



- Overview of Neuro-ophthalmologic and Cranial Nerve Disorders
- Conjugate Gaze Palsies
- Internuclear Ophthalmoplegia
- Third Cranial (Oculomotor) Nerve Disorders
- Fourth Cranial (Trochlear) Nerve Palsy
- Sixth Cranial (Abducens) Nerve Palsy
- Trigeminal Neuralgia
- Hemifacial Spasm
- Facial Nerve Palsy
- Glossopharyngeal Neuralgia
Trigeminal neuralgia is severe paroxysmal, lancinating facial pain due to a disorder of the 5th cranial nerve. Diagnosis is clinical. Treatment is usually with carbamazepine or gabapentin; sometimes surgery is required.Trigeminal neuralgia is severe paroxysmal, lancinating facial pain due to a disorder of the 5th cranial nerve. Diagnosis is clinical. Treatment is usually with carbamazepine or gabapentin; sometimes surgery is required.
Topic Resources

(See also Overview of Neuro-ophthalmologic and Cranial Nerve Disorders.)
Trigeminal neuralgia affects mainly adults, especially older people. It is more common among women.
Etiology of Trigeminal Neuralgia
Trigeminal neuralgia is usually caused by
Compression of the trigeminal nerve at its root by an aberrant loop of an intracranial artery (eg, anterior inferior cerebellar artery, ectatic basilar artery)
Less often, a venous loop that compresses the 5th cranial (trigeminal) nerve at its root entry zone into the brain stem
Other less common causes include compression by a tumor, an arteriovenous malformation, an aneurysm, and occasionally a multiple sclerosis plaque at the root entry zone (usually in younger patients), but these causes are usually distinguished by accompanying sensory loss and other deficits.
Other disorders that cause similar symptoms (eg, multiple sclerosis) are sometimes considered to be trigeminal neuralgia and sometimes not. Recognizing the cause is what is important.
The mechanism is unclear. One theory suggests that nerve compression causes local demyelination, which may result in ectopic impulse generation (ephaptic transmission) and/or disinhibition of central pain pathways involving the spinal trigeminal nucleus.
Symptoms and Signs of Trigeminal Neuralgia
Pain due to trigeminal neuralgia occurs along the distribution of one or more sensory divisions of the trigeminal nerve, most often the maxillary. The pain is paroxysmal, lasting seconds up to 2 minutes, but attacks may recur rapidly—as often as 100 times a day. It is lancinating, excruciating, and sometimes incapacitating.
Pain is often precipitated by stimulating a facial trigger point (eg, by chewing, brushing the teeth, or smiling). Sleeping on that side of the face is often intolerable.
Usually, only one side of the face is affected.
Diagnosis of Trigeminal Neuralgia
Clinical evaluation
Symptoms of trigeminal neuralgia are often pathognomonic. Thus, some other disorders that cause facial pain can be differentiated clinically:
Chronic paroxysmal hemicrania is differentiated by longer (5 to 8 minutes) attacks of pain and its dramatic response to indomethacin.Chronic paroxysmal hemicrania is differentiated by longer (5 to 8 minutes) attacks of pain and its dramatic response to indomethacin.
Postherpetic pain is differentiated by its constant duration (without paroxysms), typical antecedent rash, scarring, and predilection for the ophthalmic division.
Migraine, which may cause atypical facial pain, is differentiated by pain that is more prolonged and often throbbing.
Sinusitis and odontogenic pain, which can usually be differentiated by their associated findings (eg, nasal discharge, fever, positional headache, tooth sensitivity)
Neurologic examination is normal in trigeminal neuralgia. Thus, neurologic deficits (usually loss of facial sensation) suggest that the trigeminal neuralgia–like pain is caused by another disorder (eg, tumor, stroke, multiple sclerosis plaque, vascular malformation, other lesions that compress the trigeminal nerve or disrupt its brain stem pathways). In such cases, MRI is indicated.
Treatment of Trigeminal Neuralgia
Usually antiseizure drugs
Trigeminal neuralgia is treated with carbamazepine 200 mg orally 3 or 4 times a day, which is usually effective for long periods; it is begun at 100 mg orally twice a day, increasing the dose by 100 to 200 mg/day until pain is controlled (maximum daily dose 1200 mg).Trigeminal neuralgia is treated with carbamazepine 200 mg orally 3 or 4 times a day, which is usually effective for long periods; it is begun at 100 mg orally twice a day, increasing the dose by 100 to 200 mg/day until pain is controlled (maximum daily dose 1200 mg).
If carbamazepine is ineffective or has adverse effects, one of the following oral drugs may be tried:If carbamazepine is ineffective or has adverse effects, one of the following oral drugs may be tried:
OxcarbazepineOxcarbazepine
Lamotrigine Lamotrigine
Gabapentin Gabapentin
BaclofenBaclofen
PhenytoinPhenytoin
AmitriptylineAmitriptyline
Peripheral nerve block provides temporary relief. Botulinum toxin may be injected between the epidermis and the dermis at trigger points where pain is experienced or along the path of the nerve branches involved. This treatment may be beneficial, but data are limited.
If pain is severe despite these measures, neuroablative treatments are considered; however, efficacy may be temporary, and improvement may be followed by recurrent pain that is more severe than the preceding episodes. Surgery that relieves pain may result in facial numbness. Painful numbness (anesthesia dolorosa) may also result; it occurs in 4% of patients after rhizotomy.
In a posterior fossa craniectomy, a small pad can be placed to separate the pulsating vascular loop from the trigeminal root (called microvascular decompression, or the Jannetta procedure). In gamma knife radiosurgery, gamma radiation is focused on the proximal trigeminal nerve where it exits the brain stem; this procedure interrupts pain signals to the brain. Electrolytic or chemical lesions or balloon compression of the trigeminal (gasserian) ganglion can be made via a percutaneous stereotactically positioned needle. Occasionally, the trigeminal nerve fibers between the gasserian ganglion and brain stem are cut.
Sometimes, as a last resort to relieve intractable pain, the trigeminal nerve is destroyed.
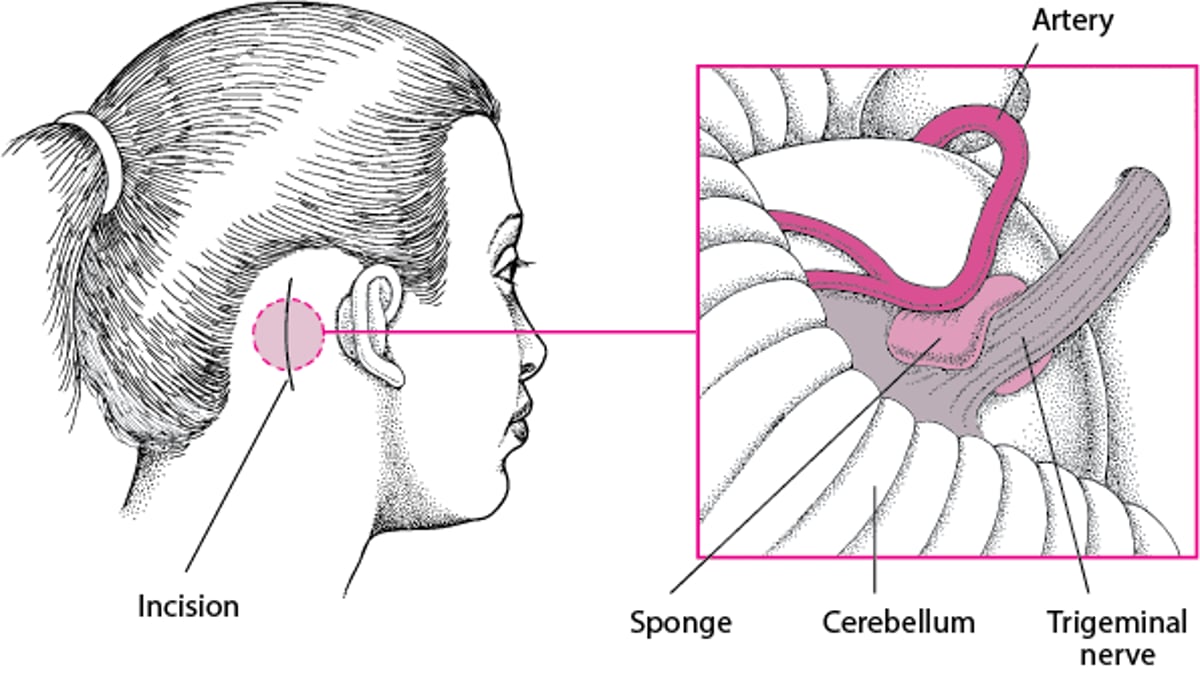
Microvascular Decompression
Microvascular decompression can relieve pain due to vascular compression of the affected cranial nerve in trigeminal neuralgia, hemifacial spasms, or glossopharyngeal neuralgia. For trigeminal neuralgia, pressure is relieved by placing a sponge is placed between the 5th cranial (trigeminal) nerve and the compressing artery (Jannetta procedure). Usually, this procedure relieves the pain, but in about 15% of patients, pain recurs. |

Key Points
Trigeminal neuralgia is usually caused by compression by an intracranial artery.
The characteristic paroxysmal, lancinating, excruciating, and sometimes incapacitating pain is often pathognomonic.
Treat with carbamazepine, which is usually effective for long periods; if carbamazepine is ineffective or has adverse effects, try another drug (eg, oxcarbazepine, lamotrigine, gabapentin, baclofen, pregabalin).Treat with carbamazepine, which is usually effective for long periods; if carbamazepine is ineffective or has adverse effects, try another drug (eg, oxcarbazepine, lamotrigine, gabapentin, baclofen, pregabalin).
If severe pain persists despite these measures, consider microvascular decompression or neuroablative treatments; however, efficacy may be temporary, and improvement may be followed by recurrent pain that is more severe than the preceding episodes.







