



- Angiostrongyliasis
- Anisakiasis
- Ascariasis
- Baylisascariasis
- Dracunculiasis
- Hookworm Infection
- Pinworm Infestation
- Strongyloidiasis
- Toxocariasis
- Trichinosis
- Trichuriasis
- Overview of Filarial Nematode Infections
- Bancroftian Lymphatic Filariasis and Brugian Lymphatic Filariasis
- Dirofilariasis
- Loiasis
- Mansonellosis
- Onchocerciasis (River Blindness)
Anisakiasis is infection with larvae of nematodes (worms) of the Anisakis simplex complex and the other anisakid species, Pseudoterranova decipiens complex and Contracecum osculatum complex. Infection is acquired by eating raw or undercooked saltwater fish or squid; larvae burrow into the mucosa of the gastrointestinal (GI) tract, causing abdominal pain and sometimes vomiting. Endoscopy is used for diagnosis (visualization of larvae or biopsy) and treatment (removal of larvae).
Topic Resources

Anisakis is a parasite that resides in the gastrointestinal (GI) tract of marine mammals. Excreted eggs hatch into free-swimming larvae, which are ingested by fish and squid (intermediate hosts). Human infection is acquired when raw or undercooked foods infested with intermediate hosts (eg, as sashimi, ceviche, or pickled/marinated seafood) are eaten and the larvae burrow into the stomach and small intestine. Raw seafood that is frozen using appropriate procedures (eg, commercial sushi in the United States) that kill anisakid larvae is safe for human consumption.
Anisakiasis infections occur globally. Japan, Spain, South Korea, Italy, and the United States have the highest rates of reported cases (1).

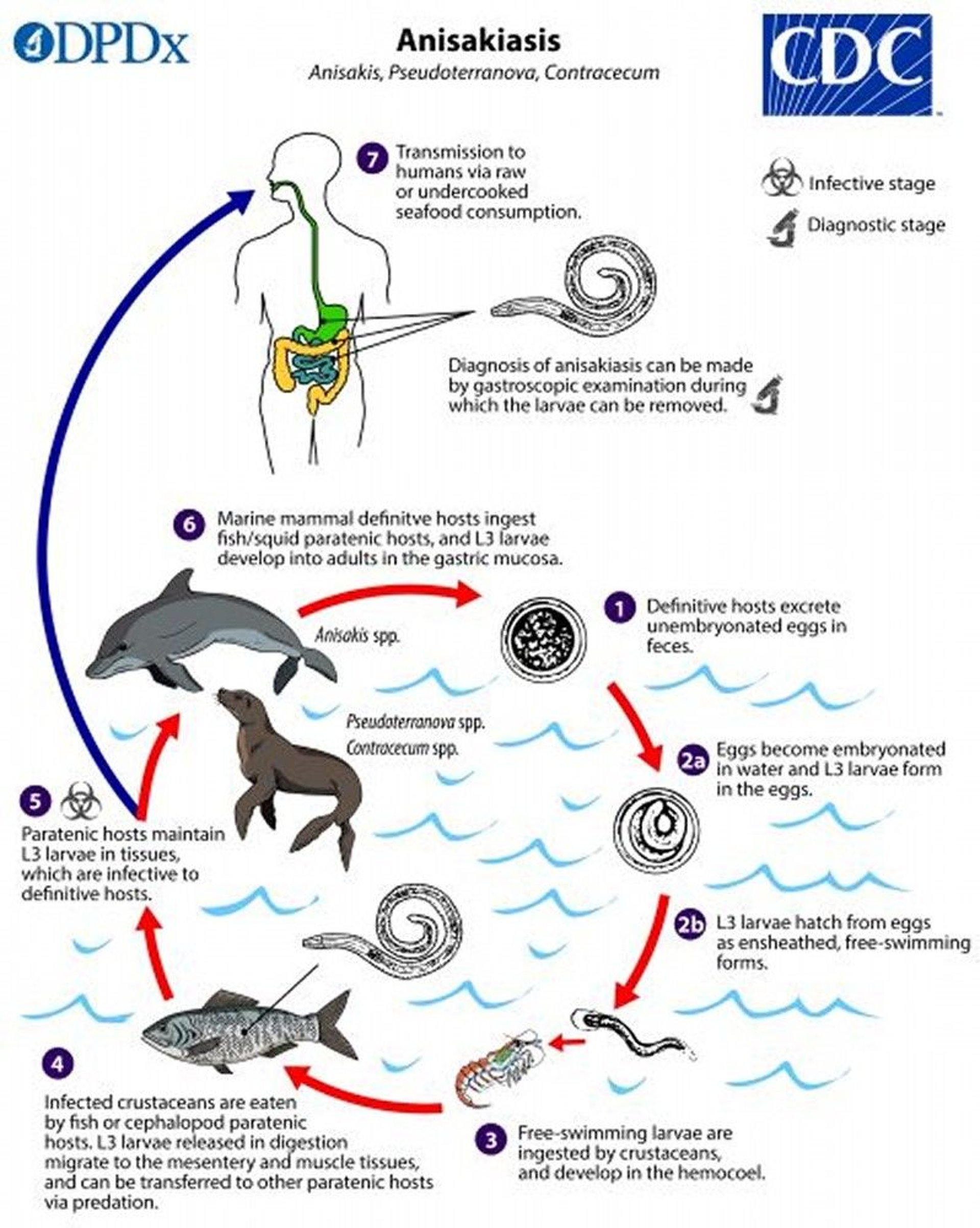
Image from the Centers of Disease Control and Prevention, Global Health, Division of Parasitic Diseases and Malaria.
(See also Approach to Parasitic Infections.)
Reference
1. Shamsi S, Barton DP. A critical review of anisakidosis cases occurring globally. Parasitol Res. 2023;122(8):1733-1745. doi:10.1007/s00436-023-07881-9
Symptoms and Signs of Anisakiasis
Symptoms of gastric anisakiasis typically include abdominal pain, nausea, and vomiting within hours of ingesting the larvae. Occasionally, the larvae are expelled into the mouth by coughing.
Involvement of the small intestine is less common and may result in an inflammatory mass and subacute symptoms resembling Crohn disease or appendicitis that develop 1 to 2 weeks later.
Ectopic infections outside the lumen of the gastrointestinal tract may rarely occur.
Anisakiasis typically resolves spontaneously after several weeks because larvae are unable to survive for long periods of time in a human host; rarely, it persists for months.
Diagnosis of Anisakiasis
Upper endoscopy
Histopathologic examination of endoscopic or surgical biopsies
Anisakiasis can be diagnosed by gross visualization of the larvae with upper endoscopy. Diagnosis can also be made by histopathologic examination of endoscopic or surgical biopsies. Sometimes, patients expel larvae by coughing and bring them in for analysis.
Serologic testing is available in some countries.
Stool examination is unhelpful.
Treatment of Anisakiasis
Endoscopic removal of the larvae
Possibly albendazole
Endoscopic removal of the larvae is curative.
Treatment of presumptive anisakiasis with albendazole 400 mg orally twice a day for 6 to 21 days may be effective, but data are limited (Treatment of presumptive anisakiasis with albendazole 400 mg orally twice a day for 6 to 21 days may be effective, but data are limited (1, 2).
Treatment references
1. Pacios E, Arias-Diaz J, Zuloaga J, Gonzalez-Armengol J, Villarroel P, Balibrea JL. Albendazole for the treatment of anisakiasis ileus. Clin Infect Dis. 2005;41(12):1825-1826. doi:10.1086/498309
2. Moore DA, Girdwood RW, Chiodini PL. Treatment of anisakiasis with albendazole. Lancet. 2002;360(9326):54. doi:10.1016/s0140-6736(02)09333-9
Prevention of Anisakiasis
Proper freezing procedures are required to kill anisakid larvae in raw or undercooked seafood (eg, sushi).
Anisakis larvae are destroyed in seafood by
Cooking to > 63° C (> 145° F)
Freezing at −20° C (−4° F) or below for 7 days
Freezing at −35° C (−31° F) or below until solid, then storing at that temperature for ≥ 15 hours, or at −20° C (−4° F ) for 24 hours
Pickling, salting, and smoking do not reliably kill anisakid larvae.
Key Points
Humans acquire Anisakis when they consume the intermediate hosts (fish or squid) that are raw or undercooked; thus, anisakiasis is common in areas where raw seafood is consumed.
Gastric anisakiasis typically causes abdominal pain, nausea, and vomiting within hours of ingesting the larvae; an inflammatory mass may form in the small intestine and symptoms may resemble Crohn disease or appendicitis.
Anisakiasis typically resolves spontaneously after several weeks.
Do upper endoscopy to diagnose anisakiasis by visualizing the larvae or histopathologic examination of biopsy tissue.
Endoscopic removal of the larvae is curative.
Proper freezing procedures prevent anisakiasis in sushi.







