


Crohn disease is a chronic transmural inflammatory bowel disease that usually affects the distal ileum and colon but may occur in any part of the gastrointestinal tract. Symptoms include diarrhea and abdominal pain. Abscesses, internal and external fistulas, and bowel obstruction may arise. Extraintestinal symptoms, particularly arthritis, may occur. Diagnosis is by colonoscopy and imaging studies. Treatment is with 5-aminosalicylic acid, corticosteroids, immunomodulators, anticytokines, antibiotics, and often surgery.
(See also Overview of Inflammatory Bowel Disease.)
Pathophysiology of Crohn Disease
Crohn disease begins with crypt inflammation and abscesses, which progress to tiny focal aphthoid ulcers. These mucosal lesions may develop into deep longitudinal and transverse ulcers with intervening mucosal edema, creating a characteristic cobblestoned appearance to the bowel.
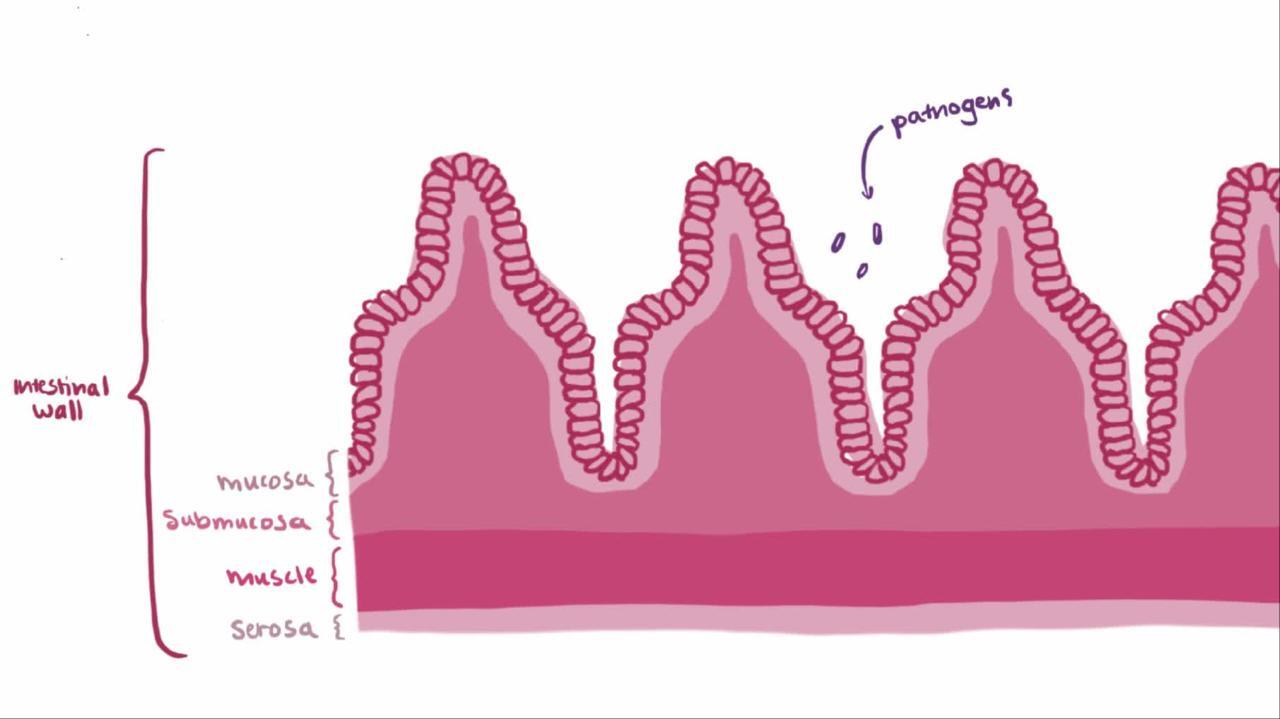
Transmural spread of inflammation leads to lymphedema and thickening of the bowel wall and mesentery. Mesenteric fat typically extends onto the serosal surface of the bowel. Mesenteric lymph nodes often enlarge. Extensive inflammation may result in hypertrophy of the muscularis mucosae, fibrosis, and stricture formation, which can lead to bowel obstruction.
Abscesses are common, and fistulas often penetrate into adjoining structures, including other loops of bowel, the bladder, or psoas muscle. Fistulas may even extend to the skin of the anterior abdomen or flanks. Independently of intra-abdominal disease activity, perianal fistulas and abscesses occur in 25 to 33% of cases; these complications are frequently the most troublesome aspects of Crohn disease.
Noncaseating granulomas can occur in lymph nodes, peritoneum, the liver, and all layers of the bowel wall. Although pathognomonic when present, granulomas are not detected in about half of patients with Crohn disease. The presence of granulomas does not seem to be related to the clinical course.
Segments of diseased bowel are sharply demarcated from adjacent normal bowel (called skip areas), hence the name regional enteritis (1):
About 30% of Crohn disease cases involve the ileum alone (ileitis).
About 40% involve the ileum and colon (ileocolitis), with a predilection for the right side of the colon.
About 30% involve the colon alone (granulomatous colitis), most of which, unlike ulcerative colitis, spares the rectum.


Occasionally, the small bowel is involved (jejunoileitis). The stomach, duodenum, or esophagus is clinically involved only rarely, although microscopic evidence of disease is often detectable in the gastric antrum, especially in younger patients. In the absence of surgical intervention, the disease almost never extends into areas of small bowel that are not involved at first diagnosis.
Classification
Crohn disease is categorized into 3 principal patterns: (1) primarily inflammatory, which after several years commonly evolves into (2) primarily stenotic or obstructing or (3) primarily penetrating or fistulizing.
These different clinical patterns dictate different therapeutic approaches. Some genetic studies suggest a molecular basis for this classification.
Complications
There is an increased risk of cancer in affected small-bowel segments. Patients with colonic involvement have a long-term risk of colorectal cancer equal to that of ulcerative colitis, given the same extent and duration of disease.
Chronic malabsorption may cause nutritional deficiencies, particularly of vitamins D and B12.
Toxic colitis is a rare complication of colonic Crohn disease. It is a clinical syndrome of ileus accompanied by radiographic evidence of colonic dilation; many cases must be treated aggressively with surgical intervention.
Pathophysiology reference
1. Dulai PS, Singh S, Vande Casteele N, et al: Should we divide Crohn's disease into ileum-dominant and isolated colonic diseases? Clin Gastroenterol Hepatol 17(13):2634-2643, 2019. doi: 10.1016/j.cgh.2019.04.040
Symptoms and Signs of Crohn Disease
The most common initial manifestations of Crohn disease are
Chronic diarrhea with abdominal pain, fever, anorexia, and weight loss
The abdomen is tender, and a mass or fullness may be palpable.
Gross rectal bleeding is unusual except in isolated colonic disease, which may manifest similarly to ulcerative colitis. Some patients present with an acute abdomen that simulates acute appendicitis or intestinal obstruction. About 33% of patients have perianal disease (especially fissures and fistulas), which is sometimes the most prominent or even initial complaint.
In children, extraintestinal manifestations frequently predominate over gastrointestinal (GI) symptoms; arthritis, fever of unknown origin, anemia, or growth retardation may be a presenting symptom, whereas abdominal pain or diarrhea may be absent.
With recurrent disease, symptoms vary. Pain is most common and occurs with both simple recurrence and abscess formation. Patients with severe flare-up or abscess are likely to have marked tenderness, guarding, rebound, and a general toxic appearance. Stenotic segments may cause bowel obstruction, with colicky pain, distention, obstipation, and vomiting. Adhesions from previous surgery may also cause bowel obstruction, which begins rapidly, without the prodrome of fever, pain, and malaise typical of obstruction due to a Crohn disease flare-up. An enterovesical fistula may produce air bubbles in the urine (pneumaturia). Draining cutaneous fistulas may occur. Free perforation into the peritoneal cavity is unusual.
Chronic disease causes a variety of systemic symptoms, including fever, weight loss, malnutrition, and other extraintestinal manifestations of IBD.
Diagnosis of Crohn Disease
Barium x-rays of the small bowel
Abdominal CT (conventional or CT enterography)
Sometimes barium enema, magnetic resonance (MR) enterography, upper endoscopy, colonoscopy, and/or video capsule endoscopy
Crohn disease should be suspected in a patient with inflammatory or obstructive symptoms or in a patient without prominent GI symptoms but with perianal fistulas or abscesses or with otherwise unexplained arthritis, erythema nodosum, fever, anemia, or (in a child) stunted growth. A family history of Crohn disease also increases the index of suspicion.
Similar symptoms and signs (eg, abdominal pain, diarrhea) may be caused by other GI disorders, particularly ulcerative colitis. Differentiation from ulcerative colitis may be an issue in the 20% of cases in which Crohn disease is confined to the colon. However, because treatment is similar, this distinction is critical only when surgery or experimental therapy is contemplated.
Patients presenting with an acute abdomen (either initially or during a relapse) should have an abdominal CT scan. These studies may show obstruction, abscesses or fistulas, and other possible causes of an acute abdomen (eg, appendicitis). Ultrasonography may better delineate gynecologic pathology in women with lower abdominal and pelvic pain.
If initial presentation is less acute, an upper GI series with small-bowel follow-through and spot films of the terminal ileum is preferred over conventional CT. However, newer techniques of CT or MR enterography, which combine high-resolution CT or MR imaging with large volumes of ingested contrast, are becoming the procedures of choice in some centers. These imaging studies are virtually diagnostic if they show characteristic strictures or fistulas with accompanying separation of bowel loops.


If findings are questionable, CT enteroclysis or video capsule enteroscopy may show superficial aphthous and linear ulcers. Barium enema x-ray may be used if symptoms seem predominantly colonic (eg, diarrhea) and may show reflux of barium into the terminal ileum with irregularity, nodularity, stiffness, wall thickening, and a narrowed lumen. Differential diagnoses in patients with similar x-ray findings include cancer of the cecum, ileal carcinoid, lymphoma, systemic vasculitis, radiation enteritis, ileocecal tuberculosis, and ameboma.


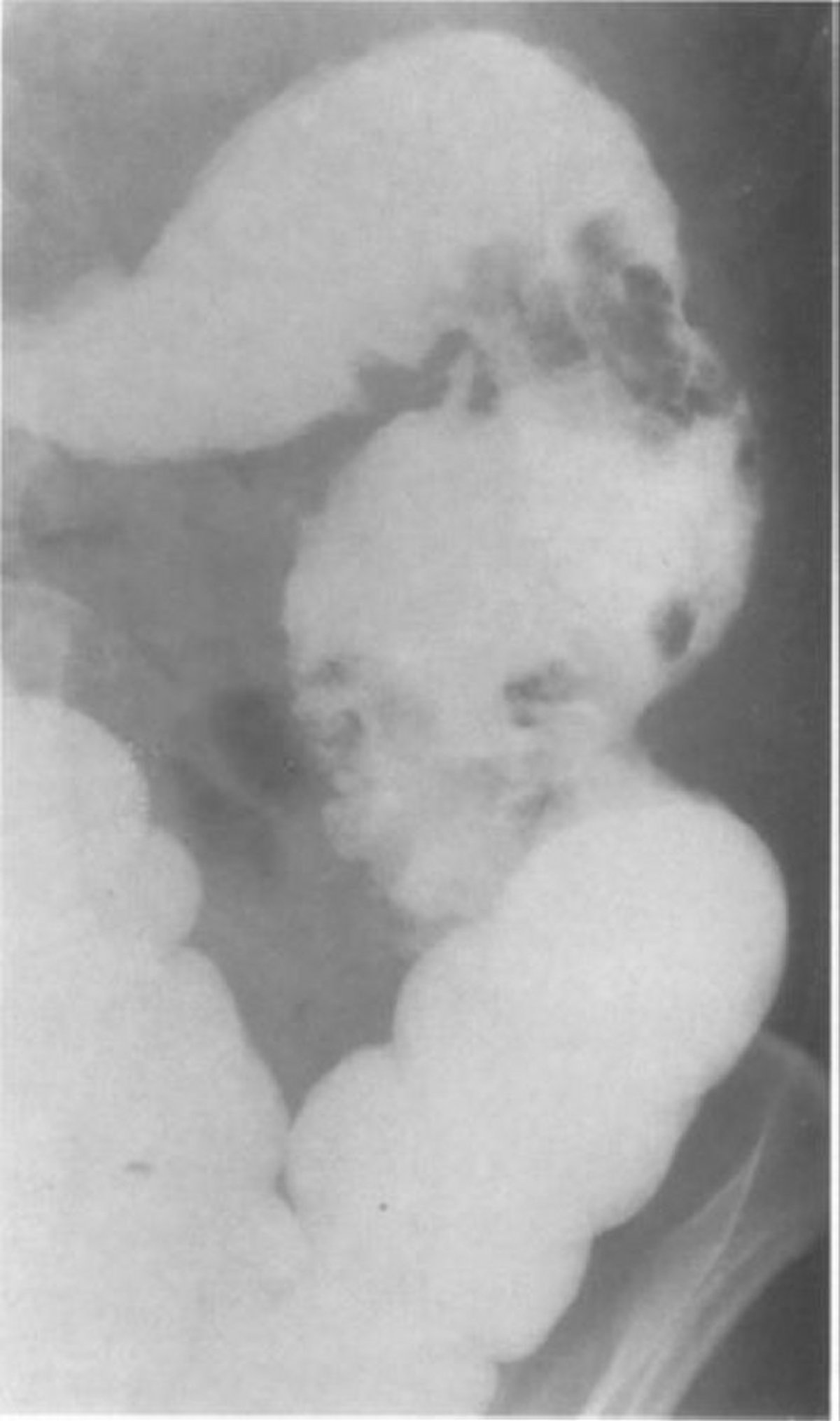
© Springer Science+Business Media
In atypical cases (eg, predominantly diarrhea, with minimal pain), evaluation is similar to that for suspected ulcerative colitis, with colonoscopy (including biopsy, sampling for enteric pathogens, and, when possible, visualization of the terminal ileum). Upper GI endoscopy may identify subtle gastroduodenal involvement even in the absence of upper GI symptoms.
Laboratory testing
Laboratory tests should be done to screen for anemia, hypoalbuminemia, and electrolyte abnormalities. Liver tests should be done; elevated alkaline phosphatase and gamma–glutamyl transpeptidase levels in patients with major colonic involvement suggest possible primary sclerosing cholangitis. Leukocytosis or increased levels of acute-phase reactants (eg, erythrocyte sedimentation rate, C-reactive protein) are nonspecific but may be used serially to monitor disease activity.
To detect nutritional deficiencies, levels of vitamin D and B12 should be checked every 1 to 2 years. Additional laboratory measurements, such as levels of water-soluble vitamins (folic acid and niacin), fat-soluble vitamins (A, D, E and K), and minerals (zinc, selenium, and copper), may be checked when deficiencies are suspected.
All patients with inflammatory bowel disease (IBD), whether male or female, young or old, should have their bone mineral density monitored, usually by dual-energy x-ray absorptiometry (DXA) scan.
Perinuclear antineutrophil cytoplasmic antibodies are present in 60 to 70% of patients with ulcerative colitis and in only 5 to 20% of patients with Crohn disease. Anti–Saccharomyces cerevisiae antibodies are relatively specific for Crohn disease. However, these tests do not reliably separate the 2 diseases and they are not recommended for routine diagnosis. Additional antibodies such as anti-OmpC and anti-CBir1 are now available, but the clinical value of these supplementary tests is uncertain; some studies suggest that high titers of these antibodies have adverse prognostic implications.
Treatment of Crohn Disease
5-Aminosalicylic acid (5-ASA) or antibiotics
Other medications depending on symptoms and severity (eg, immunomodulating medications, biologic agents, and small molecules)
Sometimes surgery
Details of specific medications and dosages are discussed in Medications for Inflammatory Bowel Disease.
(See also the American College of Gastroenterology's 2018 guidelines for the management of Crohn disease in adults.)
General management
Routine health maintenance measures (eg, immunizations, cancer screening) should be emphasized.
Mild disease
This category includes ambulatory patients who tolerate oral intake and have no signs of toxicity, tenderness, mass, or obstruction.
5-ASA® is favored for small-bowel disease, and Asacol® HD is favored for distal ileal and colonic disease. However, the benefits of any 5-ASA drug for small-bowel Crohn disease are modest, and many experts advocate not using it in small-bowel Crohn disease.
Antibiotics are considered a first-line agent by some clinicians, or they may be reserved for patients not responding to 4 weeks of 5-ASA; their use is strictly empiric. With any of these drugs, 8 to 16 weeks of treatment may be required.
Moderate to severe disease
Patients without fistulas or abscesses but with significant pain, tenderness, fever, or vomiting, or those who have not responded to treatment for mild disease, often have rapid relief of symptoms when given corticosteroids
A biologic agent antimetabolite
Obstruction is managed initially with nasogastric suction and IV fluids. Obstruction due to uncomplicated Crohn disease should resolve within a few days and therefore does not require either specific anti-inflammatory therapy or parenteral nutrition; absence of prompt response, however, indicates a complication or another etiology and requires immediate surgery.
Fulminant disease or abscess
Patients with toxic appearance, high fever, persistent vomiting, rebound, or a tender or palpable mass must be hospitalized for administration of IV fluids and antibiotics. Abscesses must be drained, either percutaneously or surgically. IV corticosteroids or biologic agents should be given only when infection has been ruled out or controlled. If there is no response to corticosteroids and antibiotics within 5 to 7 days, surgery is usually indicated.

Fistulas
Anti-TNF therapy is an alternative, but fistulas often relapse after treatment.
Maintenance therapy
Patients who require only 5-ASA or an antibiotic to achieve remission of Crohn disease can be maintained on that medication. Patients requiring acute treatment with corticosteroids or anti-TNF agents
Monitoring during remission can be done by following symptoms and doing blood tests and does not require routine x-rays or colonoscopy (other than regular surveillance for dysplasia after 7 to 8 years of disease).
Surgery
Even though about 70% of patients ultimately require an operation, surgery for Crohn disease is often done reluctantly. It is best reserved for recurrent intestinal obstruction or intractable fistulas or abscesses. Resection of the involved bowel may ameliorate symptoms but does not cure the disease, which is likely to recur even after resection of all clinically apparent lesions.
A meta-analysis of severe endoscopic recurrence after surgery in individuals who were not on IBD medications found that the rate was 50% (1).
Ultimately, further surgery is required in nearly 35% of cases in 10 years (2
Because smoking increases the risk of recurrence, especially in women, smoking cessation should be encouraged.
Treatment references
1. Renna S, Cammà C, Modesto I, et al: Meta-analysis of the placebo rates of clinical relapse and severe endoscopic recurrence in postoperative Crohn's disease. Gastroenterology 135(5):1500-1509, 2008. doi: 10.1053/j.gastro.2008.07.066
2. Fumery M, Dulai PS, Meirick P, et al: Systematic review with meta-analysis: recurrence of Crohn's disease after total colectomy with permanent ileostomy. Aliment Pharmacol Ther 45(3):381-390, 2017. doi: 10.1111/apt.13886
Prognosis for Crohn Disease
Established Crohn disease is rarely cured but is characterized by intermittent exacerbations and remissions. Some patients have severe disease with frequent, debilitating periods of pain. However, with judicious medical therapy and, where appropriate, surgical therapy, most patients function well and adapt successfully. Disease-related mortality is very low. GI cancer, including cancer of the colon and small bowel, is the leading cause of excess Crohn disease-related mortality. Thromboembolic complications (especially during active Crohn colitis) also may cause death. About 10% of people are disabled by Crohn disease and the complications it causes.
Key Points
Crohn disease typically affects the ileum and/or colon but spares the rectum (which is invariably affected in ulcerative colitis).
Intermittent areas of diseased bowel are sharply demarcated from adjacent normal bowel (called skip areas).
Symptoms primarily involve episodic diarrhea and abdominal pain; gastrointestinal bleeding is rare.
Complications include abdominal abscesses and enterocutaneous fistulas.
About 70% of patients ultimately require an operation, typically for recurrent intestinal obstruction, intractable fistulas, or abscesses.
More Information
The following English-language resource may be useful. Please note that THE MANUAL is not responsible for the content of this resource.
American College of Gastroenterology: Guidelines for the management of Crohn disease in adults (2018)







