



- Overview of Foot and Ankle Disorders
- Achilles Tendon Enthesopathy
- Anterior Achilles Tendon Bursitis
- Apophysitis of the Calcaneus
- Bunion
- Freiberg Disease
- Hammer Toe Deformity
- Inferior Calcaneal Bursitis
- Interdigital Neuroma
- Medial and Lateral Plantar Nerve Entrapment
- Metatarsalgia
- Metatarsophalangeal Joint Pain
- Plantar Fasciitis
- Plantar Fibromatosis
- Posterior Achilles Tendon Bursitis
- Sesamoiditis
- Tarsal Tunnel Syndrome
- Tibialis Posterior Tendinosis and Tibialis Posterior Tenosynovitis



(See also Overview of Foot and Ankle Disorders.)
Metatarsophalangeal joint pain is a common cause of metatarsalgia. Metatarsophalangeal joint pain most commonly results from misalignment of the joint surfaces with altered foot biomechanics, causing joint subluxations, flexor plate tears, capsular impingement, and joint cartilage destruction (osteoarthrosis). Misaligned joints may cause synovial impingement, with minimal if any warmth and swelling (osteoarthritic synovitis).
The second metatarsophalangeal joint is commonly affected. It develops laxity to the collateral ligaments due to rigid hammer toe deformities which allows the toe to sublux and dislocate out of the joint. As the disjointed toe attempts to strike the ground during ambulation, it causes a retrograde buckling force on the metatarsal head, which results in pain and abnormal pressure at the plantar aspect of the forefoot. Usually, inadequate first ray (first cuneiform and first metatarsal) function results from excessive pronation (the foot rolling inward and the hindfoot turning outward or everted), often leading to capsulitis, plantar plate injury, and hammer toe deformities. Overactivity of the anterior shin muscles in patients with pes cavus (high arch) and ankle equinus (shortened Achilles tendon that restricts ankle dorsiflexion) deformities tends to cause dorsal joint subluxations with retracted (clawed) digits and retrograde, increased submetatarsal head pressure and pain.
Metatarsophalangeal joint subluxations also occur as a result of chronic inflammatory arthropathy, particularly rheumatoid arthritis. Metatarsophalangeal joint pain with weight bearing and a sense of stiffness in the morning can be significant early signs of early rheumatoid arthritis. Inflammatory synovitis and interosseous muscle atrophy in rheumatoid arthritis lead to subluxations of the lesser metatarsophalangeal joints as well, resulting in hammer toe deformities. Consequently, the metatarsal fat pad, which usually cushions the stress between the metatarsals and interdigital nerves during walking, moves distally under the toes; interdigital (Morton) neuroma may result. To compensate for the loss of cushioning, adventitial calluses and bursae may develop. Coexisting rheumatoid nodules beneath or near the plantarflexed metatarsal heads may increase pain.
The first metatarsophalangeal joint is the most common location of osteoarthritis in the foot. The joint cartilage is damaged due to trauma, deformity (eg, bunion) or systemic arthritides (eg. gout, rheumatoid arthritis) and results in a decreased dorsiflexion of the hallux. As the disorder progresses, the loss of dorsiflexion prevents the foot from functioning properly in the push-off phase of gait. The sesamoids located within the flexor hallucis brevis tendon fibrose and lose their inherent mechanical advantage for propulsion of the great toe off the ground. This causes an unintended use of the second metatarsophalangeal joint to compensate for the lack of first metatarsophalangeal joint range of motion, which causes pain and laxity at the second metatarsophalangeal joint.
Metatarsophalangeal joint pain may also result from functional hallux limitus, which limits passive and active joint motion at the first metatarsophalangeal joint. Patients usually have foot pronation disorders that result in elevation of the first ray with lowering of the medial longitudinal arch during weight bearing. As a result of the first ray elevation, the proximal phalanx of the great toe cannot freely extend on the first metatarsal head; the result is jamming at the dorsal joint leading to osteoarthritic changes and loss of joint motion. Over time, pain may develop. As joint space narrows due to arthritis, hallux rigidus can occur.
Acute arthritis can occur secondary to systemic arthritides such as gout, rheumatoid arthritis, and spondyloarthropathy.
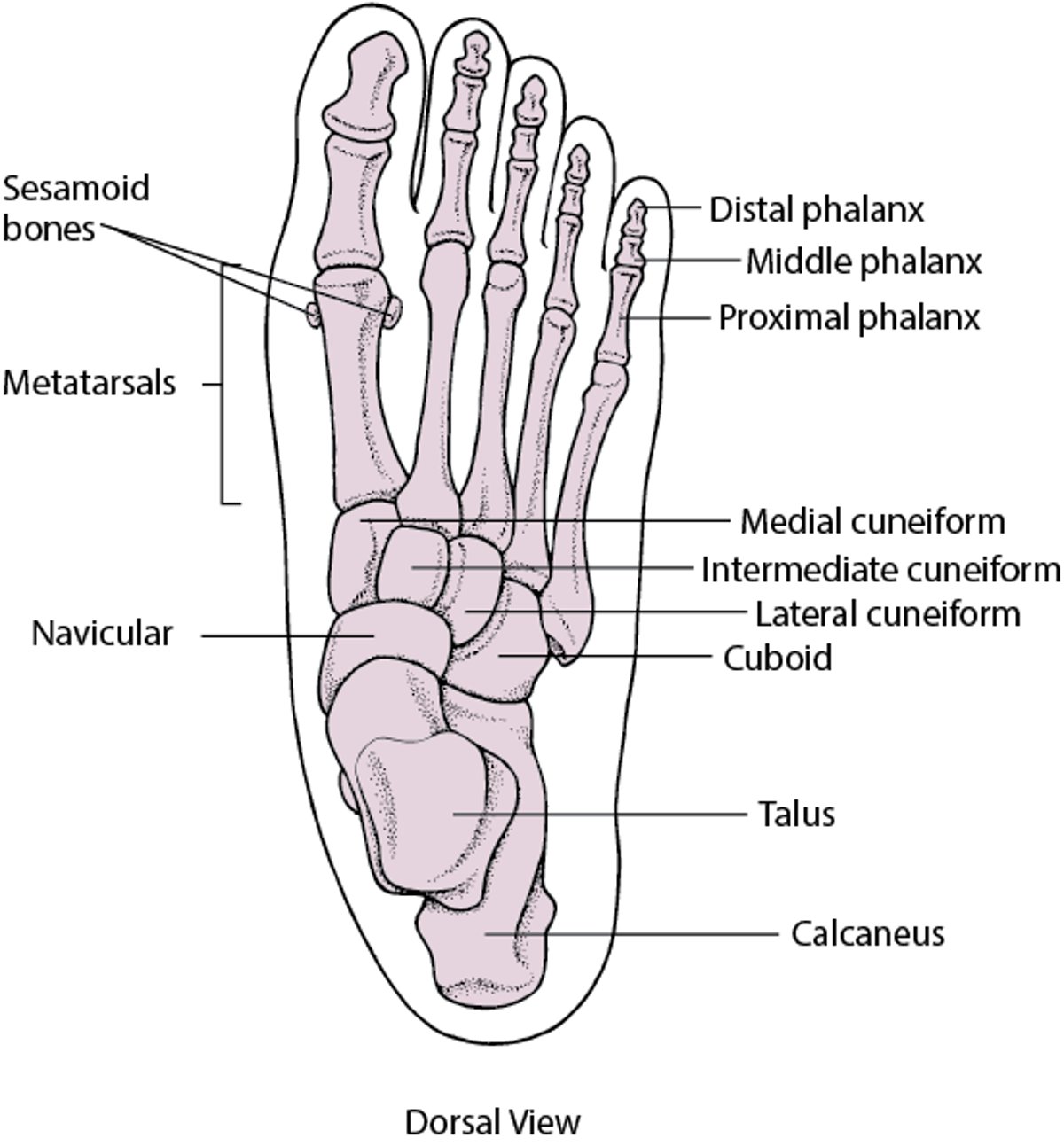
Bones of the Foot

Symptoms and Signs of Metatarsophalangeal Joint Pain
Symptoms of metatarsophalangeal joint pain include pain on walking. Dorsal and plantar joint tenderness is usually present on palpation and during passive range of motion. Mild swelling with minimal warmth may occur initially with osteoarthritis. Significant warmth, swelling, or erythema suggests inflammatory arthropathies or infection.
Diagnosis of Metatarsophalangeal Joint Pain
Mainly clinical evaluation
Exclusion of infection or arthropathy if signs of inflammation
Metatarsophalangeal joint pain can usually be differentiated from interdigital neuroma by the absence of burning, numbness, tingling, and interspace pain, but these symptoms may result from joint inflammation; if so, palpation can help with differentiation.
Monarticular warmth, erythema, and swelling indicate infection until proven otherwise, although gout is more likely. When warmth, redness, and swelling involve multiple joints, evaluation for a systemic cause of joint inflammation (eg, gout, rheumatoid arthritis, psoriatic arthritis, viral-associated arthritis, enteropathic arthritis), including laboratory tests for systemic rheumatic diseases (eg, anticyclic citrullinated peptide [anti-CCP] antibody, rheumatoid factor [RF], erythrocyte sedimentation rate, C-reactive protein), is indicated. Imaging of the foot with color Doppler ultrasonography may be helpful to detect synovial proliferation, inflammation, and possible early erosions or findings suggestive of deposition of monosodium urate ("double contrast sign").

Treatment of Metatarsophalangeal Joint Pain
Orthoses
If present, treatment of underlying systemic rheumatic disease
Foot orthoses with metatarsal pads may help redistribute and relieve pressure from the noninflamed joints. With excess subtalar eversion or when the feet are highly arched, an orthotic that corrects these abnormal alignments should be prescribed. Shoes with rocker sole modifications may also help. For hallux limitus or rigidus, orthosis modifications may further help to plantarflex the first ray to improve metatarsophalangeal joint motion and reduce pain. If the first ray elevation cannot be reduced by these means, an extended first ray elevation pad may be helpful. For more severe limitation of first metatarsophalangeal motion or pain, the use of rigid orthoses, carbon fiber plates, or external shoe bars or rocker soles may be necessary to reduce motion at the joint.
If inflammation (synovitis) is present, medications to treat the underlying inflammatory condition (eg, rheumatoid arthritis) are indicated. An injection of a local corticosteroid/anesthetic mixture may be useful for immediate pain relief (see Considerations for Using Corticosteroid Injections).
Surgery may be needed if conservative therapies are ineffective.
Key Points
Metatarsophalangeal joint pain most often results from misalignment of joint surfaces, causing synovial impingement with only minimal warmth and swelling, but may be the initial manifestation of rheumatoid arthritis.
Patients have dorsal and plantar joint tenderness with usually minimal signs of acute inflammation.
Diagnose metatarsophalangeal joint pain by the absence of burning, numbness, tingling, and interspace pain (suggesting interdigital nerve pain) and by palpation.
Correct foot biomechanics with orthoses.
Treat underlying systemic rheumatic disease (eg, rheumatoid arthritis), if present.







