




Urinary tract infections are caused by bacteria.
Infants and young children who have urinary tract infections sometimes have structural abnormalities of their urinary system that make them more susceptible to urinary infection.
Newborns and infants may have no symptoms other than a fever, whereas older children have pain or burning during urination, pain in the bladder region, and a need to urinate frequently.
The diagnosis is based on an examination and culture of the urine.
Antibiotics are given to eliminate the infection.
Proper hygiene may help prevent urinary tract infections.
(For adults, see Overview of Urinary Tract Infections (UTIs).)
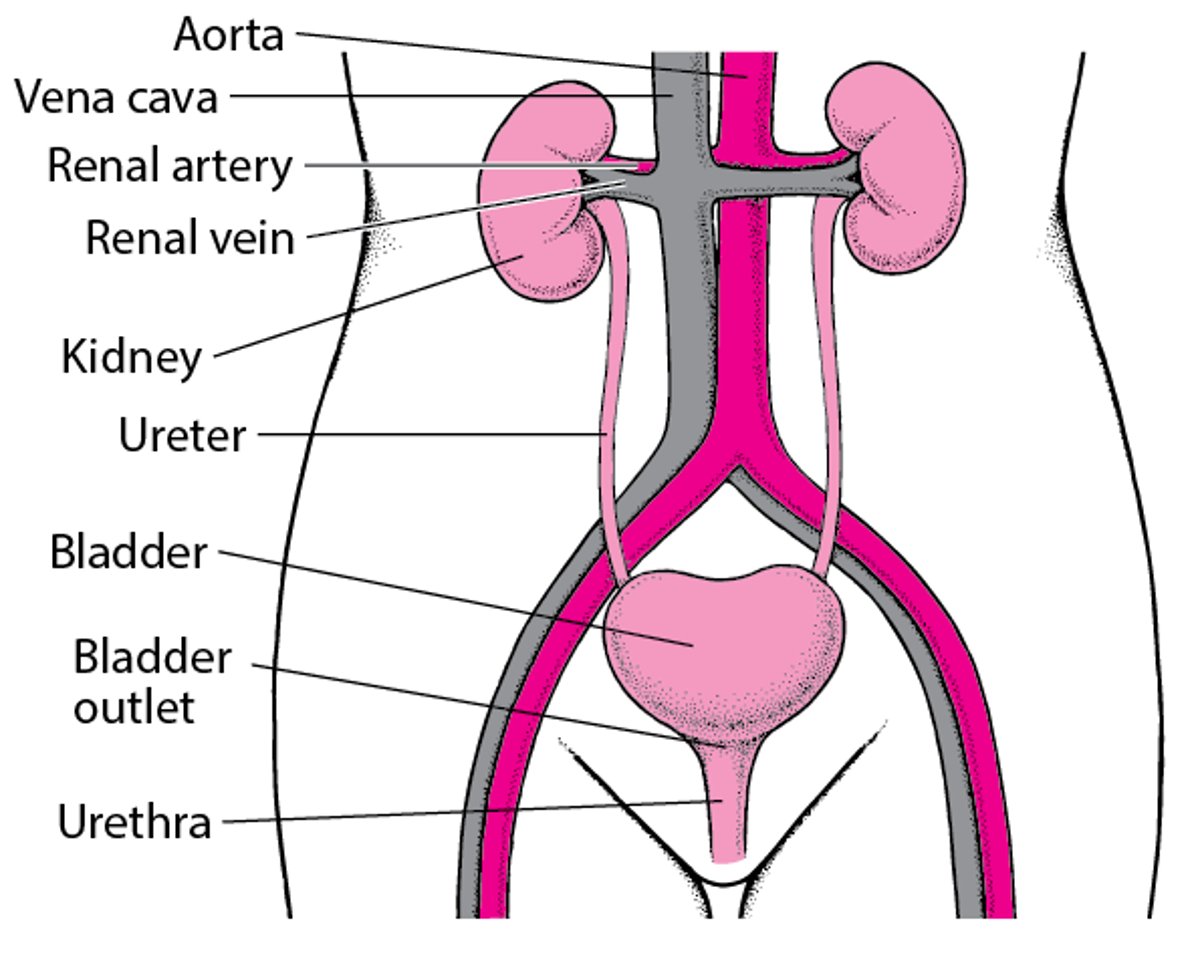
Urinary tract infections (UTIs) are common in childhood. Nearly all UTIs are caused by bacteria that enter the opening of the urethra (the tube that drains urine from the bladder out of the body) and move upward to the urinary bladder and sometimes the kidneys. Rarely, in severe infections, bacteria may enter the bloodstream from the kidneys and cause infection of the bloodstream (sepsis) or of other organs.
During infancy, boys are more likely to develop UTIs. Uncircumcised infant boys also are more prone to UTIs because bacteria tend to accumulate under the foreskin. After infancy, girls are much more likely to develop UTIs because their short urethras make it easier for bacteria to move up the urinary tract. Severe constipation or bowel dysfunction is also thought to be a cause of UTIs in infants and children.
However, infants and younger children who have UTIs more commonly have various structural abnormalities of their urinary system that make them more susceptible to urinary infection. These abnormalities include vesicoureteral reflux (VUR), which is an abnormality of the ureters (the tubes connecting the kidneys to the bladder) that allows urine to pass backward from the bladder up to the kidney, and a number of conditions that block the flow of urine. As many as 50% of newborns and infants with a UTI and 20 to 30% of school-aged children with a UTI have such abnormalities.
In older school-aged children and adolescents, diabetes, injury, and, in females, sexual intercourse increase the risk of developing a UTI.
The Urinary Tract

Many infants and preschool children with a UTI—particularly those with fever—have both a bladder infection and a kidney infection. If the kidney is repeatedly infected and VUR is severe, about 25% of children develop some scarring of the kidneys. If there is little or no VUR, very few children have scarring of the kidneys. Scarring is a concern because it may lead to high blood pressure and impaired kidney function in adulthood.
(See also Overview of Bacterial Infections in Childhood.)
Symptoms of UTI in Children
Newborns with a UTI may have no symptoms other than a fever. Sometimes they do not eat well or grow well, are sluggish (lethargic), vomit, or have diarrhea. Newborns may develop a serious bodywide infection (sepsis) from an untreated UTI.
Infants and children under age 2 years with a UTI may have fever, vomiting, diarrhea, abdominal pain, or foul-smelling urine.
Children over age 2 years with a UTI usually have the typical symptoms of a bladder or kidney infection similar to adults.
Children with bladder infections (cystitis) usually have pain or burning during urination, a need to urinate frequently and urgently, and pain in the bladder region. They may have difficulty urinating or holding urine (urinary incontinence). Urine may smell foul.
Children with kidney infections (pyelonephritis) typically have pain in the side or back over the affected kidney, high fever, chills, and a general feeling of illness (malaise).
Children who have urinary tract abnormalities may have a mass in the abdomen, enlarged kidneys, an abnormal opening to the urethra, or possible deformities in the lower spine. Children who do not have a forceful stream of urine may have a blockage in one of the tubes that transports urine from the kidneys to the bladder (ureters) or may not be able to control their bladder because of a nerve problem.
Did You Know...
|
Diagnosis of UTI in Children
Urine tests
Imaging of the urinary tract
Sometimes blood tests
Urine tests
A doctor diagnoses a UTI by obtaining a sample of urine (urinalysis) and sending it for a urine culture to grow any bacteria present.
A UTI increases levels of white blood cells and bacteria in the urine. To detect these white blood cells and bacteria, a laboratory technician examines the urine under a microscope and does several chemical tests. The technician also does a culture of the urine to grow and identify any bacteria present. The culture is the most important of these tests.

Toilet-trained children may provide a urine sample by using the clean-catch method. In this method, the opening of the urethra is cleansed with a small pad that contains an antiseptic. Then the child urinates a small amount of urine into the toilet, washing out the urethra. Children then stop urinating in the toilet and continue urinating into a sterile cup.
Doctors obtain urine from younger children and infants by inserting a thin, flexible, sterile tube (catheter) through the urethral opening into the bladder. This process is called catheterization.
In some newborn and infant boys, the foreskin is too tight to be pulled back over the head of the penis, blocking the urethral opening, so the doctor needs to withdraw urine from the bladder with a needle inserted through the skin just above the pubic bone.
Sometimes doctors tape a urine collection bag to the area between the genitals and the anus to collect urine for other tests. Urine collected in this manner is not useful for the diagnosis of UTI because it is contaminated with bacteria and other material from the skin.
Imaging tests
Many structural abnormalities of the urinary system are diagnosed before birth during prenatal ultrasonography. Sometimes, however, children have abnormalities that cannot be seen during prenatal ultrasonography. Therefore, boys of all ages and girls younger than 3 years who develop even a single UTI usually need further tests to look for structural abnormalities of the urinary system. Older girls who have had recurring UTIs also need these tests.
The tests include
Ultrasonography of the kidneys and bladder
Possibly voiding cystourethrography (VCUG)
Sometimes radionuclide cystography (RNC) or radionuclide kidney scans
Ultrasonography is done to identify abnormalities and blockages of the kidneys and bladder.
Voiding cystourethrography (VCUG) may be done to further identify abnormalities of the kidneys, ureters, and bladder and can identify when the flow of urine is partially reversed (reflux). For voiding cystourethrography, a catheter is passed through the urethra into the bladder, a dye is instilled through the catheter, and x-rays are taken before and after the child urinates. Voiding cystourethrography may be done if ultrasonography is abnormal or if children have repeated UTIs.
Radionuclide cystography is similar to voiding cystourethrography except that a radioactive agent is placed in the bladder and images are taken using a nuclear scanner. This procedure exposes the child's ovaries or testes to less radiation than voiding cystourethrography. However, radionuclide cystography is much more useful for monitoring the healing of reflux than for diagnosing it, because the structures are not outlined as well as in voiding cystourethrography.
In another type of nuclear scanning, a radioactive substance (called dimercaptosuccinic acid or DMSA) is injected into a vein and enters the kidneys. The substance is detected by special cameras that take pictures of the insides of the kidneys. DMSA scanning may be used to confirm the diagnosis of pyelonephritis and identify scarring of the kidneys. It is most useful for children with severe UTIs or UTIs caused by certain bacteria.
Blood tests
Blood tests and tests that determine whether inflammation is present (C-reactive protein and erythrocyte sedimentation rate) are done in children whose urine tests results do not confirm a diagnosis, or are done to help doctors diagnose a kidney infection in addition to a bladder infection.
Blood cultures are done in infants who have a UTI and in children over age 1 to 2 years who are very ill.
Treatment of UTI in Children
Antibiotics
Sometimes surgery
UTIs are treated with antibiotics. Children who appear very ill or whose initial test results suggest a UTI are given antibiotics before culture results are available. Otherwise, doctors wait for culture results to confirm the diagnosis of UTI. Children who are very ill and all newborns receive antibiotics by injection into either a muscle (intramuscularly) or a vein (intravenously). Other children are given antibiotics by mouth. Treatment typically lasts about 7 to 10 days. Children who require tests to diagnose structural abnormalities often continue antibiotic treatment at a lower dose until tests are complete.
Some children with structural abnormalities of the urinary tract require surgery to correct the problem. Others need to take antibiotics daily to prevent infection (known as prophylaxis). Children who have severe VUR usually need surgery and need to take antibiotics until they have the surgery. Children who have VUR that is not severe are monitored closely and may be given antibiotics.
Certain cases of mild to moderate VUR resolve without treatment.
Prognosis for UTI in Children
Children who receive proper treatment rarely develop kidney failure (the inability of the kidneys to adequately filter metabolic waste products from the blood) unless they have urinary tract abnormalities that cannot be repaired. However, repeated UTIs, especially in children who have severe VUR, are thought to cause kidney scarring, which may lead to high blood pressure and chronic kidney disease in adulthood.
Prevention of UTI in Children
Prevention of UTIs is difficult, but proper hygiene may help.
Girls should be taught to wipe themselves from front to back (as opposed to back to front) after a bowel movement and after urinating to minimize the chance of bacteria entering the urethral opening.
Avoiding frequent bubble baths, which may irritate the skin around the urethral opening, may help lessen the risk of UTIs in both boys and girls.
Circumcision of boys lowers their risk of UTIs during infancy. Boys who are circumcised are infected with UTIs only 1/10th as often as boys who are not circumcised, but it is not clear whether this advantage by itself is a sufficient reason for circumcision.
Regular urination and regular bowel movements (especially treatment of severe constipation) may lessen the risk of UTIs.







