



Subarachnoid hemorrhage is sudden bleeding into the subarachnoid space. The most common cause of spontaneous bleeding is a ruptured aneurysm. Symptoms include sudden, severe headache, usually with loss or impairment of consciousness. Secondary vasospasm (causing focal brain ischemia), meningismus, seizures, and hydrocephalus (causing persistent headache and obtundation) are common. Diagnosis is by CT or MRI; if neuroimaging is normal, diagnosis is by cerebrospinal fluid analysis to look for xanthochromia and red blood cells. Treatment is with supportive measures and neurosurgery or endovascular measures, preferably in a comprehensive stroke center.

")

Etiology of Subarachnoid Hemorrhage
Subarachnoid hemorrhage is bleeding between the arachnoid and pia mater.
In general, head trauma is the most common cause of subarachnoid hemorrhage, but traumatic subarachnoid hemorrhage is usually considered a separate disorder. Spontaneous (primary) subarachnoid hemorrhage usually results from ruptured aneurysms. A congenital intracranial saccular or berry aneurysm is the cause in about 85% of patients. Bleeding may stop spontaneously. Aneurysmal hemorrhage may occur at any age but is most common from age 40 to 65.
Less common causes are mycotic aneurysms, arteriovenous malformations, and bleeding disorders.
Pathophysiology of Subarachnoid Hemorrhage
Blood in the subarachnoid space causes a chemical meningitis that commonly increases intracranial pressure for days or a few weeks. Secondary vasospasm may cause focal brain ischemia; about 25% of patients develop signs of a transient ischemic attack (TIA) or ischemic stroke. Brain edema is maximal and risk of vasospasm and subsequent infarction (called angry brain) is highest between 72 hours and 10 days. Secondary acute hydrocephalus is also common. A 2nd rupture (rebleeding) sometimes occurs, most often within about 7 days.
Symptoms and Signs of Subarachnoid Hemorrhage
Headache is usually severe, peaking within seconds. Patients often describe it as "the worst headache in their life." Loss of consciousness may follow, usually immediately but sometimes not for several hours. Severe neurologic deficits may develop and become irreversible within minutes or a few hours. Sensorium may be impaired, and patients may become restless. Seizures are possible.
Usually, the neck is not stiff initially unless the cerebellar tonsils herniate. However, within 24 hours, chemical meningitis causes moderate to marked meningismus, vomiting, and sometimes bilateral extensor plantar responses. Heart or respiratory rate is often abnormal.
Fever, continued headaches, and confusion are common during the first 5 to 10 days. Secondary hydrocephalus may cause headache, obtundation, and motor deficits that persist for weeks. Rebleeding may cause recurrent or new symptoms.
Diagnosis of Subarachnoid Hemorrhage
Usually noncontrast CT and, if negative, lumbar puncture
Diagnosis of subarachnoid hemorrhage is suggested by characteristic symptoms. Testing should proceed as rapidly as possible, before damage becomes irreversible.
Noncontrast CT is done within 6 hours of symptom onset. When done within this time frame, this test has very high sensitivity. Therefore, if this test does not detect a subarachnoid hemorrhage, no other testing is needed as long as patients have a normal physical examination, no meningeal signs, and no anemia, MRI is comparably sensitive but less likely to be immediately available. False-negative results occur if volume of blood is small or if the patient is so anemic that blood is isodense with brain tissue.
If subarachnoid hemorrhage is suspected clinically but not identified by neuroimaging or if neuroimaging is not immediately available, lumbar puncture is done. Lumbar puncture is contraindicated if increased intracranial pressure is suspected because the sudden decrease in cerebrospinal (CSF) pressure may lessen the tamponade of a clot on the ruptured aneurysm, causing further bleeding.
Pearls & Pitfalls
|

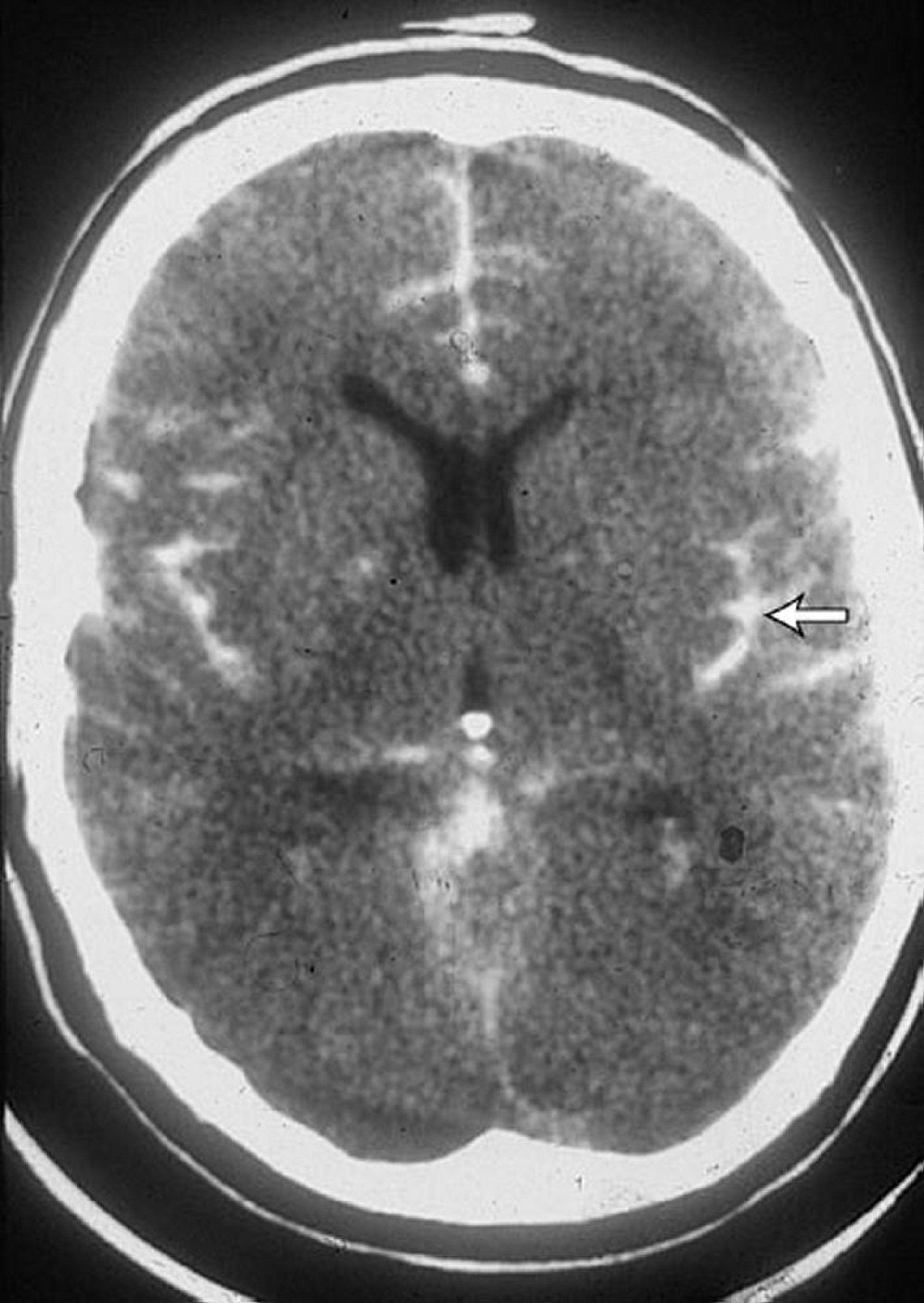
By permission of the publisher. From Lenaerts M, Couch J. In Atlas of Clinical Neurology. Edited by RN Rosenberg. Philadelphia, Current Medicine, 2002.
CSF findings suggesting subarachnoid hemorrhage include
Numerous red blood cells (RBCs)
Xanthochromia
Increased pressure
RBCs in CSF may also be caused by traumatic lumbar puncture. Traumatic lumbar puncture is suspected if the RBC count decreases in tubes of CSF drawn sequentially during the same lumbar puncture. About 6 hours or more after a subarachnoid hemorrhage, RBCs become crenated and lyse, resulting in a xanthochromic CSF supernatant and visible crenated RBCs (noted during microscopic CSF examination); these findings usually indicate that subarachnoid hemorrhage preceded the lumbar puncture. If there is still doubt, hemorrhage should be assumed, or the lumbar puncture should be repeated in 8 to 12 hours.
In patients with subarachnoid hemorrhage, conventional cerebral angiography is done as soon as possible after the initial bleeding episode; alternatives include magnetic resonance angiography and CT angiography. All 4 arteries (2 carotid and 2 vertebral arteries) should be injected because up to 20% of patients (mostly women) have multiple aneurysms.
On ECG, subarachnoid hemorrhage may cause ST-segment elevation or depression. It can cause syncope, mimicking myocardial infarction. Other possible ECG abnormalities include prolongation of the QRS or QT intervals and peaking or deep, symmetric inversion of T waves.

Treatment of Subarachnoid Hemorrhage
Treatment in a comprehensive stroke center
Nicardipine if mean arterial pressure is Nicardipine if mean arterial pressure is> 130 mm Hg
Nimodipine to prevent vasospasm Nimodipine to prevent vasospasm
Occlusion of causative aneurysms
Patients with subarachnoid hemorrhage should be treated in a comprehensive stroke center whenever possible.
Bed rest is mandatory. Restlessness and headache are treated symptomatically. Stool softeners are given to prevent constipation, which can lead to straining.
Hypertension should be treated only if mean arterial pressure is > 130 mm Hg or systolic blood pressure (BP) is > 160 mm Hg; euvolemia is maintained, and IV nicardipine is titrated as for 130 mm Hg or systolic blood pressure (BP) is > 160 mm Hg; euvolemia is maintained, and IV nicardipine is titrated as forintracerebral hemorrhage (1).
Anticoagulants and antiplatelet medications are contraindicated.
Vasospasm is prevented by giving nimodipine 60 mg orally every 4 hours for 21 days to prevent vasospasm, but BP needs to be maintained in the desirable range (usually considered to be a mean arterial pressure of 70 to 130 mm Hg and a systolic pressure of 120 to 185 mm Hg).is prevented by giving nimodipine 60 mg orally every 4 hours for 21 days to prevent vasospasm, but BP needs to be maintained in the desirable range (usually considered to be a mean arterial pressure of 70 to 130 mm Hg and a systolic pressure of 120 to 185 mm Hg).
If clinical signs of acute hydrocephalus occur, ventricular drainage should be considered.
Aneurysms are occluded to reduce risk of rebleeding. Detachable endovascular coils can be inserted during angiography to occlude the aneurysm. Alternatively, if the aneurysm is accessible, surgery to clip or stent the aneurysm can be done, especially for patients with an evacuable hematoma or acute hydrocephalus. If patients are arousable, most vascular neurosurgeons operate within the first 24 hours to minimize risk of rebleeding and risks due to angry brain. If > 24 hours have elapsed, some neurosurgeons delay surgery until 10 days have passed; this approach decreases risks due to angry brain but increases risk of rebleeding and overall mortality.
Treatment reference
1. Greenberg SM, Ziai WC, Cordonnier C, et al: 2022 Guideline for the management of patients with spontaneous intracerebral hemorrhage: A guideline from the American Heart Association/American Stroke Association. Stroke 53 (7):e282–e361, 2022. doi: 10.1161/STR.0000000000000407 Epub 2022 May 17.
Prognosis for Subarachnoid Hemorrhage
About 35% of patients die after the first aneurysmal subarachnoid hemorrhage; another 15% die within a few weeks because of a subsequent rupture (1). After 6 months, a 2nd rupture occurs at a rate of about 3%/year. In general, prognosis is grave with an aneurysm, better with an arteriovenous malformation, and best when 4-vessel angiography does not detect a lesion, presumably because the bleeding source is small and has sealed itself. Among survivors, neurologic damage is common, even when treatment is optimal.
Prognosis reference
1. Nieuwkamp DJ, Setz LE, Algra A, et al: Changes in case fatality of aneurysmal subarachnoid haemorrhage over time, according to age, sex, and region: A meta-analysis. Lancet Neurol 8 (7):635–642, 2019. doi: 10.1016/S1474-4422(09)70126-7 Epub 2009 Jun 6.
Key Points
Possible complications after subarachnoid hemorrhage include chemical meningitis, vasospasm, hydrocephalus, rebleeding, seizures, and brain edema.
Suspect subarachnoid hemorrhage if headache is severe at onset and reaches peak intensity within seconds or causes loss of consciousness.
If subarachnoid hemorrhage is confirmed, image both carotid and both vertebral arteries using conventional cerebral angiography, magnetic resonance angiography, or CT angiography because many patients have multiple aneurysms.
If possible, send patients to a comprehensive stroke center for treatment.







