



- Overview of Glomerular Disorders
- Overview of Nephritic Syndrome
- Alport Syndrome
- Immunoglobulin A Nephropathy
- Postinfectious Glomerulonephritis (PIGN)
- Rapidly Progressive Glomerulonephritis (RPGN)
- Thin Basement Membrane Disease
- Overview of Nephrotic Syndrome
- Congenital Nephrotic Syndromes
- Diabetic Nephropathy
- Focal Segmental Glomerulosclerosis
- HIV-Associated Nephropathy
- Membranous Nephropathy
- Minimal Change Disease
- Fibrillary and Immunotactoid Glomerulopathies
- Lupus Nephritis
- Membranoproliferative Glomerulonephritis
Membranoproliferative glomerulonephritis (MPGN) is characterized by a pattern of glomerular injury on light microscopy, including hypercellularity and thickening of the glomerular basement membrane. The clinical presentation usually consists of mixed nephritic and nephrotic features. Cause is idiopathic or secondary to another disorder. Diagnosis is by renal biopsy. Treatment is directed at the underlying disorder, when present. For patients with idiopathic disease, treatment may be supportive or include corticosteroids and other immunosuppressive agents.





(See also Overview of Nephrotic Syndrome.)
Membranoproliferative glomerulonephritis (MPGN) is characterized histologically by glomerular basement membrane (GBM) thickening and proliferative changes on light microscopy.
The preferred classification is based on pathophysiologic processes and informed by findings on immunofluorescence microscopy (1). This classification scheme broadly divides MPGN into
Immunoglobulin/immune complex–mediated MPGN
Complement-mediated MPGN
MPGN without immunoglobulin or complement deposition
An underlying (secondary) cause is present in the majority of cases regardless of type. Idiopathic (primary) cases are less common and usually observed within the immunoglobulin/immune complex–mediated category.
Primary forms affect children, particularly between 2 and 15 years of age (2), and account for < 10% of cases of nephrotic syndrome in children (3); secondary forms tend to affect adults. Familial cases suggest genetic factors play a role in at least some cases. Many factors contribute to hypocomplementemia.

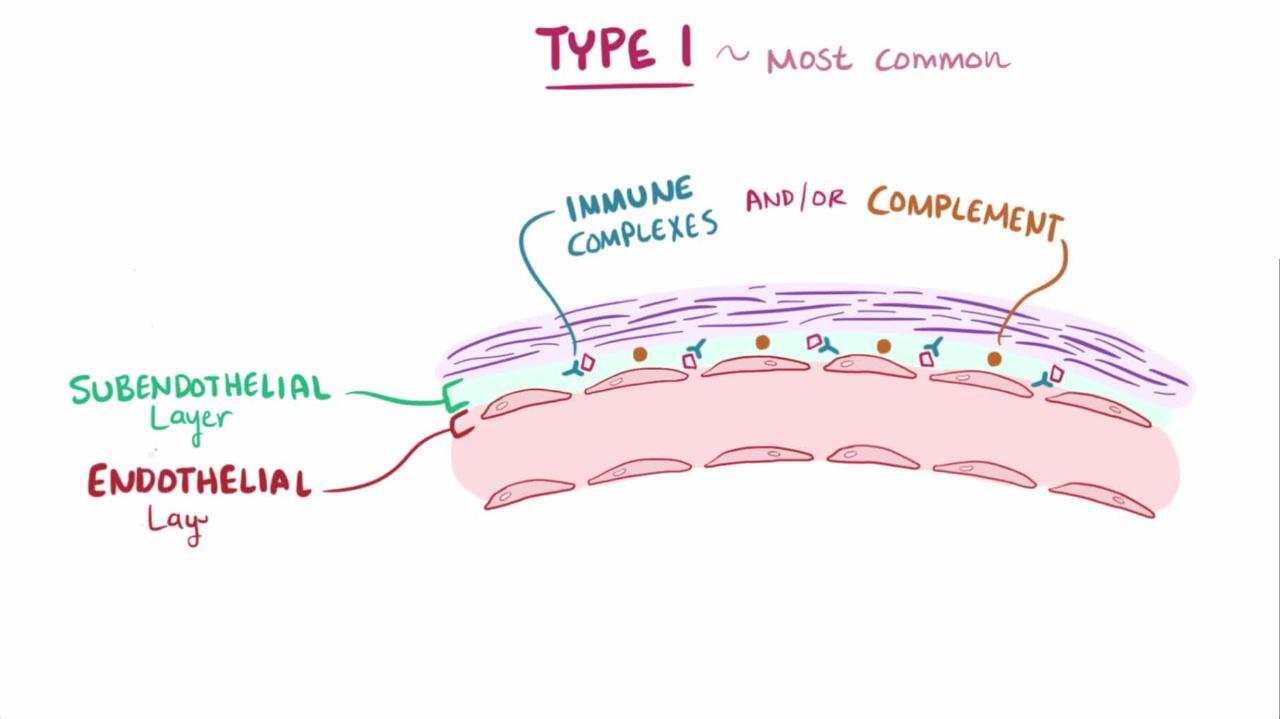
Immunoglobulin/immune complex–mediated MPGN
Immunoglobulin/immune complex–mediated MPGN is due to chronic antigenemia and/or circulating immune complexes and most commonly occurs secondary to one of the following:
Systemic immune complex disorder (eg, systemic lupus erythematosus, mixed connective tissue disease, Sjögren syndrome, rheumatoid arthritis)
Chronic infection (eg, bacterial endocarditis, HIV infection, hepatitis B or C infection, visceral abscess, ventriculoatrial shunt infection, protozoa infection)
Monoclonal gammopathies (eg, monoclonal gammopathy of unknown significant (MGUS), chronic lymphocytic leukemia, lymphomas, multiple myeloma)
Immunofluorescence microscopy findings may suggest certain underlying diseases.

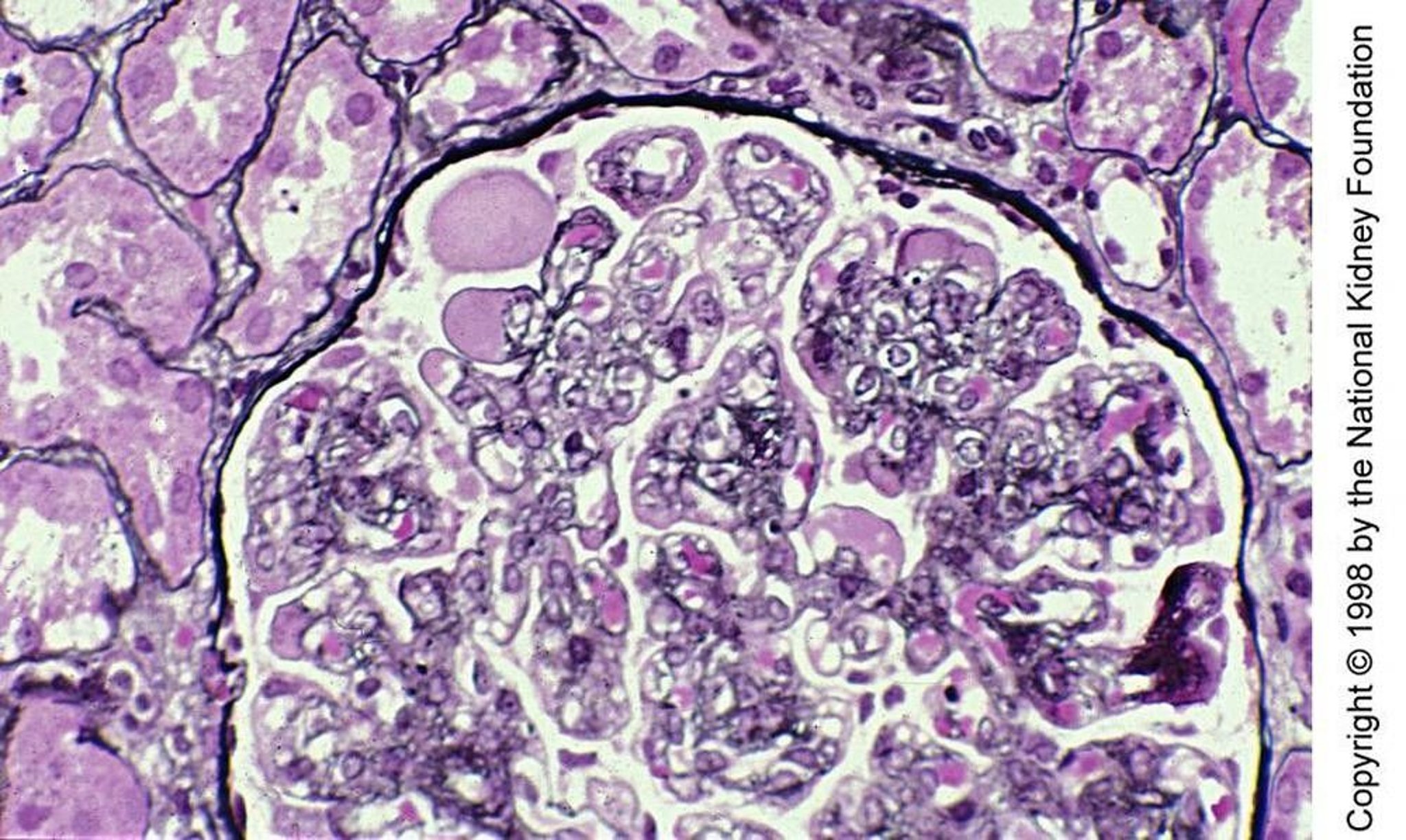
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
Complement-mediated MPGN

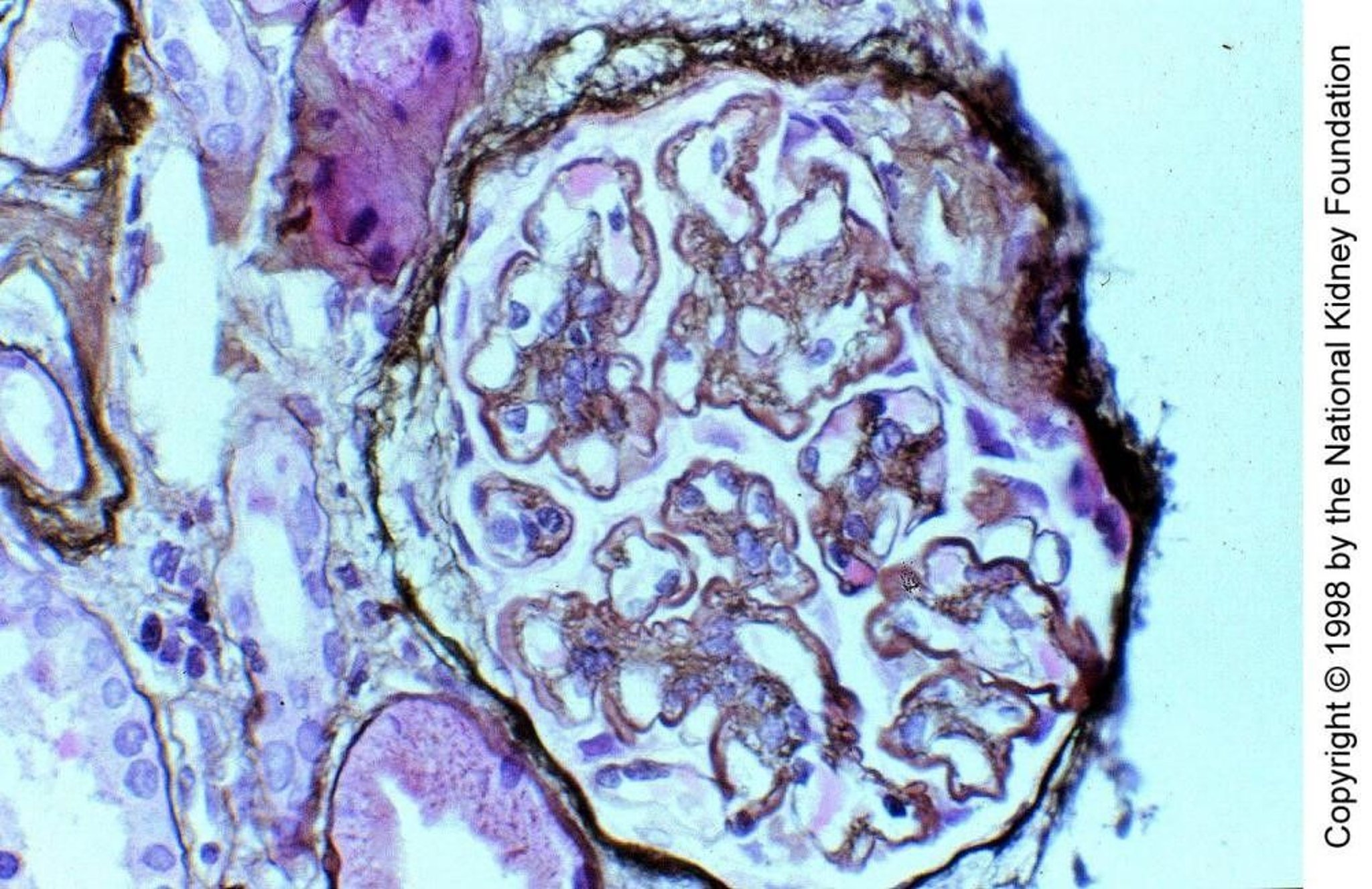
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
Complement-mediated MPGN is less common than immunuglobulin/immune complex–mediated MPGN. It is caused by dysregulation and persistent activation of the alternative complement pathway, and there is deposition of complement products along the capillary walls and in the mesangium. Complement-mediated MPGN can be further categorized based on features observed on immunofluorescence and electron microscopy as C3 or C4 glomerulonephritis or dense deposition disease (DDD).
Membranoproliferative pattern MPGN without immunoglobulin or complement deposition
MPGN without immunoglobulin or complement deposition may occur in:
Healing phase of thrombotic microangiopathies (eg, thrombotic thrombocytopenia purpura,hemolytic-uremic syndrome)
POEMS syndrome (polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, skin changes)
Radiation nephritis
Nephropathy associated with bone marrow transplantation
Drug-associated thrombotic microangiopathies
Disfibrinogenemia and other prothrombotic states
Histology suggests endothelial injury and reparative changes. Immunofluorescence microscopy does not show significant immunoglobulin or complement deposition, and electron microscopy does not show electron-dense deposits along the capillary walls.
General references
1. Kidney Disease: Improving Global Outcomes (KDIGO) Glomerular Diseases Work Group. KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases. Kidney Int 2021;100(4S):S1-S276. doi:10.1016/j.kint.2021.05.021
2. Wong EKS, Marchbank KJ, Lomax-Browne H, et al. C3 Glomerulopathy and Related Disorders in Children: Etiology-Phenotype Correlation and Outcomes. Clin J Am Soc Nephrol 2021;16(11):1639-1651. doi:10.2215/CJN.00320121
3. Coppo R, Gianoglio B, Porcellini MG, Maringhini S. Frequency of renal diseases and clinical indications for renal biopsy in children (report of the Italian National Registry of Renal Biopsies in Children). Group of Renal Immunopathology of the Italian Society of Pediatric Nephrology and Group of Renal Immunopathology of the Italian Society of Nephrology. Nephrol Dial Transplant 1998;13(2):293-297. doi:10.1093/oxfordjournals.ndt.a027821
Symptoms and Signs of Membranoproliferative Glomerulonephritis
Symptoms and signs are similar to those for other types of glomerulonephritis. The urine sediment may reveal hematuria (with dysmorphic red cells and/or red cell casts). The degree of proteinuria is variable. The serum creatinine may be normal or elevated.
Patients with dense deposition disease, a subtype of complement-mediated MPGN, have a greater incidence of ocular abnormalities (basal laminar drusen, diffuse retinal pigment alterations, diskiform macular detachment, choroidal neovascularization), which ultimately impair vision (1).
Symptoms and signs reference
1. Appel GB, Cook HT, Hageman G, et al. Membranoproliferative glomerulonephritis type II (dense deposit disease): an update. J Am Soc Nephrol 2005;16(5):1392-1403. doi:10.1681/ASN.2005010078
Diagnosis of Membranoproliferative Glomerulonephritis
Renal biopsy
Serum complement profile
Specific laboratory tests based on the classification of the membranoproliferative lesion and associated underlying disorders
Diagnosis is confirmed by renal biopsy. The pattern of immunoglobulin and complement deposition on immunofluorescence microscopy helps classify the type of MPGN lesion. Additional tests are also performed to help identify the underlying cause of the MPGN lesion.
Hypocomplementemia is more frequently present in all types of MPGN than in other glomerular disorders and provides supportive evidence of the diagnosis (see table Serum Complement Profiles in Membranoproliferative Glomerulonephritis). In immunoglobulin/immune complex–mediated MPGN, the classic complement pathway is activated; C3 is normal or mildly decreased, and C4 is typically decreased. In complement-mediated MPGN, the alternate complement pathway is activated; C3 is decreased, but C4 is normal. In MPGN without immunoglobulin complement deposition, C3 and C4 are normal.
Serum Complement Profiles in Membranoproliferative Glomerulonephritis
Classification Based on Immunofluorescence Microscopy | Complement Profile |
|---|---|
Immunoglobulin/immune complex–mediated MPGN | Classic complement pathway activated C3: Normal or mildly decreased C4: Decreased |
Complement-mediated MPGN | Alternate complement pathway activated C3: Decreased C4: Normal |
MPGN without immunoglobulin or complement deposition | C3: Normal C4: Normal |
Specific laboratory testing for secondary causes is based on their associations with the types of MPGN.
Complete blood count (CBC), often obtained in the course of diagnostic evaluation, demonstrates normochromic-normocytic anemia, often out of proportion to the stage of chronic kidney disease (possibly because of hemolysis), and thrombocytopenia from platelet consumption.
Treatment of Membranoproliferative Glomerulonephritis
For adults, renin-angiotensin system inhibition, and/or immunosuppressive therapy
Corticosteroids for children with nephrotic-range proteinuria
Kidney transplantation for patients with kidney failure
Underlying disorders are treated when possible. Patients with mild disease (ie, normal kidney function and non–nephrotic-range proteinuria or significant hematuria) are typically treated with angiotensin-converting enzyme (ACE) inhibitors or angiotensin II receptor blockers (ARBs). Additional immunosuppressive therapy is typically not indicated in such patients.
Among patients with nephrotic-range proteinuria (≥ 3 g/day) and normal kidney function, treatment with corticosteroids (eg, prednisone for 1 year, followed by tapering to maintenance therapy) may stabilize kidney function. However, corticosteroid treatment may retard growth in children and cause 3 g/day) and normal kidney function, treatment with corticosteroids (eg, prednisone for 1 year, followed by tapering to maintenance therapy) may stabilize kidney function. However, corticosteroid treatment may retard growth in children and causehypertension. Calcineurin inhibitors (eg, cyclosporine, tacrolimus) may be used as alternatives for patients who do not tolerate or wish to receive corticosteroids. Patients who present with rapidly progressive crescentic MPGN should be treated more aggressively with corticosteroids plus cyclophosphamide (. Calcineurin inhibitors (eg, cyclosporine, tacrolimus) may be used as alternatives for patients who do not tolerate or wish to receive corticosteroids. Patients who present with rapidly progressive crescentic MPGN should be treated more aggressively with corticosteroids plus cyclophosphamide (1). Kidney transplantation may be necessary in kidney failure.
Other general supportive measures include dietary and sodium restriction, antihypertensive therapy, renin-angiotensin inhibition, and treatment of dyslipidemia.
Treatment reference
1. Kidney Disease: Improving Global Outcomes (KDIGO) Glomerular Diseases Work Group. KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases. Kidney Int 2021;100(4S):S1-S276. doi:10.1016/j.kint.2021.05.021
Prognosis for Membranoproliferative Glomerulonephritis
Prognosis varies based on histopathologic classification, and whether the disease is primary or has a treatable secondary cause (1).
Prognosis reference
1. Noris M, Daina E, Remuzzi G. Membranoproliferative glomerulonephritis: no longer the same disease and may need very different treatment. Nephrol Dial Transplant 2023;38(2):283-290. doi:10.1093/ndt/gfab281
Key Points
Membranoproliferative glomerulonephritis (MPGN) is a pattern of glomerular injury with characteristic findings on light microscopy, including hypercellularity and thickening of the glomerular basement membrane.
Patients most often present with nephrotic syndrome, but they may present with nephritic syndrome.
Confirm the diagnosis with renal biopsy and obtain serum complement (C3, C4) and additional tests to classify MPGN as immune complex/monoclonal immunoglobulin-mediated MPGN, complement-mediated MPGN, or MPGN without immunoglobulin or complement deposition.
Test for underlying diseases based on clinical presentation and specific type of MPGN.
Treat nephrotic-range proteinuria with corticosteroids and consider immunosuppressants depending upon progression of kidney dysfunction; target additional therapy at any specific underlying disease.







