



Aspergillosis is an opportunistic infection that usually affects the lower respiratory tract and is caused by inhaling spores of the filamentous fungus Aspergillus, commonly present in the environment. The spores germinate and develop into hyphae, which enter blood vessels and, with invasive disease, cause hemorrhagic necrosis and infarction. Symptoms may be those of asthma, pneumonia, sinusitis, or rapidly progressing systemic illness. Diagnosis is based on imaging, histopathology, and specimen staining and culture. Treatment is with voriconazole, posaconazole, or isavuconazonium. A lipid formulation of amphotericin B is an alternative treatment. Fungus balls may require surgical resection.
Topic Resources

(See also Overview of Fungal Infections.)
Pathophysiology of Aspergillosis
Invasive infections are usually acquired by inhalation of spores or, occasionally, by direct invasion through damaged skin.
Major risk factors for aspergillosis include
Neutropenia when prolonged (typically > 7 days)
Long-term high-dose corticosteroid therapy
Organ transplantation (especially bone marrow transplantation with graft-vs-host disease [GVHD])
Hereditary disorders of neutrophil function (eg, chronic granulomatous disease)
Aspergillus species tend to infect open spaces, such as pulmonary cavities caused by previous lung disorders (eg, bronchiectasis, tumor, tuberculosis), the sinuses, or external auditory canals (otomycosis). Such infections tend to be locally invasive and destructive, although systemic spread sometimes occurs, particularly in patients who are immunocompromised with neutropenia or immunosuppression due to corticosteroid use. Aspergillosis can also occur in those with HIV infection/AIDS.
A. fumigatus is the most common cause of invasive pulmonary disease.
Allergic bronchopulmonary aspergillosis is a hypersensitivity reaction to A. fumigatus that results in lung inflammation unrelated to fungal invasion of tissues.
Focal infections, typically in the lung, sometimes form a fungus ball (aspergilloma), a characteristic growth of tangled masses of hyphae, with fibrin exudate and few inflammatory cells, typically encapsulated by fibrous tissue. Occasionally, there is some local invasion of tissue at the periphery of the cavity, but usually the fungus just resides within the cavity with no appreciable local invasion.
A chronic form of invasive aspergillosis occasionally occurs, particularly in patients taking corticosteroids long-term and those with chronic granulomatous disease, which is characterized by a hereditary phagocytic cell defect.
Aspergillus species can also cause endophthalmitis after trauma or surgery to the eye or by hematogenous seeding and can infect intravascular and intracardiac prostheses.
Primary superficial aspergillosis is uncommon but may occur in burns; beneath occlusive dressings; after corneal trauma (keratitis); or in the sinuses, mouth, nose, or ear canal.
Symptoms and Signs of Aspergillosis
Acute invasive pulmonary aspergillosis usually causes cough, often with hemoptysis, pleuritic chest pain, and shortness of breath. If untreated, invasive pulmonary aspergillosis may lead to rapidly progressive, ultimately fatal respiratory failure.
Chronic pulmonary aspergillosis may manifest with mild, indolent symptoms despite significant disease.
Extrapulmonary invasive aspergillosis occurs in patients who are severely immunocompromised. It begins with skin lesions, sinusitis, or pneumonia and may involve the liver, kidneys, brain, and other tissues via hematogenous dissemination; it is often rapidly fatal.
Aspergillosis in the sinuses can form an aspergilloma or cause allergic fungal sinusitis or a chronic, slowly invasive granulomatous inflammation with fever, rhinitis, and headache. Patients may have necrosing cutaneous lesions overlying the nose or sinuses, palatal or gingival ulcerations, signs of cavernous sinus thrombosis, or pulmonary or disseminated lesions.
Aspergillomas are usually asymptomatic but may cause mild cough and occasionally hemoptysis.
Diagnosis of Aspergillosis
Usually fungal culture and histopathology of tissue samples
Galactomannan antigen test on serum and/or bronchoalveolar lavage fluid
Because Aspergillus species are common in the environment, positive sputum cultures may be due to environmental contamination or noninvasive colonization in patients with chronic lung disease; positive cultures are significant mainly when sputum is obtained from patients with increased susceptibility due to immunosuppression or neutropenia or when there is high suspicion due to typical imaging findings (1). Conversely, sputum cultures from patients with aspergillomas or invasive pulmonary aspergillosis are often negative.
Chest x-rays are taken; however, chest CT is far more sensitive and should be done if patients are at high risk (ie, neutropenic). CT of sinuses is done if sinus infection is suspected. A movable fungus ball within a cavitary lesion is characteristic on both, although most lesions are focal and solid. Sometimes imaging detects a halo sign (a hazy shadow surrounding a nodule) or cavitation within a necrotic lesion. Diffuse, generalized pulmonary infiltrates are seen in some patients.

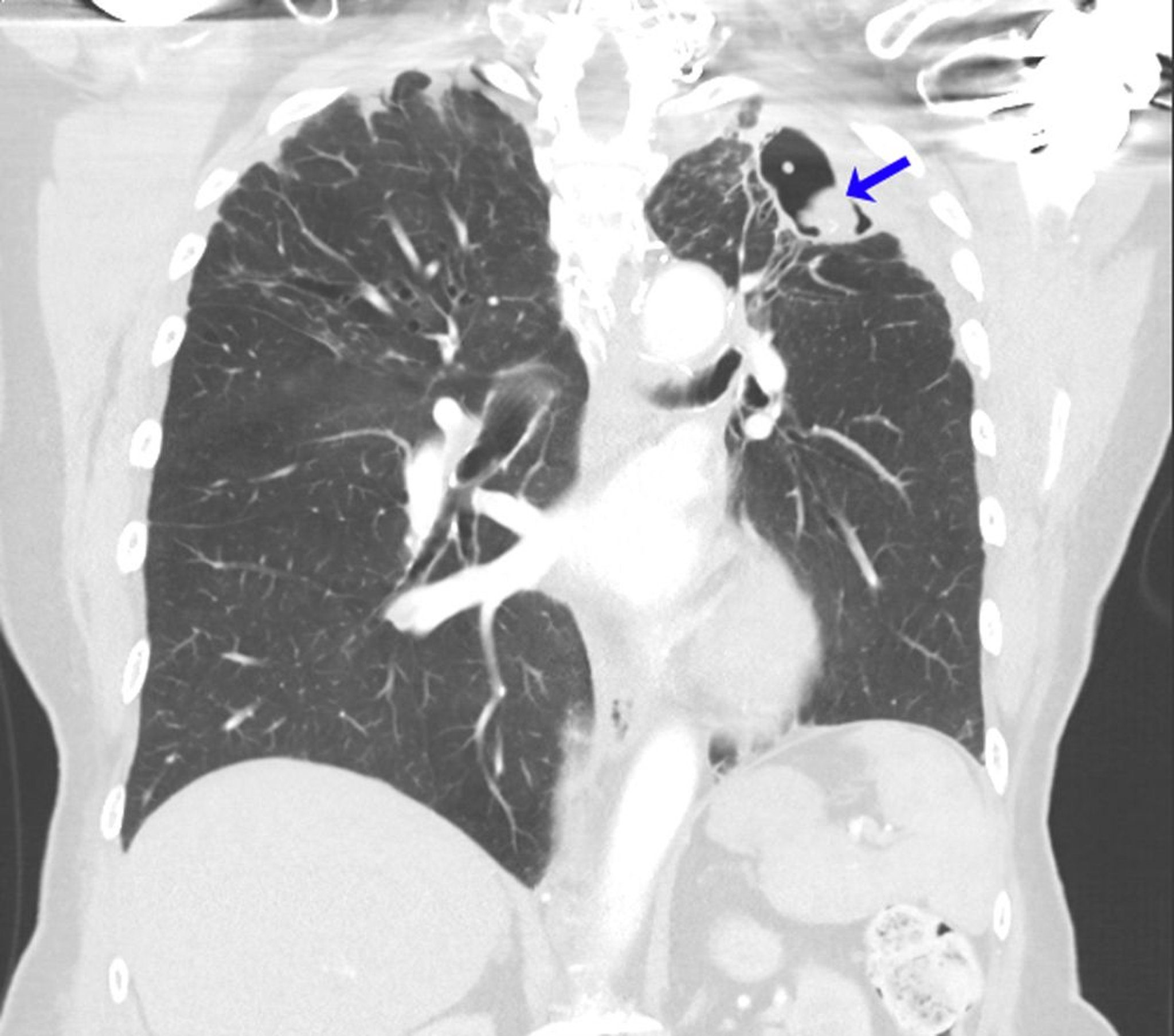
Image courtesy of Paschalis Vergidis, MD, MSc.
Culture and histopathology of a tissue sample are usually necessary for confirmation; histopathology helps distinguish invasive infection from colonization. The sample is typically taken from the lungs via bronchoscopy or percutaneous needle biopsy and from the sinuses via anterior rhinoscopy. Because cultures take time and histopathology results may be false-negative, most decisions to treat are based on strong presumptive clinical evidence. Blood cultures are almost always negative, even in rare cases of endocarditis. In Aspergillus endocarditis, large vegetations often release sizable emboli that may occlude blood vessels and provide specimens for diagnosis. Echocardiograms, especially transesophageal echocardiograms, can show a mobile intracardiac mass consistent with a vegetation despite negative blood cultures.
Serum Aspergillus galactomannan is specific but often not sufficiently sensitive to identify most cases in their early stages. In invasive pulmonary aspergillosis, the galactomannan test on bronchoalveolar lavage fluid is much more sensitive than that on serum and is often the only diagnostic option for patients with thrombocytopenia, for whom biopsy is contraindicated. Polymerase chain reaction (PCR) assays are available commercially.
Diagnosis reference
1. Patterson TF, Thompson GR 3rd, Denning DW, et al: Practice guidelines for the diagnosis and management of aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin Infect Dis 63(4):e1–e60, 2016. doi: 10.1093/cid/ciw326
Treatment of Aspergillosis
Voriconazole
Posaconazole
Isavuconazonium
Amphotericin B (including lipid formulations)
Echinocandins as salvage therapy
Sometimes surgery for aspergillomas
(See also Antifungal Medications).
Invasive infections usually require aggressive treatment with voriconazole (usually require aggressive treatment with voriconazole (1), posaconazole (), posaconazole (2), or isavuconazonium (), or isavuconazonium (3). Posaconazole and isavuconazonium have equal efficacy to and fewer adverse effects than voriconazole (2, 3). Amphotericin B (particularly lipid formulations) is also effective although more toxic (). Amphotericin B (particularly lipid formulations) is also effective although more toxic (4). Itraconazole (but not fluconazole) can be effective in some cases. Caspofungin or other echinocandins may be used as salvage therapy in combination with mold-active azole or ). Itraconazole (but not fluconazole) can be effective in some cases. Caspofungin or other echinocandins may be used as salvage therapy in combination with mold-active azole oramphotericin B. Combination therapy with voriconazole and echinocandins may be effective in certain patients.
Usually, treatment requires reversal of immunosuppression (eg, resolution of neutropenia, discontinuation of corticosteroids). Recrudescence is common if neutropenia recurs.
Aspergillomas neither require nor respond to systemic antifungal therapy but may require resection because of local effects, especially hemoptysis.
Prophylaxis with posaconazole or itraconazole can be considered for high-risk patients (those with graft-vs-host disease or neutropenia due to acute myelocytic leukemia).Prophylaxis with posaconazole or itraconazole can be considered for high-risk patients (those with graft-vs-host disease or neutropenia due to acute myelocytic leukemia).
Treatment references
1. Herbrecht R, Denning DW, Patterson TF, et al: Voriconazole versus amphotericin B for primary treatment of invasive aspergillosis. N Engl J Med 347(6):408–415, 2002. doi: 10.1056/NEJMoa020191
2. Maertens JA, Rahav G, Lee DG, et al: Posaconazole versus voriconazole for primary treatment of invasive aspergillosis: A phase 3, randomised, controlled, non-inferiority trial. Lancet 397(10273):499–509, 2021. doi: 10.1016/S0140-6736(21)00219-1. Clarification and additional information. Lancet 398(10299):490, 2021.
3. Maertens JA, Raad II, Marr KA, et al: Isavuconazole versus voriconazole for primary treatment of invasive mould disease caused by Aspergillus and other filamentous fungi (SECURE): A phase 3, randomised-controlled, non-inferiority trial. Lancet 387(10020):760–769, 2016. doi: 10.1016/S0140-6736(15)01159-9
4. Patterson TF, Thompson GR 3rd, Denning DW, et al: Practice guidelines for the diagnosis and management of aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin Infect Dis 63(4):e1–e60, 2016. doi: 10.1093/cid/ciw326
Key Points
Inhaling spores of the mold Aspergillus can cause localized or invasive pulmonary disease and, rarely, disseminated infection (eg, to the brain) in patients who are severely immunocompromised.
Invasive aspergillosis is more common among patients who are immunocompromised with neutropenia or immunosuppression due to corticosteroid use, but it can also occur in those with HIV infection/AIDS.
Culture and histopathology of a tissue sample are usually necessary, but the galactomannan test on bronchoalveolar lavage fluid can help diagnose pulmonary infection.
Treat invasive infections with voriconazole, posaconazole or isavuconazonium; amphotericin B is an alternative.Treat invasive infections with voriconazole, posaconazole or isavuconazonium; amphotericin B is an alternative.
Aspergillomas neither require nor respond to antifungals, but consider surgical resection if they cause bleeding or other symptoms.
More Information
The following English-language resource may be useful. Please note that THE MANUAL is not responsible for the content of this resource.
Infectious Diseases Society of America: Practice Guidelines for the Diagnosis and Management of Aspergillus (2016)







