


Gastroesophageal reflux is the backward movement of food and acid from the stomach into the esophagus and sometimes into the mouth.
Reflux may be caused by the infant’s position during feeding; overfeeding; exposure to caffeine, nicotine, and cigarette smoke; a food intolerance or allergy; or an abnormality of the digestive tract.
Infants may vomit, spit up excessively, have feeding or breathing problems, and also appear irritable.
Tests that help doctors diagnose the disorder include a barium study, an esophageal pH probe, a gastric emptying scan, endoscopy, and sometimes ultrasonography.
Treatment options include thickened or hypoallergenic formula for feedings, special positioning, frequent burping, sometimes medications, and, in severe cases, surgery.
(For adults, see Gastroesophageal Reflux Disease (GERD).)
Nearly all infants have episodes of gastroesophageal reflux, which are characterized by spitting up fluid or food, usually soon after eating and sometimes when they are being burped. Reflux typically worsens in the first several months of life, peaks around 6 to 7 months of age, and then gradually lessens. Nearly all infants with reflux outgrow it by about 18 months of age.
Gastroesophageal reflux becomes known as gastroesophageal reflux disease (GERD) when it
Interferes with feeding and growth
Damages the esophagus (esophagitis)
Leads to breathing difficulties (such as coughing, wheezing, or stopping breathing)
Continues beyond infancy into childhood
Causes of Gastroesophageal Reflux
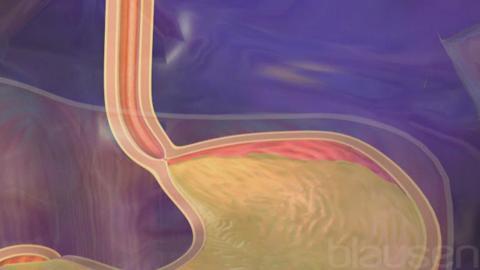
Healthy infants have reflux for many reasons. The circular band of muscle at the junction of the esophagus and stomach (the lower esophageal sphincter) normally keeps stomach contents from entering the esophagus (see Overview of the Esophagus). In infants, this muscle may be underdeveloped, or it may relax at inappropriate times, allowing stomach contents to move backward (reflux) into the esophagus. Being held flat during feeding or lying down after feeding promotes reflux because gravity is no longer able to help keep material in the stomach from flowing back up the esophagus. Overfeeding and chronic lung diseases predispose infants to reflux because they increase pressure in the stomach. Cigarette smoke (as secondhand smoke) and caffeine (in beverages or breast milk) relax the lower esophageal sphincter, allowing reflux to occur more readily. Caffeine and nicotine (in breast milk) also stimulate acid production, so any reflux that does occur is more acidic.
A food allergy, most commonly cow's milk allergy, or food intolerance also can contribute to reflux, but these are less common causes.
Another less common cause of reflux is a slowly emptying stomach (gastroparesis). In gastroparesis, food remains in the stomach for a longer period of time, which causes pressure in the stomach to remain high. High pressure in the stomach leads to reflux.
Inherited disorders of metabolism, such as galactosemia and hereditary fructose intolerance, and anatomic abnormalities, such as narrowing of the esophagus, partial blocking of the stomach (pyloric stenosis), or abnormal positioning of the intestines (malrotation), can initially mimic reflux because they cause repeated episodes of vomiting. However, these abnormalities are more serious and can progress to vomiting and other symptoms of obstruction, such as abdominal pain, listlessness, and dehydration.
Symptoms of Gastroesophageal Reflux
In infants, the most obvious symptoms of gastroesophageal reflux are
Vomiting
Excessive spitting up (regurgitation)
In young children, the most common symptoms are
Chest pain
Abdominal pain
Sometimes heartburn (a burning pain behind the breastbone)
In adolescents, the most common symptom is the same as in adults:
Heartburn
Complications of reflux
In some infants, reflux causes complications and becomes known as GERD. Such complications include
Irritability due to stomach discomfort
Feeding problems that can result in poor growth
“Spells” of twisting and posturing that may be confused with seizures
Less commonly, small amounts of acid from the stomach may enter the windpipe (aspiration). Acid in the windpipe and breathing passages may result in coughing, wheezing, stopping breathing (apnea), or pneumonia. Many children with asthma also have reflux. Ear pain, hoarseness, hiccups, and sinusitis also can occur as a result of GERD. If the esophagus is significantly irritated (esophagitis), there may be some bleeding, resulting in iron deficiency anemia. In others, esophagitis can cause scar tissue, which can narrow the esophagus (stricture).
Diagnosis of Gastroesophageal Reflux
Barium study
Esophageal pH probe or impedance probe
Gastric emptying scan
Upper endoscopy
Ultrasound of the abdomen
Tests are often not needed to diagnose gastroesophageal reflux in infants or older children who simply have mild symptoms such as frequent spit-ups (in infants) and heartburn (in older children). However, if symptoms are more complicated, various tests can be done.
A barium study is the most common test. The child swallows barium, a liquid that outlines the digestive tract when x-rays are taken. Although this test can help the doctor diagnose gastroesophageal reflux, it more importantly helps the doctor identify some of the possible causes of the reflux.
An esophageal pH probe is a thin flexible tube with a sensor at the tip that measures the degree of acidity (pH). Doctors pass the tube through the child’s nose, down the throat, and into the end of the esophagus. The tube is usually left in place for 24 hours. Normally, children do not have acid in their esophagus, so if the sensor detects acid, it is a sign of reflux. Doctors sometimes use this test to see whether children with symptoms such as coughing or breathing difficulties have reflux.
An impedance probe is very similar to the esophageal pH probe but it can detect both acid and nonacid reflux. This probe is used in children who are taking medications that suppress stomach acid to see whether they still have reflux, to see whether the reflux is associated with other symptoms, and to confirm that the medications are working to lessen acid reflux.
A gastric emptying scan is done to determine how quickly the stomach empties. In a gastric emptying scan (milk scan), the child drinks a beverage (such as milk, breast milk, or formula) that contains a small amount of mildly radioactive material. This material is harmless to the child. A special camera or scanner that is highly sensitive to radiation can detect where the material is in the child’s body. The camera can see how rapidly the material leaves the stomach and whether there is reflux, aspiration, or both.
In upper endoscopy, the child is sedated, and a small flexible tube with a camera on the end (endoscope) is passed through the mouth into the esophagus and stomach. Doctors may do upper endoscopy if they need to see whether the reflux has caused damage to the esophagus (esophagitis), an ulcer, or irritation or if they need to obtain a sample for a biopsy. Endoscopy can also help determine whether the symptoms of reflux are not due to something else such as an allergy, infection, or celiac disease. Bronchoscopy is a similar test in which doctors use an endoscope to examine the voice box (larynx) and airways. Bronchoscopy can help doctors decide whether reflux is a likely cause of lung or breathing problems.
An ultrasound of the abdomen may be done for infants who forcefully vomit, especially those who have lost weight and have complications of dehydration. The ultrasound can help doctors determine whether the muscular valve between the stomach and small intestine (called the pylorus) is normal or whether the infant may have pyloric stenosis.
Treatment of Gastroesophageal Reflux
For spitting up in infants, parents may use thickened formula, special positioning, and frequent burping
For breastfed infants, changing the mother's diet
For formula-fed infants, a trial of a hypoallergenic formula
Other measures to reduce reflux
Sometimes medications
Rarely surgery
Treatment of reflux depends on the child’s age and symptoms.
For infants who just have mild spitting up when being burped, doctors reassure parents that there is nothing more serious happening. They may recommend no treatment or may suggest measures such as thickening formula for feedings, special positioning, and frequent burping. Formula can be thickened by adding 1 to 3 teaspoons of rice cereal per ounce of formula. The nipple may have to be cross-cut to allow the formula to flow. Infants with reflux should be fed in an upright or semi-upright position and then maintained in an upright, nonsitting position for 20 to 30 minutes after eating (sitting, as in an infant seat, increases stomach pressure and is not helpful). In addition, burping the infant after every 1 to 2 ounces can help decrease pressure in the stomach by expelling the air the infant swallows.
Cow's milk allergy can occur even in breastfed infants and can cause GERD. Mothers can try not drinking cow's milk for several weeks and see whether it is helpful.
Formula-fed infants may benefit from a 2- to -4-week trial of a hypoallergenic formula because they may have a food intolerance or allergy. Hypoallergenic formula can even be helpful for infants who do not have a food allergy because the formula helps the stomach empty faster.
Because of safety concerns, doctors no longer recommend raising the head of the crib or bed. Doctors do recommend that infants should be put on their back to sleep. This position reduces the risk of sudden infant death syndrome (SIDS).
Older children also should avoid eating 2 to 3 hours before bedtime, drinking carbonated beverages and those that contain caffeine, taking certain medications (such as those with anticholinergic effects), eating certain foods (such as chocolate or fatty foods), and overeating.
All children should be kept away from caffeine and tobacco smoke.
Medications for reflux
If changes in feeding and positioning do not control symptoms, doctors may prescribe medications. Several types of medications are available for reflux:
Those that neutralize acid
Those that suppress acid production
Those that improve the movement of the digestive tract (promotility medications)
Antacids are medications that neutralize stomach acid. These medications work quickly to relieve symptoms such as heartburn.
Acid-suppressing medications may be required for children with more severe disease. By reducing stomach acid, these medications lessen symptoms and allow the esophagus to heal. There are two types of acid-suppressing medications: histamine-2 (H2) blockers and proton pump inhibitors (PPIs). H2 blockers do not suppress acid production quite as much as PPIs.
Promotility medications (such as erythromycin and baclofen) may help increase the speed at which the stomach empties. Improved stomach emptying should decrease stomach pressure, making reflux less likely to occur. Acid-suppressing medications and promotility medications may help infants who have gastroparesis.
Surgery for reflux
Rarely, reflux does not go away after medications are tried and is so severe that doctors recommend surgery. The most common surgical procedure is a fundoplication. In fundoplication, the surgeon wraps the top of the stomach around the lower end of the esophagus to make that junction tighter and decrease reflux.
Some anatomic causes of reflux, vomiting, or both also may have to be corrected surgically.







