


Allergic bronchopulmonary aspergillosis (ABPA) is a hypersensitivity reaction to Aspergillus species (generally A. fumigatus) that occurs almost exclusively in patients with asthma or, less commonly, cystic fibrosis. Immune responses to Aspergillus antigens cause airway obstruction and, if untreated, bronchiectasis and pulmonary fibrosis. Symptoms and signs are those of asthma with the addition of productive cough and, occasionally, fever and anorexia. Diagnosis is suspected based on history and imaging tests and confirmed by Aspergillus skin testing and measurement of IgE levels, circulating precipitins, and A. fumigatus
Allergic bronchopulmonary aspergillosis develops when airways of patients with asthma or cystic fibrosis become colonized with species of Aspergillus (ubiquitous fungi in the soil).
Pathophysiology
For unclear reasons, colonization in these patients prompts vigorous antibody (IgE and IgG) and cell-mediated immune responses (type I, III, and IV hypersensitivity reactions) to Aspergillus antigens, leading to frequent, recurrent asthma exacerbations. Over time, the immune reactions, combined with direct toxic effects of the fungus, lead to airway damage with dilation and, ultimately, bronchiectasis and fibrosis. The disorder is characterized histologically by mucoid impaction of airways, eosinophilic pneumonia, infiltration of alveolar septa with plasma and mononuclear cells, and an increase in the number of bronchiolar mucous glands and goblet cells.
Rarely, other fungi, such as Penicillium, Candida, Curvularia, Helminthosporium, and Drechslera, cause an identical syndrome called allergic bronchopulmonary mycosis in the absence of underlying asthma or cystic fibrosis.
Aspergillus is present intraluminally but is not invasive. Thus, ABPA must be distinguished from
Invasive aspergillosis, which occurs in immunocompromised patients
Aspergillomas, which are collections of Aspergillus in patients with established cavitary lesions or cystic airspaces
Aspergilluschronic obstructive pulmonary disease)
Although the distinction can be clear, overlap syndromes have been reported.
Symptoms and Signs
Symptoms are those of asthma or pulmonary cystic fibrosis exacerbation, with the addition of cough productive of dirty-green or brown plugs and, occasionally, hemoptysis. Fever, headache, and anorexia are common systemic symptoms in severe disease. Signs are those of airway obstruction, specifically, wheezing and prolonged expiration, which are indistinguishable from asthma exacerbation.
Diagnosis
History of asthma
Chest x-ray or high-resolution CT
Skin prick test with Aspergillus antigen
Aspergillus precipitins in blood
Positive sputum culture for Aspergillus species (or, rarely, other fungi)
IgE levels
Blood eosinophil count
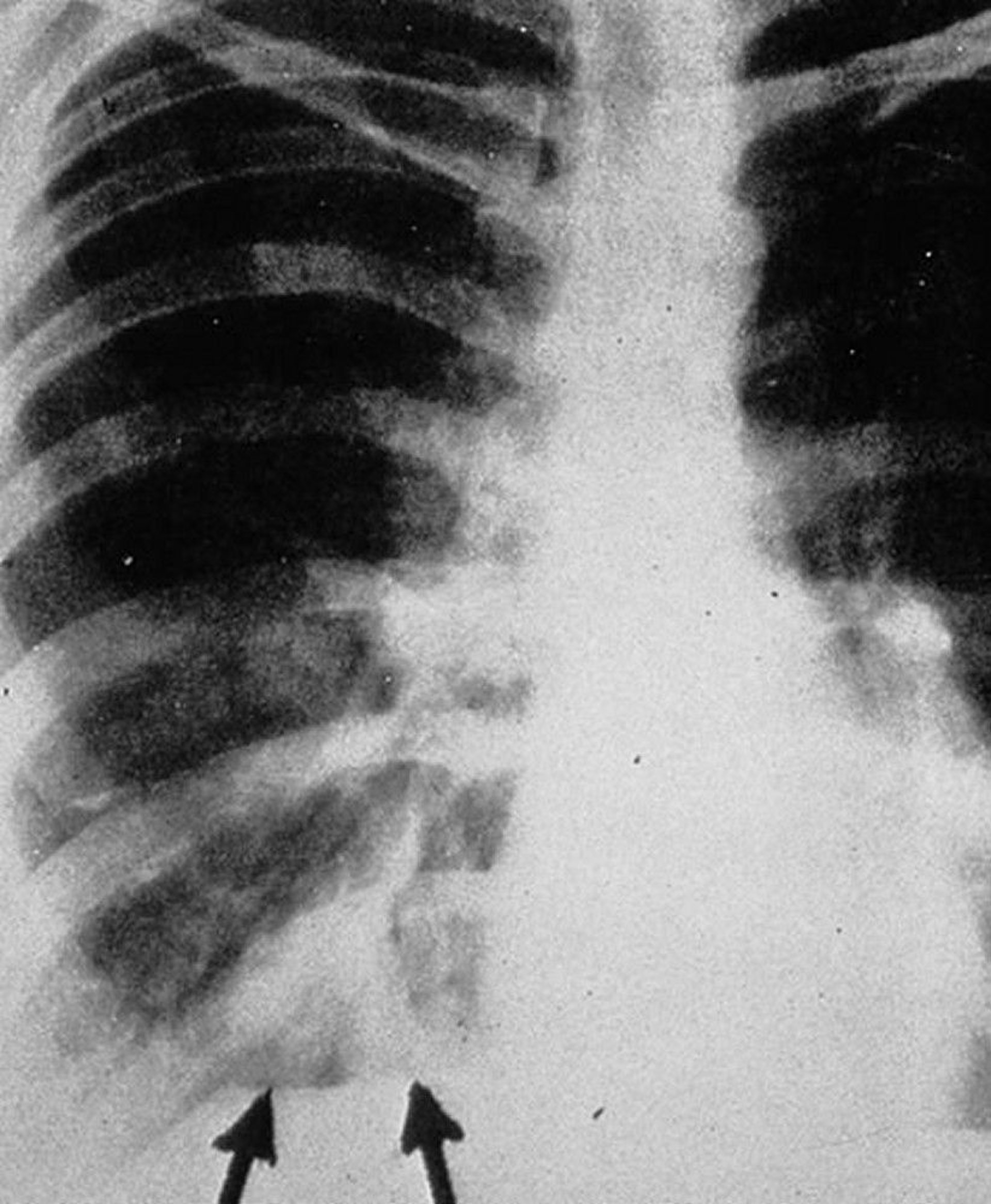
The diagnosis is suspected in patients with asthma or cystic fibrosis with recurrent exacerbations, migratory or nonresolving infiltrates on chest x-ray (often due to atelectasis resulting from mucoid plugging and bronchial obstruction), evidence of bronchiectasis on imaging studies, sputum cultures positive for A. fumigatus, or notable peripheral eosinophilia.

By permission of the publisher. From Groll A, Walsh T. In Atlas of Infectious Diseases: Fungal Infections. Edited by GL Mandell and RD Diamond. Philadelphia, Current Medicine, 2000.


By permission of the publisher. From Coakley R, Boucher R, Fiel S, et al. In Bone's Atlas of Pulmonary and Critical Care Medicine. Edited by J Crapo. Philadelphia, Current Medicine, 2005.
Several criteria have been proposed for the diagnosis (see table Diagnostic Criteria for Allergic Bronchopulmonary Aspergillosis), but in practice not all criteria are assessed in every case.
When the diagnosis is suspected, a skin prick test with Aspergillus antigen is the best first step, but serologic testing for Aspergillus precipitins may be a more practical initial test. An immediate wheal-and-flare reaction should prompt measurement of serum IgE and Aspergillus precipitins because up to 25% of patients with asthma without ABPA have a positive skin test. An IgE level > 1000 ng/mL (> 417 IU/mL) and positive precipitins suggest the diagnosis, which should be confirmed by measurement of specific anti-Aspergillus immunoglobulins (up to 10% of healthy patients have circulating precipitins). When ABPA is suspected, a finding of A. fumigatus–specific IgG and IgE antibodies in concentrations at least twice those found in patients without ABPA establishes the diagnosis.
Sputum and bronchoscopic cultures for Aspergillus have a low sensitivity and specificity for the diagnosis of ABPA and are not included as diagnostic criteria.
Whenever test results diverge, such as when serum IgE is elevated but no A. fumigatus–specific immunoglobulins are found, testing should be repeated and the patient should be monitored over time to definitively establish or exclude the diagnosis.
Diagnostic Criteria for Allergic Bronchopulmonary Aspergillosis
Essential criteria |
|
Other criteria |
|
* May be lower if patient meets all other criteria for diagnosis |
Adapted from Agarwal R, Chakrabarti A, Shah A, et al: Allergic bronchopulmonary aspergillosis: review of literature and proposal of new diagnostic and classification criteria. Clin Exp Allergy 43:850, 2013. |
Treatment
Sometimes antifungal drugs
Treatment is based on disease stage (see table Stages of Allergic Bronchopulmonary Aspergillosis).
≥ 50% decline in eosinophils, and 33% decline in IgE. Patients who achieve stage II disease require annual monitoring only.
Stages of Allergic Bronchopulmonary Aspergillosis*
Stage | Description | Criteria |
|---|---|---|
I | Acute | All diagnostic criteria present |
II | Remission | Symptoms resolved for > 6 months |
III | Relapse | Recurrence of ≥ 1 of the diagnostic criteria |
IV | Refractory | Corticosteroid-dependent or refractory to treatment |
V | Fibrosis | Diffuse fibrosis and bronchiectasis |
* Stages do not progress sequentially. | ||
All patients should be optimally treated for their underlying asthma or cystic fibrosis. In addition, patients taking long-term corticosteroids should be monitored for complications, such as cataracts, diabetes mellitus, and osteoporosis, and possibly prescribed treatments to prevent bone demineralization and Pneumocystis jirovecii lung infection.
Key Points
Consider allergic bronchopulmonary aspergillosis (ABPA) if a patient with asthma or cystic fibrosis develops frequent exacerbations for unclear reasons, has migratory or nonresolving infiltrates on chest x-ray, has evidence of bronchiectasis on imaging studies, has persistent blood eosinophilia, or if a sputum culture reveals Aspergillus.
Begin testing with a skin prick using Aspergillus antigen, followed usually by serologic testing.







