal bites, chalazion or hordeolum, or sinusitis.
Orbital cellulitis is most often caused by extension of infection from adjacent sinuses, especially the ethmoid sinus. Less commonly, orbital cellulitis is caused by direct infection accompanying local trauma (eg, insect or animal bite, penetrating eyelid injuries), contiguous spread of infection from the face or teeth, or by hematogenous spread.
Pathogens vary by etiology and patient age. Streptococcus pneumoniae is a frequent pathogen associated with sinus infection, whereas Staphylococcus aureus (usually methicillin sensitive) and Streptococcus pyogenes predominate when infection arises from local trauma (1). Haemophilus influenzae type b, once a common cause, is now less common because of widespread vaccination. Fungi are uncommon pathogens, causing orbital cellulitis in patients who have diabetes or in those who are immunosuppressed. Infection in children < 9 years is typically with a single aerobic organism; with increasing age, particularly age > 15 years, infection is more typically polymicrobial with mixed aerobic and anaerobic (Bacteroides, Peptostreptococcus) infections (2, 3).
Etiology references
1. Anosike BI, Ganapathy V, Nakamura MM: Epidemiology and management of orbital cellulitis in children. J Pediatric Infect Dis Soc 11(5):214-220, 2020. doi: 10.1093/jpids/piac006
2. Garcia GH, Harris GJ: Criteria for nonsurgical management of subperiosteal abscess of the orbit: analysis of outcomes 1988-1998. Ophthalmology 107(8):1454-1456, 2000; discussion 1457-8. doi: 10.1016/s0161-6420(00)00242-6
3. Liao JC, Harris GJ: Subperiosteal abscess of the orbit: Evolving pathogens and the therapeutic protocol. Ophthalmology 122(3):639-647, 2015. doi: 10.1016/j.ophtha.2014.09.009
Pathophysiology of Preseptal and Orbital Cellulitis
Because orbital cellulitis originates from large adjacent foci of fulminant infection (eg, sinusitis) separated by only a thin bone barrier, orbital infection can be extensive and severe. Subperiosteal fluid collections, some quite large, can accumulate; they are called subperiosteal abscesses, but many are sterile initially.
Preseptal and Orbital Cellulitis

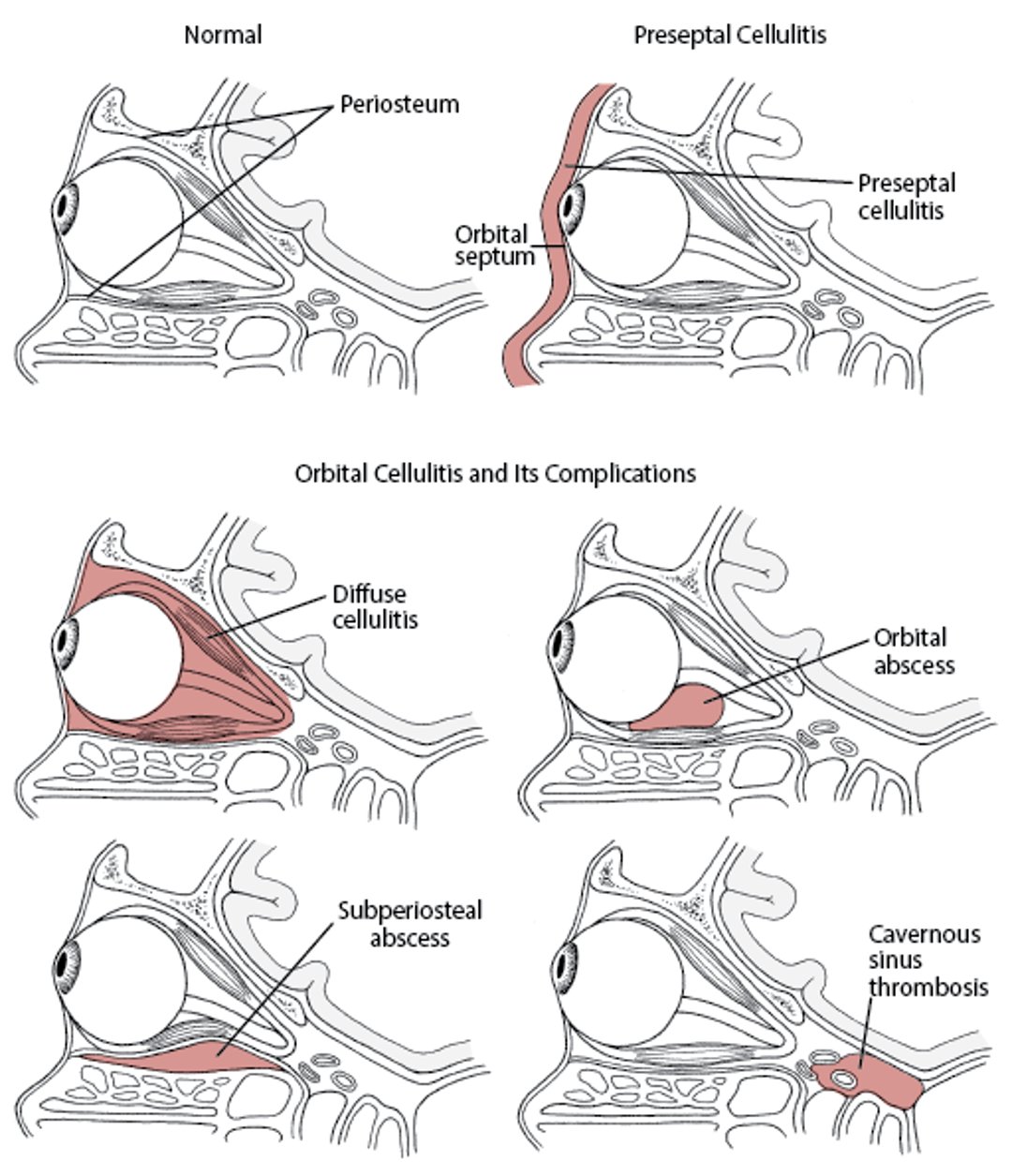
Complications with orbital cellulitis include vision loss due to ischemic retinopathy and optic neuropathy caused by increased intraorbital pressure; restricted ocular movements (ophthalmoplegia) caused by soft-tissue inflammation; and intracranial sequelae from central spread of infection, including cavernous sinus thrombosis, meningitis, and brain abscess.
Symptoms and Signs of Preseptal and Orbital Cellulitis
Symptoms and signs of preseptal cellulitis include tenderness, swelling, warmth, redness or discoloration (violaceous in the case of H. influenzae) of the eyelid, and sometimes fever. Patients may be unable to open their eyes because of eyelid swelling. The swelling and discomfort can make it difficult to examine the eye, but when accomplished, examination shows that visual acuity is not affected, ocular movement is intact, and the globe is not pushed forward (proptosis).


Photo courtesy of James Garrity, MD.
Symptoms and signs of orbital cellulitis include swelling and redness of the eyelid and surrounding soft tissues, conjunctival hyperemia and chemosis, decreased ocular motility, pain with eye movements, decreased visual acuity, and proptosis caused by orbital swelling. Signs of the primary infection are also often present (eg, nasal discharge and bleeding with sinusitis, periodontal pain and swelling with abscess). Fever is usually present. Headache and lethargy should raise suspicion of associated meningitis. Some or all of these findings may be absent early in the course of the infection.


Photos courtesy of James Garrity, MD.

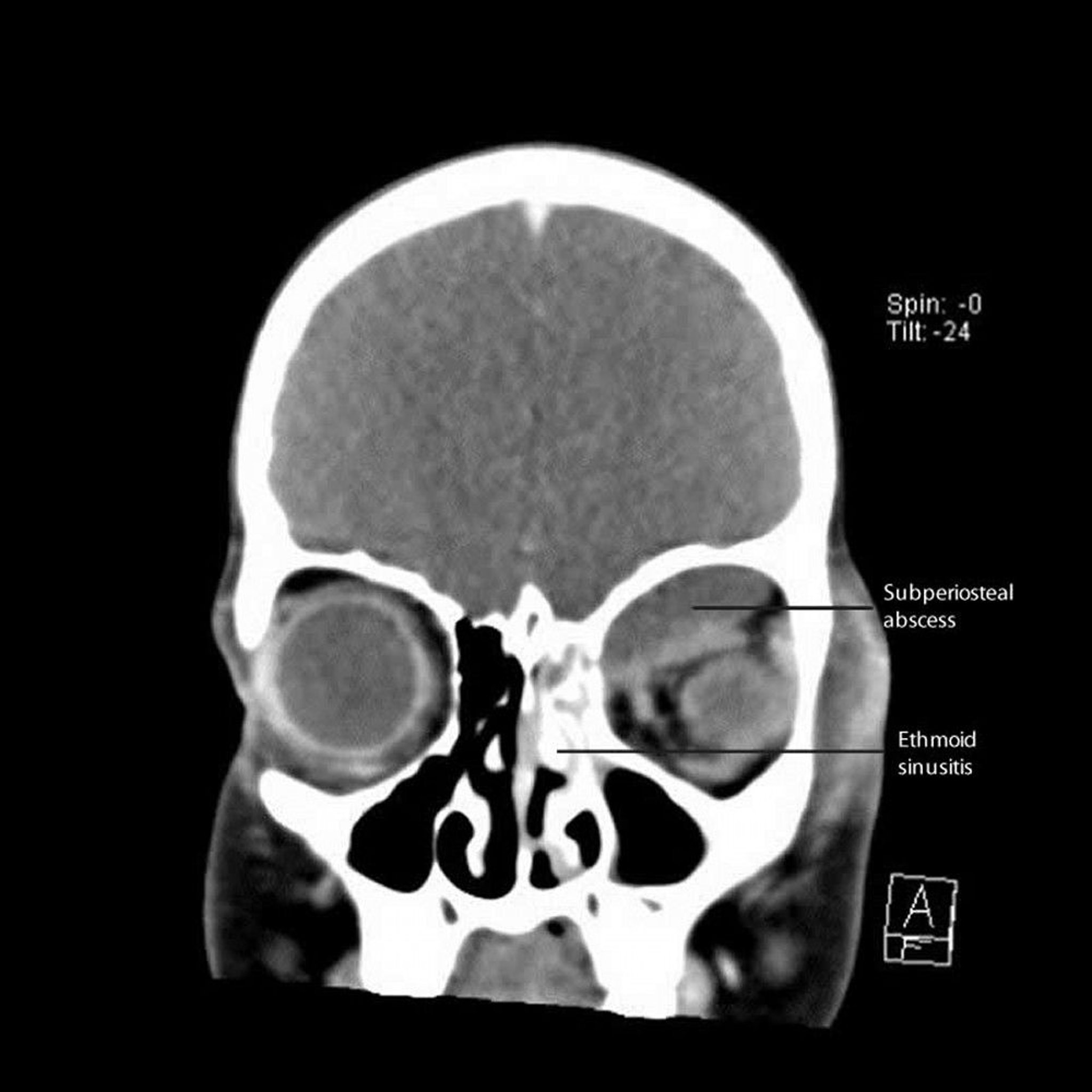
CT courtesy of James Garrity, MD.
Subperiosteal abscesses, if large enough, can contribute to symptoms of orbital cellulitis such as swelling and redness of the eyelid, decreased ocular motility, proptosis, and decreased visual acuity.
Diagnosis of Preseptal and Orbital Cellulitis
Mainly clinical evaluation
CT or MRI if orbital cellulitis is possible
Diagnosis of preseptal cellulitis and orbital cellulitis is primarily clinical. Other disorders to consider include trauma, insect or animal bites without cellulitis, retained foreign bodies, allergic reactions, tumors, and inflammatory orbital pseudotumor.
Eyelid swelling may require the use of lid retractors for evaluation of the globe, and initial signs of complicated infection may be subtle. An ophthalmologist should be consulted when orbital cellulitis is suspected.
Preseptal cellulitis and orbital cellulitis are often distinguishable clinically. Preseptal cellulitis is likely if eye findings are normal except for eyelid swelling. The presence of a local nidus of infection on the skin makes preseptal cellulitis even more likely.
Necrotizing fasciitis (necrotizing soft tissue infection) of the orbit is a severe form of preseptal cellulitis that can rapidly invade surrounding tissues in the fascial planes. Surgical debridement is the mainstay of therapy, plus adjunctive intravenous broad-spectrum antibiotics that cover group A streptococci and other bacteria (1, 2). Prognosis is guarded.
Pearls & Pitfalls
|
If findings are equivocal, if the examination is difficult (as in young children), or if nasal discharge is present (suggesting sinusitis), CT or MRI should be done to exclude orbital cellulitis, tumor, and pseudotumor. MRI is better than CT if cavernous sinus thrombosis is being considered.
The direction of proptosis may be a clue to the site of infection; eg, extension from the frontal sinus pushes the globe down and out, and extension from the ethmoid sinus pushes the globe laterally and out.
Blood cultures are often done (ideally before beginning antibiotics) in patients with orbital cellulitis, but yields are low (3). Lumbar puncture is done if meningitis is suspected. Cultures of the paranasal sinus fluid are done if sinusitis is the suspected source; however, unless done intraoperatively, such cultures are unlikely to affect management (4). Other laboratory tests are not particularly helpful.
Diagnosis references
1. Wladis EJ: Periorbital necrotizing fasciitis. Surv Ophthalmology 67(5):1547-1552. https://doi.org/10.1016/j.survophthal.2022.02.006
2. Tambe K, Tripathi A, Burns J, et al: Multidisciplinary management of periocular necrotising fasciitis: A series of 11 patients. Eye (Lond) 26(3):463-467, 2012. doi: 10.1038/eye.2011.241
3. Mukherjee G, Sufcak K, Hames N, et al: Bugs behind the bulging eyeball: Microbiology and antibiotic management in orbital cellulitis with or without subperiosteal abscess. Clin Pediatr (Phila) 63(2):214-221, 2024. doi: 10.1177/00099228231202158
4. Schein Y, Lin LY, Revere K, et al: Microbial patterns and culture utility in orbital cellulitis. J AAPOS 27(4):200.e1-200.e6, 2023. doi: 10.1016/j.jaapos.2023.05.010
Treatment of Preseptal and Orbital Cellulitis
Antibiotics
Preseptal cellulitis
In patients with preseptal cellulitis, initial therapy should be directed against sinusitis pathogens (S. pneumoniae, nontypeable H. influenzae, S. aureus, Moraxella catarrhalis); however, in areas where methicillin-resistant S. aureus is prevalent, clinicians should add appropriate antibiotics (eg, clindamycin, trimethoprim/sulfamethoxazole, or doxycycline for oral treatment and vancomycin for inpatient treatment). In patients with dirty wounds, gram-negative infection must be considered.is prevalent, clinicians should add appropriate antibiotics (eg, clindamycin, trimethoprim/sulfamethoxazole, or doxycycline for oral treatment and vancomycin for inpatient treatment). In patients with dirty wounds, gram-negative infection must be considered.
Outpatient treatment is an option if orbital cellulitis has been definitively excluded; children should have no signs of systemic infection and should be in the care of responsible parents or guardians. Patients should be closely followed by an ophthalmologist. Outpatient treatment options include amoxicillin/clavulanate 30 mg/kg orally every 8 hours (for children Outpatient treatment is an option if orbital cellulitis has been definitively excluded; children should have no signs of systemic infection and should be in the care of responsible parents or guardians. Patients should be closely followed by an ophthalmologist. Outpatient treatment options include amoxicillin/clavulanate 30 mg/kg orally every 8 hours (for children< 12 years) or 500 mg orally every 8 to 12 hours or 875 mg orally 2 times a day (for adults) for 10 days. (Dose may need to increase if penicillin-resistant S. pneumoniae is suspected.)
For inpatients, ampicillin/sulbactam 50 mg/kg IV every 6 hours (for children) or 1.5 to 3 g (for adults) IV every 6 hours (maximum 8 g ampicillin/day) for 7 days is an option. If methicillin-resistant For inpatients, ampicillin/sulbactam 50 mg/kg IV every 6 hours (for children) or 1.5 to 3 g (for adults) IV every 6 hours (maximum 8 g ampicillin/day) for 7 days is an option. If methicillin-resistantS. aureus is a consideration, antibiotics should be adjusted accordingly.
Orbital cellulitis
Patients with orbital cellulitis should be hospitalized and treated with meningitis-dose antibiotics (see table Common IV Antibiotic Dosages for Acute Bacterial Meningitis). A second- or third-generation cephalosporin, such as cefotaxime 50 mg/kg IV every 6 hours (for children ). A second- or third-generation cephalosporin, such as cefotaxime 50 mg/kg IV every 6 hours (for children< 12 years) or 1 to 2 g IV every 6 hours (for adults) for 14 days, is an option when sinusitis is present; imipenem, ceftriaxone, and piperacillin/tazobactam are other options. 12 years) or 1 to 2 g IV every 6 hours (for adults) for 14 days, is an option when sinusitis is present; imipenem, ceftriaxone, and piperacillin/tazobactam are other options.
If cellulitis is related to trauma or foreign body, treatment should cover gram-positive pathogens, including methicillin-resistant S. aureus if in a prevalent area (vancomycin 1 g IV every 12 hours), and gram-negative pathogens (eg, ertapenem 1g IV once/day), and be taken for 7 to 10 days or until clinical improvement (if in a prevalent area (vancomycin 1 g IV every 12 hours), and gram-negative pathogens (eg, ertapenem 1g IV once/day), and be taken for 7 to 10 days or until clinical improvement (1).
If anaerobic pathogens are suspected (as may be the case with dental infections), metronidazole is typically used. If anaerobic pathogens are suspected (as may be the case with dental infections), metronidazole is typically used.
Surgery to decompress the orbit, drain an abscess, open infected sinuses, or a combination is indicated in any of the following circumstances:
Vision is compromised.
Suppuration or foreign body is suspected.
Imaging shows orbital or large subperiosteal abscess, particularly along the orbital roof.
The infection does not resolve with antibiotics.
Treatment reference
1. Liao JC, Harris GJ: Subperiosteal abscess of the orbit: Evolving pathogens and the therapeutic protocol. Ophthalmology 122(3):639-647, 2015. doi: 10.1016/j.ophtha.2014.09.009
Key Points
Preseptal and orbital cellulitis are differentiated by whether infection is anterior or posterior to the orbital septum.
Orbital cellulitis is usually caused by contiguous spread of ethmoid or frontal sinusitis, whereas preseptal cellulitis is commonly caused by contiguous spread from local facial or eyelid injuries, insect or animal bites, conjunctivitis, and chalazion or hordeolum.
Both disorders can cause tenderness, swelling, warmth, redness or discoloration of the eyelid, and fever.
Orbital cellulitis is likely if there is decreased ocular motility, pain with eye movements, proptosis, or decreased visual acuity.
Antibiotic therapy is indicated, with surgery reserved for complicated orbital cellulitis (eg, abscess, foreign body, impaired vision, antibiotic failure).







