



- Огляд вроджених серцево-судинних аномалій
- Аортолегеневе вікно
- Дефект міжпередсердної перегородки (ASD)
- Дефект атріовентрикулярної перегородки
- Двостулковий аортальний клапан
- Коарктація аорти
- Вроджена коригована транспозиція магістральних артерій
- Подвоєння вихідного отвору правого шлуночка
- Аномалія Ебштейна
- Синдром Айзенменгера
- Гіпопластичний синдром лівого серця
- Відкрита артеріальна протока (ВАП)
- Стійкий артеріальний стовбур
- Тетралогія Фалло
- Повний аномальний легенево-венозне повернення (TAPVR)
- Транспозиція магістральних артерій (ТМА)
- Атрезія тристулкового клапана
- Дефект міжшлуночкової перегородки (ДШП)
- Інші вроджені аномалії серця
Persistent truncus arteriosus occurs when, during fetal development, the primitive truncus does not divide into the pulmonary artery and aorta, resulting in a single, large, arterial trunk that overlies a large, malalignment type ventricular septal defect. Consequently, a mixture of oxygenated and deoxygenated blood enters systemic, pulmonary, and coronary circulations. Symptoms include cyanosis and heart failure, with poor feeding, diaphoresis, and tachypnea. A normal first heart sound (S1) and a loud, single second heart sound (S2) are common; murmurs may vary. Before profound heart failure develops, peripheral pulses will be bounding because of the large run off from the proximal aorta to the pulmonary arteries. Diagnosis is by echocardiography, MRI, CT angiography, or cardiac catheterization. Medical treatment for heart failure is typically followed by early surgical repair.
Ресурси за темою


(See also Overview of Congenital Cardiovascular Anomalies.)
Persistent truncus arteriosus (see figure Truncus arteriosus) accounts for about 1% of congenital heart anomalies and 4% of critical congenital heart defects. About 35% of patients have 22q11 deletion syndrome, which includes DiGeorge syndrome and velocardiofacial syndromes. A severe form of truncus arteriosus is one associated with an interrupted aortic arch.
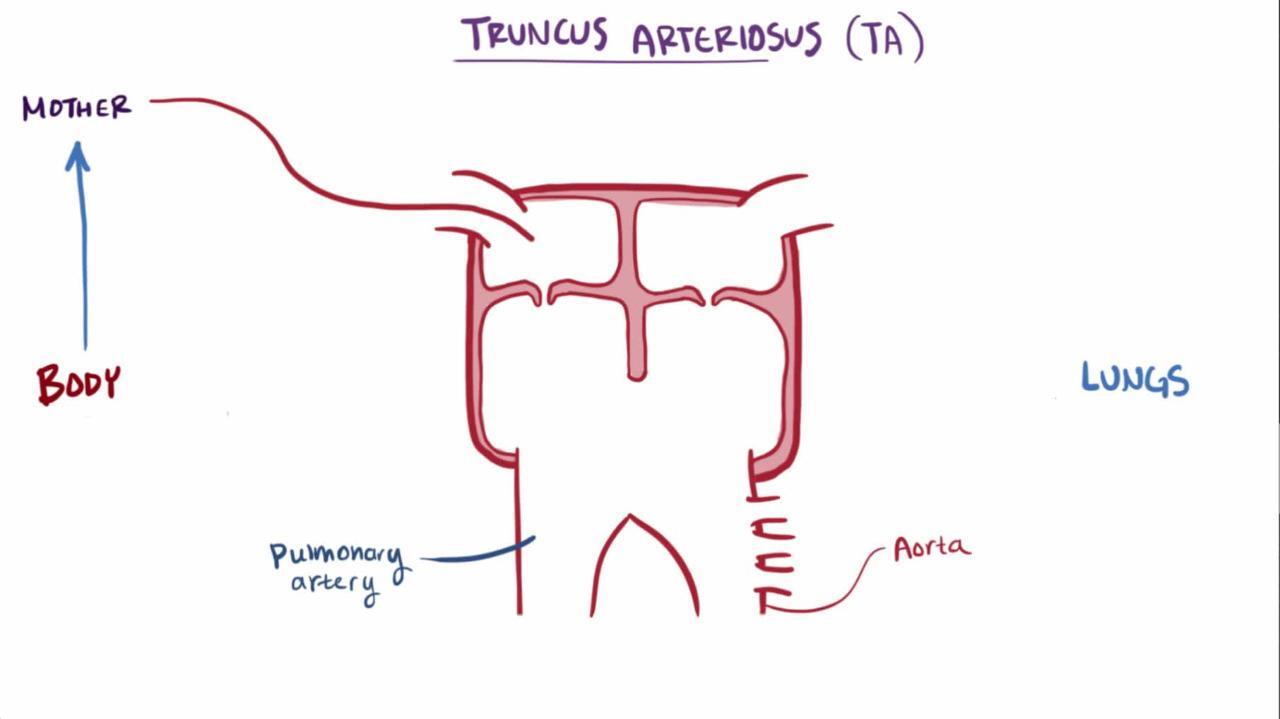
артеріальний стовбур
The primitive truncus does not divide into the pulmonary artery and aorta, resulting in a single large arterial trunk that overlies a large ventricular septal defect. |
IVC = inferior vena cava; LA = left atrium; LV = left ventricle; PA = pulmonary artery; PV = pulmonary veins; RA =right atrium; RV = right ventricle; SVC = superior vena cava. |


Класифікація
There are several classification systems in use.

An earlier classification, by Collett and Edwards, is
Type I: The main pulmonary artery arises from the truncus and then divides into the right and left pulmonary arteries.
Type II: The right and left pulmonary arteries arise separately (but adjacent to each other) from the posterior aspect of the truncus.
Type III: The right and left pulmonary arteries arise from the lateral aspects of the truncal root reasonably distant from each other.
Type IV: Both pulmonary arteries are supplied by collateral vessels from the descending aorta. (Type IV is now reclassified as tetralogy of Fallot with pulmonary atresia.)
An updated classification by Van Praagh consists of type A (truncus arteriosus withventricular septal defect [VSD]) and the very rare type B (truncus arteriosus without VSD). Type A is subdivided into 4 types:
Type A1: The main pulmonary artery arises from the truncus and then divides into right and left pulmonary arteries.
Type A2: The right and left pulmonary arteries arise separately from the posterior aspect of the truncus.
Type A3: One lung is supplied by a pulmonary artery branch that arises from the truncus and the other lung (usually the left) is supplied by a ductus-like collateral artery
Type A4: The truncus is a large pulmonary artery and the aortic arch is interrupted or coarctation is present.
The truncal valve may be quite abnormal and manifest with stenosis, regurgitation, or both. The valve is tricuspid in 69%, quadricuspid in 22%, and bicuspid in 9%. Other anomalies (eg, right aortic arch, interrupted aortic arch, coronary artery anomalies) may be present and may contribute to the high surgical mortality rate. A patent ductus arteriosus is exceedingly rare in Collett and Edwards types I, II, and III defects or in Van Praagh types A1 and A2 but is present in about half of patients with truncus arteriosus, most notably those with types A3 and A4 defects.
Physiologic consequences of truncus arteriosus include mild cyanosis, significant pulmonary overcirculation, and heart failure.
Symptoms and Signs of Persistent Truncus Arteriosus
Infants usually present with mild cyanosis and symptoms and signs of heart failure (eg, tachypnea, poor feeding, diaphoresis) in the first few weeks of life. Physical examination may detect a hyperdynamic precordium, increased pulse pressure with bounding pulses, a loud and single second heart sound (S2), and an ejection sound (click). A grade 2 to 4/6 systolic murmur is audible along the left sternal border (see table Heart Murmur Intensity). A mid-diastolic mitral flow murmur may be audible at the apex when pulmonary blood flow is increased. With truncal valve insufficiency, a high-pitched diastolic decrescendo murmur is audible over the mid left sternal border.
Diagnosis of Persistent Truncus Arteriosus
Chest x-ray and ECG
Echocardiography
Occasionally cardiac catheterization, cardiac MRI, or CT angiography
Diagnosis is suspected clinically, supported by chest x-ray and ECG, and established by 2-dimensional echocardiography with color flow and Doppler studies. Cardiac catheterization is occasionally necessary to delineate associated anomalies before surgery, but cardiac MRI or CT angiography may supplant the need for catheterization.
Chest x-ray shows varying degrees of cardiomegaly with increased pulmonary vascular markings, right aortic arch (in about 30%), and relatively high position of pulmonary arteries.
ECG commonly shows combined ventricular hypertrophy. Substantial pulmonary overcirculation may produce evidence of left atrial enlargement.
Treatment of Persistent Truncus Arteriosus
Medical treatment of heart failure (eg, diuretics, digoxin, angiotensin-converting enzyme inhibitors) before surgery
Surgical repair
Heart failure is treated vigorously with diuretics, digoxin, and angiotensin-converting enzyme (ACE) inhibitors, followed by early surgical repair. Prostaglandin infusion is beneficial to maintain ductal patency when there is interruption or coarctation of the aortic arch, in which case right-to-left shunt through the ductus provides systemic blood flow.
Surgical management consists of repair during the neonatal period. The ventricular septal defect is closed so that the left ventricle ejects into the truncal root. Usually, continuity between the right ventricle and the confluence of the pulmonary arteries is achieved using a conduit with or without a valve. Some centers have reported good success using a non conduit approach, in which the left atrial appendage is used as the posterior wall of the pulmonary outflow and a patch is used as the anterior wall, with or without the insertion of a monocusp valve.
When a conduit is placed during early infancy, its size becomes inadequate as children grow, and the conduit must be revised during childhood. When the patient's own tissue is used for part of this outflow tract, there is the potential for growth of the conduit as the child grows.
Branch pulmonary artery stenosis is a common sequela and is often effectively treated with transcatheter balloon dilation with or without stent placement. Surgical mortality rates are as low as 10%.
Endocarditis prophylaxis is recommended preoperatively but is required only for the first 6 months after repair unless there is a residual defect adjacent to a surgical patch or prosthetic material.
Ключові моменти
In persistent truncus arteriosus, the primitive truncus does not divide into the pulmonary artery and aorta, resulting in a single large arterial trunk that overlies a large ventricular septal defect (VSD).
Different types are distinguished based on the origin of the pulmonary arteries and associated defects.
Patients present with mild cyanosis, significant pulmonary overcirculation, and heart failure; a grade 2 to 4/6 systolic murmur is audible along the left sternal border and a mid-diastolic mitral flow murmur may be audible at the apex, and bounding peripheral pulses.
Treat heart failure with diuretics, digoxin, and ACE inhibitors; prostaglandin infusion is beneficial to maintain duct patency only in patients with type A4 truncus with interrupted aortic arch or coarctation.
Do surgical repair early; one or more revisions are usually needed as children grow.
Більше інформації
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
American Heart Association: Common Heart Defects: Provides overview of common congenital heart defects for parents and caregivers
American Heart Association: Infective Endocarditis: Provides an overview of infective endocarditis, including summarizing prophylactic antibiotic use, for patients and caregivers


