


Asthma is a recurring inflammatory lung disorder in which certain stimuli (triggers) inflame the airways and cause them to temporarily narrow, resulting in difficulty breathing.



Asthma triggers include viral infections, pets, smoke, perfume, pollen, mold, and dust mites.
Wheezing, cough, shortness of breath, chest tightness, and difficulty breathing are symptoms of asthma.
The diagnosis is based on a child's repeated wheezing episodes, a family history of asthma, and sometimes the results of tests that measure how well the lungs function.
Treatment includes bronchodilators and inhaled corticosteroids.
Many children who wheeze in childhood do not have asthma later in life.
Asthma symptoms can often be prevented by avoiding triggers.
(See also Asthma in adults.)
Although asthma can develop at any age, it most commonly begins in childhood, particularly in the first 5 years of life. Some children continue to have asthma into their adult years. In other children, asthma resolves. Sometimes, children who doctors thought had asthma actually had another disorder that caused similar symptoms (see Wheezing in Infants and Young Children).
Asthma is one of the most common chronic diseases of childhood, affecting approximately 6 million children in the United States. It occurs more frequently in boys before puberty and in girls after puberty. Asthma is a leading cause of hospitalization for children and is the number one chronic condition causing school absenteeism.
Most children with asthma are able to participate in normal childhood activities, except during flare-ups. A smaller number of children have moderate or severe asthma and need to take daily preventive medications to enable them to engage in sports and normal play.

Triggers for Asthma in Children
For unknown reasons, children with asthma respond to certain stimuli (triggers) in ways that children without asthma do not. Children with asthma may have certain genes that may make them more susceptible to react to certain triggers. Most children with asthma also have parents and siblings or other relatives with asthma, which is evidence that genetics plays a role in asthma.
There are many potential triggers, and most children respond to only a few. In some children, specific triggers for flare-ups cannot be identified.
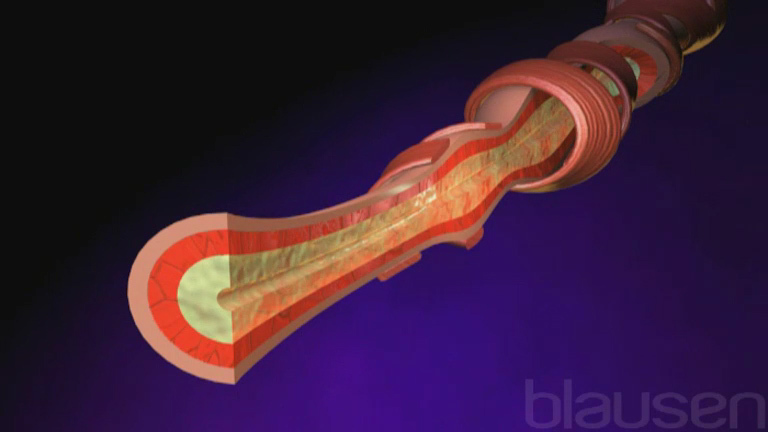
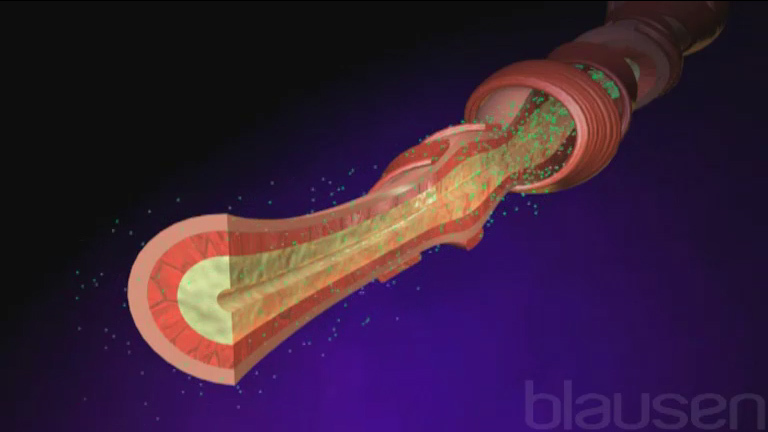
The triggers all result in a similar response. Certain cells in the airways release chemical substances. These substances
Cause the airways to become inflamed and swollen
Stimulate the muscle cells in the walls of the airways to contract
Increase mucus production in the airways
Each of these responses contributes to a sudden narrowing of the airways (an asthma attack). In most children, the airways return to normal between asthma attacks. Repeated stimulation by these chemical substances increases mucus production in the airways, causes shedding of the cells lining the airways, and enlarges the muscle cells in the walls of the airways.
Common Asthma Triggers
Triggers | Examples |
|---|---|
Allergens | Dust or house mites, molds, pollen, animal dander, cockroach feces, pets, and feathers |
Exercise | Particularly exercise in cold or dry air |
Irritants | Firsthand and secondhand tobacco smoke, perfumes, wood smoke, cleaning products, scented candles, air pollution, strong odors, and irritating fumes |
Viral respiratory infections* | In young children: Respiratory syncytial virus, rhinovirus, parainfluenza virus infection In older children: Upper respiratory infections (particularly with rhinovirus) and pneumonia |
Other | Emotions (such as anxiety, anger, and excitement) Aspirin or other nonsteroidal anti-inflammatory drugs (NSAIDs) |
* Viral infections are the most common triggers in children. | |
Risk Factors for Asthma in Children
Doctors do not completely understand why some children develop asthma, but a number of risk factors are recognized:
Inherited and prenatal factors
Allergen exposure
Viral infections
Diet
If one or both parents have asthma, the risk of asthma is increased in their children. Children whose mothers smoked during pregnancy may be more likely to develop asthma. Asthma also has been linked to other factors related to the mother, such as young maternal age, poor maternal nutrition, and lack of breastfeeding. Prematurity and low birth weight are also risk factors.
In the United States, children in urban environments are more likely to develop asthma, particularly if they are from lower socioeconomic groups. Although it is not entirely understood, it is believed that poorer living conditions, greater potential exposure to triggers, and less access to health care contribute to the higher incidence of asthma in these groups. Asthma affects a higher percentage of non-Hispanic Black and Puerto Rican children in the United States.
Children who are exposed to high concentrations of certain allergens, such as dust mites or cockroach feces, at an early age are more likely to develop asthma. However, doctors have noticed that asthma is more common among children living in very clean, hygienic environments where they are exposed to fewer infectious diseases than children living in environments where they are exposed to more infectious diseases. Thus, doctors think that perhaps childhood exposure to certain substances and infections may actually help children's immune system learn not to overreact to triggers.
Most children who are having an asthma attack or who have been hospitalized for asthma have a viral infection (usually rhinovirus or the common cold). Children who have bronchiolitis at an early age often wheeze with subsequent viral infections. The wheezing may at first be interpreted as asthma, but these children are no more likely than others to have asthma during adolescence.
Diet may be a risk factor. Children who do not consume enough of vitamins C and E and omega-3 fatty acids or who have obesity may be at higher risk of asthma.
Symptoms of Asthma in Children
As the airways narrow during an asthma attack, the child develops difficulty breathing, chest tightness, and coughing, typically accompanied by wheezing. Wheezing is a high-pitched noise heard when the child breathes out.

Not all asthma attacks cause wheezing, however. Mild asthma, particularly in very young children, may result only in a cough. Some older children with mild asthma tend to cough only when exercising or when exposed to cold air.
In a severe attack, breathing becomes visibly difficult, wheezing usually becomes louder, the child breathes faster and with greater effort, and the ribs stand out when the child breathes in (inspiration). With very severe attacks, the child gasps for breath and sits upright, leaning forward. The skin is sweaty and pale or blue-tinged. Children who have frequent severe attacks sometimes have slowed growth, but their growth usually is similar to that of other children by adulthood.
In an extremely severe asthma attack, children may not wheeze because there is too little air flowing to even make a noise.
Diagnosis of Asthma in Children
Wheezing and family history of asthma or allergies
Sometimes allergy testing
Sometimes pulmonary function tests
A doctor suspects asthma in children who have repeated episodes of wheezing, particularly when family members are known to have asthma or allergies. However, asthma is only one of several causes of wheezing.
X-rays of the chest are rarely necessary for the diagnosis of asthma in children. X-rays are usually done only if doctors think that the child's symptoms might be caused by a different disorder, such as pneumonia. Doctors sometimes do allergy testing to help determine potential triggers.
Children with frequent wheezing episodes may be tested for other disorders, such as cystic fibrosis or gastroesophageal reflux. Older children sometimes undergo tests that are used to measure how well the lungs function (pulmonary function tests). In most children with asthma, lung function is normal between flare-ups.
Older children or adolescents known to have asthma often use a peak flow meter (a small handheld device that records how fast a person can blow out air) to measure the degree of airway narrowing. This device can be used at home. Doctors and parents can use this measurement to assess the child's condition during an attack and between attacks. X-rays are not done during an attack in children known to have asthma unless doctors suspect another disorder such as pneumonia or a collapsed lung.


Treatment of Asthma in Children
For acute attacks, bronchodilators and sometimes corticosteroids
For chronic asthma, inhaled corticosteroids (sometimes combined with bronchodilators) and possibly leukotriene modifiers and/or cromolynFor chronic asthma, inhaled corticosteroids (sometimes combined with bronchodilators) and possibly leukotriene modifiers and/or cromolyn
Treatment is given to resolve sudden (acute) attacks and sometimes to prevent attacks.
Children who have mild, very infrequent attacks usually take medications only during an attack. Children who have more frequent or severe attacks also need to take medications even when they are not having attacks. Different medications are used depending on the frequency and severity of the attacks. Children with infrequent attacks that are not very severe usually take a low dose of an inhaled corticosteroid or a leukotriene modifier (montelukast or zafirlukast) every day to help prevent attacks. These medications reduce inflammation by blocking the release of the chemical substances that inflame the airways.Children who have mild, very infrequent attacks usually take medications only during an attack. Children who have more frequent or severe attacks also need to take medications even when they are not having attacks. Different medications are used depending on the frequency and severity of the attacks. Children with infrequent attacks that are not very severe usually take a low dose of an inhaled corticosteroid or a leukotriene modifier (montelukast or zafirlukast) every day to help prevent attacks. These medications reduce inflammation by blocking the release of the chemical substances that inflame the airways.
Acute attacks (flare-ups)
Treatment of an acute asthma attack consists of
Opening the airways (bronchodilation)
Stopping inflammation
A variety of inhaled medications open the airways (bronchodilators—see Treating Asthma Attacks). Typical examples are albuterol and ipratropium. Doctors do not recommend using long-acting bronchodilators, such as salmeterol and formoterol, as the only treatment for children. ). Typical examples are albuterol and ipratropium. Doctors do not recommend using long-acting bronchodilators, such as salmeterol and formoterol, as the only treatment for children.
Children and adolescents should use a metered-dose inhaler with a spacer or valve-holding chamber (see figure How to Use a Metered-Dose Inhaler With a Spacer). The spacer optimizes delivery of the medication to the lungs and minimizes the chance of side effects.

How to Use a Metered-Dose Inhaler With a Spacer
|

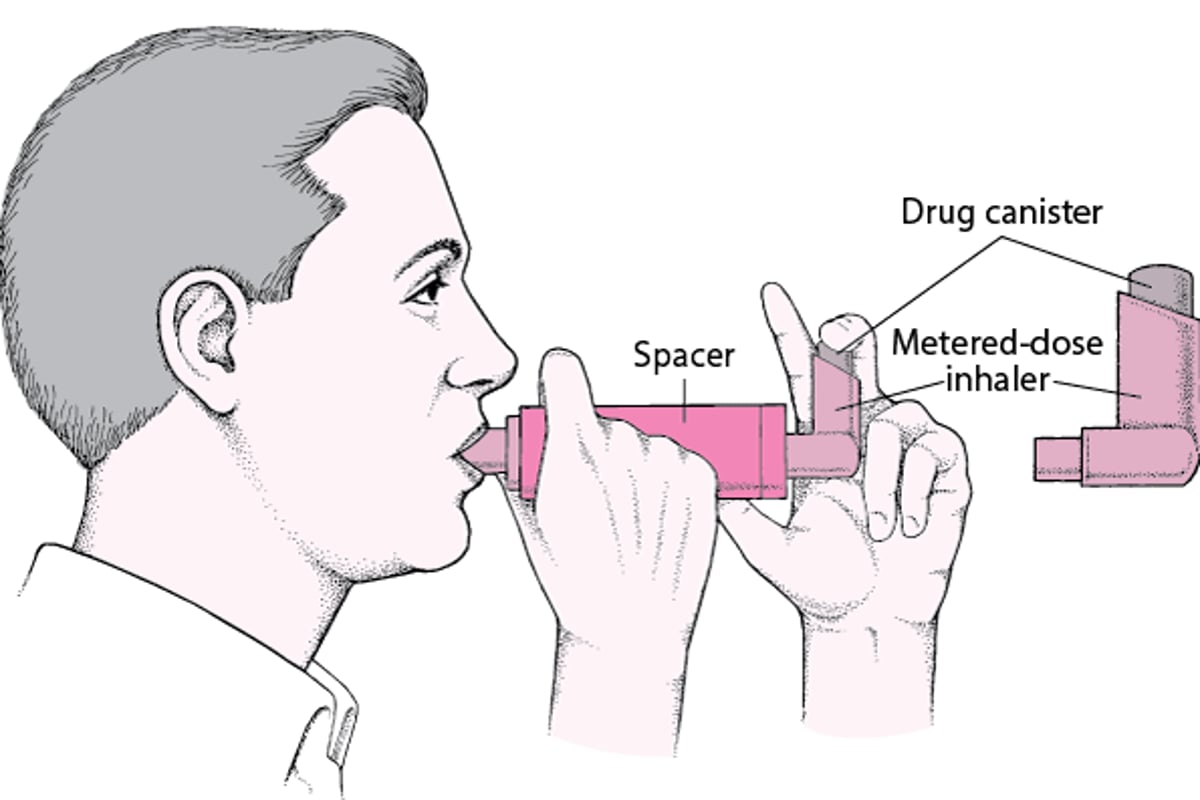
Infants and very young children sometimes can use an inhaler and spacer if an infant-sized mask is attached.
Children who cannot use inhalers may receive inhaled medications at home through a mask connected to a nebulizer (a small device that creates a mist of the medication by using compressed air). Inhalers and nebulizers are equally effective at delivering the medications, but most parents find the inhaler and spacer much more convenient and easier to use.

Albuterol also can be taken by mouth, but this route is less effective and may have more side effects than inhalation and usually is used only in infants who do not have a nebulizer and are too young to use an inhaler. Children with moderately severe attacks also may be given corticosteroids by mouth or injection.Albuterol also can be taken by mouth, but this route is less effective and may have more side effects than inhalation and usually is used only in infants who do not have a nebulizer and are too young to use an inhaler. Children with moderately severe attacks also may be given corticosteroids by mouth or injection.
Children with very severe attacks are treated in the hospital with bronchodilators given in a nebulizer or an inhaler at least every 20 minutes initially. Sometimes doctors use injections of epinephrine or terbutaline (bronchodilators) in children with very severe attacks if inhaled medications are not effective rapidly enough. Doctors usually give corticosteroids by vein to children having a severe attack.Children with very severe attacks are treated in the hospital with bronchodilators given in a nebulizer or an inhaler at least every 20 minutes initially. Sometimes doctors use injections of epinephrine or terbutaline (bronchodilators) in children with very severe attacks if inhaled medications are not effective rapidly enough. Doctors usually give corticosteroids by vein to children having a severe attack.
Chronic asthma
Treatment of chronic asthma consists of
Taking inhaled corticosteroids daily and possibly other medications that control inflammation
Using an inhaler before exercise
Infants and children under age 5 who need treatment more than 2 times a week, who have more persistent asthma, or those at risk of frequent or more severe attacks should receive daily anti-inflammatory treatment with inhaled corticosteroids. These children may also be given an additional medication such as a leukotriene modifier (montelukast or zafirlukast), a long-acting bronchodilator (always mixed with an inhaled corticosteroid in a combination inhaler), or cromolyn. Medications are increased or decreased over time to achieve optimal control of the child’s asthma symptoms and to prevent severe attacks. If these medications do not prevent severe attacks, children may need to take corticosteroids by mouth. Children over age 5 and adolescents with asthma can be treated similarly to adults (see Infants and children under age 5 who need treatment more than 2 times a week, who have more persistent asthma, or those at risk of frequent or more severe attacks should receive daily anti-inflammatory treatment with inhaled corticosteroids. These children may also be given an additional medication such as a leukotriene modifier (montelukast or zafirlukast), a long-acting bronchodilator (always mixed with an inhaled corticosteroid in a combination inhaler), or cromolyn. Medications are increased or decreased over time to achieve optimal control of the child’s asthma symptoms and to prevent severe attacks. If these medications do not prevent severe attacks, children may need to take corticosteroids by mouth. Children over age 5 and adolescents with asthma can be treated similarly to adults (seeTreating Asthma Attacks).
Children who have attacks during exercise usually inhale a dose of bronchodilator just before exercising.
Children whose asthma is triggered by aspirin or other nonsteroidal anti-inflammatory drugs (NSAIDs) must avoid using these medications. This reaction, however, is very uncommon in children. Children whose asthma is triggered by aspirin or other nonsteroidal anti-inflammatory drugs (NSAIDs) must avoid using these medications. This reaction, however, is very uncommon in children.
Because asthma is a long-term disorder with a variety of treatments, doctors work with parents and children to make sure they understand the disorder as well as possible. Adolescents and mature younger children should participate in developing their own asthma management plans and establishing their own goals for therapy to improve adherence to treatment. Parents and children should learn how to determine the severity of an attack, when to use medications and a peak flow meter, when to call the doctor, and when to go to the hospital.
Parents and doctors should inform school nurses, child care providers, and other appropriate adults of the child's disorder and the medications being used. Some children may be permitted to use inhalers in school as needed, and others must be supervised by the school nurse.
Prognosis for Asthma in Children
Many children outgrow asthma. However, as many as 1 in 4 children either continue to have asthma attacks or the asthma symptoms resolve only to return (called relapse) when children are older. Children who have severe asthma are more likely to have asthma as adults. Other risk factors for persistence and relapse include female sex, smoking, development of asthma at a younger age, and sensitivity to household dust mites.
Although asthma causes a significant number of deaths each year, most of these are preventable with treatment. Thus, the prognosis is good for children who have access to treatment and who are able to follow their treatment plan.
Prevention of Asthma in Children
It is not yet known how to prevent a child with a family history of asthma from developing asthma. However, there is evidence that children of mothers who smoked during pregnancy are more likely to have asthma. Thus, pregnant women should not smoke, especially if there is a family history of asthma.
On the other hand, there are many things that can be done to prevent asthma symptoms or attacks in children who have asthma.
Asthma flare-ups often can be prevented by avoiding or trying to control whatever triggers a particular child's attacks. Children who have allergies should have the following items removed from their bedroom:
Feather pillows
Carpets and rugs
Drapes/curtains
Upholstered furniture
Soft or stuffed toys
Pets
Other potential sources of dust mites and allergens
Other ways to reduce allergens include
Using synthetic fiber pillows and impermeable mattress covers
Washing bed sheets, pillowcases, and blankets in hot water
Using dehumidifiers in basements and in other poorly aerated, damp rooms to reduce mold
Using steam to clean the home to reduce dust mite allergens
Cleaning the house and pest extermination to eliminate cockroach exposure
Eliminating smoking in the home
Secondhand tobacco smoke often worsens symptoms in children with asthma, so it is important to eliminate smoking at least in areas where the child spends time.
Other triggers, such as strong odors, irritating fumes, cold temperatures, and high humidity, should also be avoided or controlled when possible.
Because exercise is so important for a child's development, doctors usually encourage children to maintain physical activities, exercise, and sports participation and use an asthma medication immediately before exercising if needed.
Allergy shots (immunotherapy)
If a particular allergen cannot be avoided, a doctor may try to desensitize the child by using allergy shots, although the benefits of allergy shots for asthma are not well known.
Allergy shots are typically more effective in children than adults. If asthma symptoms are not significantly relieved after 24 months, the shots are usually stopped. If symptoms are relieved, the shots should be continued for 3 years or more. However, the optimum length of time to continue the shots is unknown.







