


In shoulder (glenohumeral) dislocations, the humeral head separates from the glenoid fossa; displacement is usually anterior.
Shoulder dislocations account for about half of major joint dislocations.
Shoulder dislocations may be
Anterior
Posterior
Inferior
(See Overview of Dislocations.)
Anterior Shoulder Dislocations
Shoulder dislocations are anterior in ≥ 95% of patients; the mechanism is abduction and external rotation. Associated injuries can include
Brachial plexus injuries
Rotator cuff tears (particularly in older patients)
Fracture of the greater tuberosity
Axillary nerve injury
Shoulder instability and thus recurrent dislocation are common in patients > 30 years old.
The acromion is prominent, and the elbow is held slightly out from the side in abduction. The humeral head is displaced anteriorly and inferiorly and cannot be palpated in its usual position. Patients are unwilling to move the arm. They may have motor and sensory deficits (eg, if the axillary nerve is injured, decreased sensation over the deltoid).
Diagnosis of Anterior Shoulder Dislocations
True anteroposterior and axillary x-rays


By permission of the publisher. From Jacobs P: Current Orthopedic Diagnosis and Treatment. Edited by JD Heckman, RC Schenck, and A Agarwal. Philadelphia, Current Medicine, 2002.
True anteroposterior (AP) and axillary x-rays are diagnostic for anterior dislocations, showing the humeral head outside the glenoid fossa.
Treatment of Anterior Shoulder Dislocations
Usually closed reduction
Treatment of anterior shoulder dislocations is usually closed reduction using local anesthesia (intra-articular injection) or procedural sedation (see also Overview of Shoulder Dislocation Reduction Techniques). Commonly used techniques include
External rotation (eg, Hennepin technique)
Scapular manipulation
Cunningham (massage) technique
Davos (autoreduction) technique
Stimson (dangling weights) technique
FARES (fast, reliable, and safe) technique
Many techniques (eg, Hennepin, scapular manipulation, Cunningham, FARES) can often be done without sedation, but they require time for muscles affected by spasm to adequately relax; patients must be able to focus their attention on relaxation.
No one technique is best for all shoulder dislocations. The patient's position at presentation, if possible, is one factor in choosing a technique. The following should also be taken into account:
If the patient's arm cannot be adducted, the Cunningham technique or external rotation should not be used because both maneuvers depend on arm adduction.
If the patient's arm is fixed in abduction, the FARES technique, the Stimson technique, or scapular manipulation should be used.
If the patient's arm is inferiorly dislocated, traction-countertraction should be used.
If the patient is pregnant and cannot lie flat on her stomach, the Stimson technique should not be used.
After reduction, the joint is immobilized immediately with a sling and swathe (see figure Sling and swathe). In patients age > 40 years, sling and swathe for 5 to 7 days and encourage early range of motion to help prevent complications (eg, frozen shoulder).
Sling and Swathe


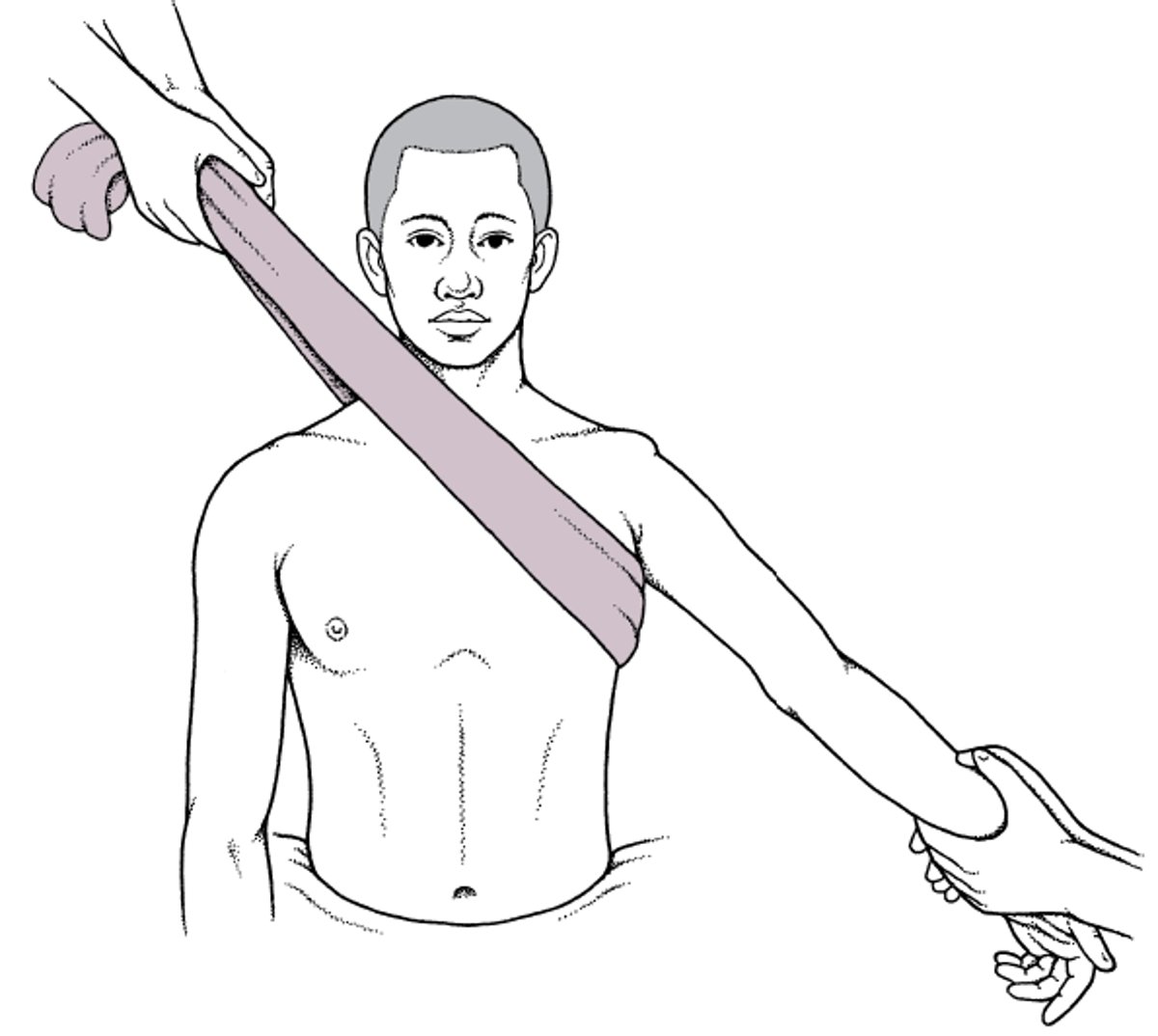
The traction-countertraction technique can be used to reduce anterior shoulder dislocations (see figure Traction-countertraction technique for reducing anterior shoulder dislocations). For this procedure, the patient lies on a stretcher, and its wheels are locked. One practitioner pulls on a folded sheet wrapped around the patient’s chest. Another practitioner pulls the affected limb down and laterally 45°. After the humerus is free, slight lateral traction on the upper humerus may be needed. (See also How To Reduce Anterior Shoulder Dislocations Using Traction-Countertraction.)
Traction-countertraction technique for reducing anterior shoulder dislocations
The patient lies on a stretcher, and its wheels are locked. One practitioner pulls on a folded sheet wrapped around the patient’s chest. Another practitioner pulls the affected limb down and laterally 45°. After the humerus is free, slight lateral traction on the upper humerus may be needed. |

Hennepin technique (external rotation) can be done with the patient supine or seated (see figure Hennepin technique for reducing anterior shoulder dislocations). The dislocated arm is adducted with the elbow held at 90°. The arm is then externally rotated slowly (eg, over 5 to 10 minutes) to allow time for muscle spasms to resolve. Reduction commonly occurs at 70 to 110° of external rotation. This technique is effective in about 80 to 90% of cases. (See also How To Reduce Anterior Shoulder Dislocations Using External Rotation.)
Hennepin technique for reducing anterior shoulder dislocations
The practitioner adducts the dislocated arm with the elbow held at 90°. The arm is then externally rotated slowly (eg, over 5 to 10 min) to allow time for muscle spasms to resolve. Reduction commonly occurs at 70 to 110° of external rotation. |


Scapular manipulation can be done with the patient upright or prone. The practitioner flexes the patient's elbow 90° and slowly externally rotates the arm. An assistant applies gentle traction on the arm. The practitioner then rotates the scapula so that the inferior tip moves medially, toward the spine. Scapular manipulation can be used with other techniques (eg, Stimson technique). (See also How To Reduce Anterior Shoulder Dislocations Using Scapular Manipulation.)
The Cunningham technique involves massage of the muscles around the glenohumeral joint while the patient is sitting. The practitioner does the following:
Sits facing and just to the side of the patient
Puts the patient’s hand on the practitioner's shoulder, keeping the patient's elbow flexed and adducted
Puts the practitioner's hand in the depression in the bend of the patient's elbow (antecubital fossa) and holds the dislocated arm in place
Massages the biceps, mid-deltoid, and trapezius to relax muscle spasms
Instructs the patient to try to relax rather than tense up if the shoulder feels as if it is moving (relaxation is crucial to reduction using this technique)
Instructs the patient to sit up straight (no slouching forward or to the side) and to shrug the shoulders back, trying to make the upper ends of the right and left scapula touch each other
The shoulder slips back into place within minutes.
The Davos (autoreduction) technique is a patient-controlled technique used to reduce anterior dislocations; it should be done without procedural sedation (1). The patient sits with the ipsilateral knee flexed and elbows close to the thigh. The hands are clasped together in front of the leg and tied together and to the proximal tibia with an elastic band so that the patient does not have to concentrate on maintaining the correct position for the maneuver and can relax the muscles. The practitioner sits on the patient's foot and instructs the patient to lean the head back (neck extension) and shrug the shoulders. Extending the neck exerts constant traction on the dislocated shoulder. Thus, patients can use their own weight to reduce the dislocation. (See also How To Reduce Anterior Shoulder Dislocations Using the Davos Technique.)
The Stimson technique (also called the dangling weights technique) is done less commonly. It is done with the patient prone and the affected extremity hanging over the side of a bed. Weights are attached to the patient's wrist. After about 30 minutes, the muscle spasm usually relaxes enough to allow the humeral head to reduce. Because the patient is prone, conscious sedation is not recommended. This position may be too uncomfortable for pregnant patients and extremely obese patients. This technique can also be used with scapular manipulation; the practitioner applies scapular manipulation while the patient is prone. This approach shortens the time needed for the shoulder to relocate. (See also How To Reduce Anterior Shoulder Dislocations Using the Stimson Technique.)
The FARES technique is usually done without sedation (2). The patient lies in the supine position with the elbow extended and the forearm in neutral rotation. The practitioner applies traction and slowly abducts the arm, moving the arm vertically between about 5 cm above and below the horizontal plane in an oscillating pattern at a rate of 2 or 3 full cycles/second. This movement aids in muscle relaxation. Once the arm is abducted to 90°, the patient's palm is turned up, the arm is externally rotated, and the vertical oscillations are continued as the arm is continually abducted. Reduction usually occurs at about 120° abduction. (See also How To Reduce Anterior Shoulder Dislocations Using the FARES Method.)

© Elsevier Inc. All Rights Reserved.
This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.

© Elsevier Inc. All Rights Reserved.
This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.

© Elsevier Inc. All Rights Reserved.
This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.

© Elsevier Inc. All Rights Reserved.
This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.


© Elsevier Inc. All Rights Reserved.
This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.


© Elsevier Inc. All Rights Reserved.
This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.

© Elsevier Inc. All Rights Reserved.
This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.

© Elsevier Inc. All Rights Reserved.
This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.

© Elsevier Inc. All Rights Reserved.
This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.


© Elsevier Inc. All Rights Reserved.
This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.
Treatment references
1. Stafylakis D, Abrassart S, Hoffmeyer P: Reducing a shoulder dislocation without sweating: The Davos technique and its results: Evaluation of a nontraumatic, safe, and simple technique for reducing anterior shoulder dislocations. J Emerg Med 50 (4):656–659, 2016. doi: 10.1016/j.jemermed.2016.01.020
2. Sayegh FE, Kenanidis EI, Papavasiliou KA, et al: Reduction of acute anterior dislocations: A prospective randomized study comparing a new technique with the Hippocratic and Kocher methods. J Bone Joint Surg Am 91 (12): 2775–2782, 2009. https://doi.org/10.2106/JBJS.H.01434
Key Points
Most shoulder dislocations are anterior; the acromion is prominent, and the elbow is held slightly out from the side in abduction.
Diagnose based on true anteroposterior and axillary x-rays, which show the humeral head outside the glenoid fossa (a Y-view x-ray is useful to diagnose a posterior dislocation).
Reduce using a technique based partly on the patient's position at presentation; other factors should also be considered.
Some techniques require sedation, and some (eg, Hennepin, scapular manipulation, Cunningham, FARES) can often be done without sedation, but they require time for the affected muscles to adequately relax.
After reduction, immobilize the joint immediately with a sling and swathe.
Posterior Shoulder Dislocations
Occasionally, dislocations are posterior—a commonly missed injury (see table Examination for Some Commonly Missed Injuries). It is classically caused by seizures, electric shock, or electroconvulsive therapy done without muscle relaxants.
Pearls & Pitfalls
|
Deformity may not be obvious. The arm is held adducted and internally rotated. Typically, when the elbow is flexed, passive external rotation is impossible. If such rotation is impossible, an anteroposterior (AP) shoulder x-ray should be taken. If it shows no obvious fracture or dislocation, posterior shoulder dislocation should be considered. A clue to the diagnosis on the AP view is the light bulb or ice cream cone sign; the humeral head is internally rotated, and the tuberosities do not project laterally, making the humeral head appear circular.
Bony injuries occur in about 65% of posterior dislocations (1).
The axillary view or trans-scapular Y view is diagnostic. A posterior dislocation cannot be excluded without a Y view.


In the left image (anteroposterior view), the humeral head is internally rotated, resulting in the light bulb or ice cream cone sign (projections of the greater and lesser humeral tuberosities are not seen), which suggests a posterior dislocation. In the right image (Y view), the humeral head is posterior to the glenoid fossa, which demonstrates a posterior dislocation.
Image courtesy of Danielle Campagne, MD.


In the Y view, lines drawn through the acromion (blue arrow), coracoid (black arrow), and scapular body (red arrow) intersect at the center of the glenoid fossa. In this x-ray, the humeral head is outside of and posterior to the glenoid fossa, indicating a posterior dislocation.
Image courtesy of Danielle Campagne, MD.
In the left image (anteroposterior view), the humeral head is internally rotated, resulting in the light bulb or ice cream cone sign (projections of the greater and lesser humeral tuberosities are not seen), which suggests a posterior dislocation. In the right image (Y view), the humeral head is posterior to the glenoid fossa, which demonstrates a posterior dislocation.
Image courtesy of Danielle Campagne, MD.
In the Y view, lines drawn through the acromion (blue arrow), coracoid (black arrow), and scapular body (red arrow) intersect at the center of the glenoid fossa. In this x-ray, the humeral head is outside of and posterior to the glenoid fossa, indicating a posterior dislocation.
Image courtesy of Danielle Campagne, MD.
Reduction is often possible using longitudinal traction (as with the traction-countertraction technique). (See also How To Reduce Posterior Shoulder Dislocations.)

Reference
1. Rouleau DM, Hebert-Davies J: Incidence of associated injury in posterior shoulder dislocation: systematic review of the literature. J Orthop Trauma 26(4):246-51, 2012. doi: 10.1097/BOT.0b013e3182243909
Inferior Shoulder Dislocations
Inferior dislocations (luxatio erecta) are rare and usually clinically obvious; patients hold their arm over their head (ie, abducted to almost 180°), usually with the forearm resting on the head. The arm is shortened; the humeral head is often palpable in the axilla. The joint capsule is disrupted, and the rotator cuff may be torn. The brachial artery is injured in < 5% of cases. The axillary nerve or another nerve is usually damaged, but deficits often resolve after reduction.
X-rays are diagnostic.

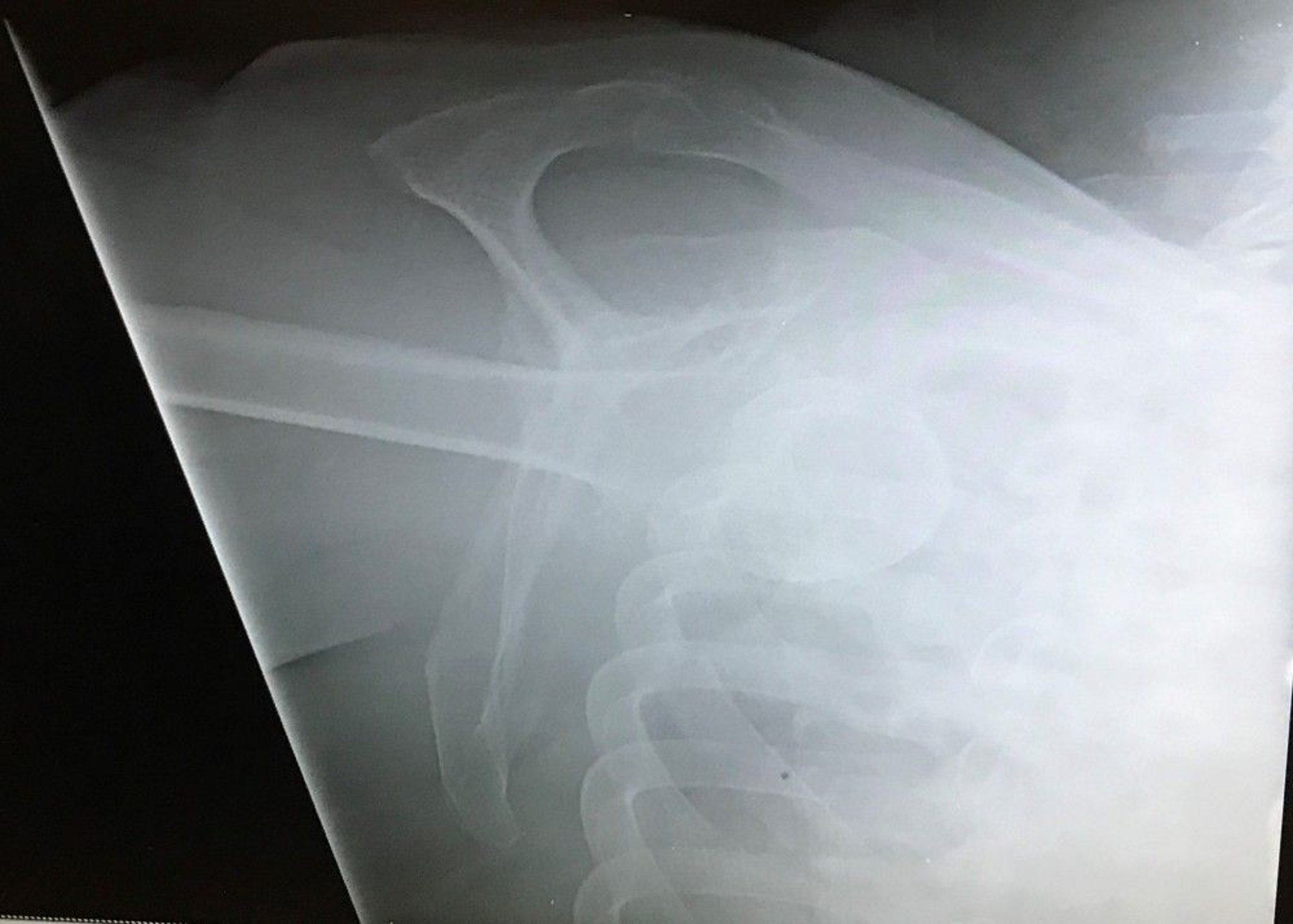
Image courtesy of Danielle Campagne, MD.
Reduction is done using traction-countertraction of the abducted arm. Closed reduction is usually successful unless there is a buttonhole deformity (humeral head is trapped in a tear of the inferior capsule); in such cases, open reduction is required.







