



- Ambulatory pH Monitoring
- Anoscopy and Sigmoidoscopy
- Endoscopy
- Gastric Analysis
- Impedance Planimetry
- Laparoscopy
- Manometry
- Nasogastric Intubation or Intestinal Intubation
- Nuclear Gastrointestinal Scans
- Paracentesis
- Radiographs and Other Imaging Contrast Studies of the Gastrointestinal Tract
- Other Gastrointestinal Testing and Therapeutic Procedures



Radiographs and Contrast Studies of the Abdomen
Radiographs and other imaging contrast studies visualize the entire gastrointestinal tract from pharynx to rectum and are most useful for detecting mass lesions and structural abnormalities (eg, tumors, strictures).
Single-contrast studies fill the lumen with radiopaque material, outlining the structure. Better, more detailed images are obtained from double-contrast studies, in which a small amount of high-density barium coats the mucosal surface and gas distends the organ and enhances contrast. The gas is injected by the operator in double-contrast barium enema, whereas in other studies, intrinsic gastrointestinal tract gas is adequate. In all cases, patients turn themselves to properly distribute the gas and barium. Fluoroscopy can be used to monitor the progress of the contrast material. Either video or plain radiographs can be taken for documentation, but video is particularly useful when assessing motor disorders (eg, cricopharyngeal spasm, achalasia).
The main contraindication to a radiographic contrast studies is
Suspected perforation
Perforation is a contraindication because free barium is highly irritating to the mediastinum and peritoneum; water-soluble contrast is less irritating and may be used if perforation is possible. Older patients may have difficulty turning themselves to properly distribute the barium and intraluminal gas.
Patients having upper gastrointestinal radiographic contrast studies must have nothing by mouth (npo) after midnight. Patients having barium enema follow a clear liquid diet the day before, take an oral sodium phosphate laxative in the afternoon, and take a bisacodyl suppository in the evening. Other laxative regimens are effective.Patients having upper gastrointestinal radiographic contrast studies must have nothing by mouth (npo) after midnight. Patients having barium enema follow a clear liquid diet the day before, take an oral sodium phosphate laxative in the afternoon, and take a bisacodyl suppository in the evening. Other laxative regimens are effective.
Complications of abdominal radiographic contrast studies are rare. Perforation can occur if barium enema is done in a patient with toxic megacolon. Barium impaction may be prevented by postprocedure oral fluids and sometimes laxatives.
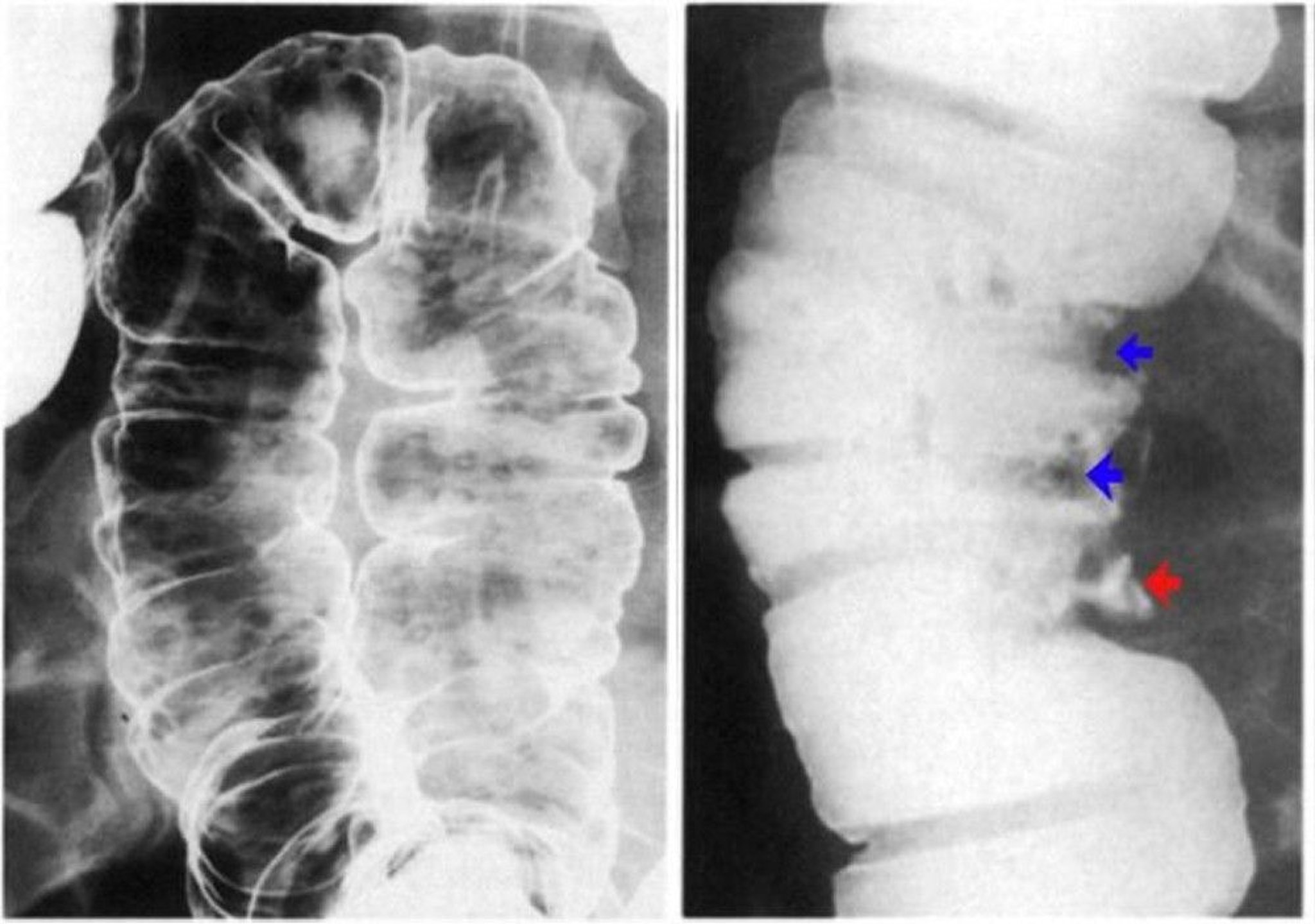
Barium enema
A barium enema can be done as a single- or double-contrast study. Single-contrast barium enemas are used for potential obstruction, diverticulitis, fistulas, and megacolon. Double-contrast studies are preferred for detection of tumors.

© Springer Science+Business Media


Upper gastrointestinal examination
An upper gastrointestinal examination is best done as a biphasic study beginning with a double-contrast examination of the esophagus, stomach, and duodenum, followed by a single-contrast study using low-density barium.
Further evaluation of the small bowel can be accomplished by extending the examination and taking additional radiographic images as the barium contrast extends throughout the rest of the small intestine beyond the duodenum.
Glucagon 0.5 mg IV can facilitate the examination by causing gastric hypotonia.Glucagon 0.5 mg IV can facilitate the examination by causing gastric hypotonia.
CT Scanning of the Abdomen
CT scanning using oral and IV contrast allows excellent visualization of both the small bowel and colon as well as of other intra-abdominal structures.
CT colonography
CT colonography (virtual colonoscopy) generates 3-dimensional and 2-dimensional images of the colon by using multidetector CT and a combination of oral contrast and gas distention of the colon (1). Viewing the high-resolution 3D images somewhat simulates the appearance of optical endoscopy, hence the name. Optimal CT colonography technique requires careful cleansing and distention of the colon. Residual stool causes problems similar to those encountered with barium enema because it simulates polyps or masses. Three-dimensional endoluminal images are useful to confirm the presence of a lesion and to improve diagnostic confidence (2).


CT enterography and MR enterography
CT enterography provides optimal visualization of the small-bowel mucosa; it is preferably done by using a multidetector CT (MDCT) scanner. Patients are given a large volume (1350 mL) of 0.1% barium sulfate before imaging. For certain indications (eg, obscure CT enterography provides optimal visualization of the small-bowel mucosa; it is preferably done by using a multidetector CT (MDCT) scanner. Patients are given a large volume (1350 mL) of 0.1% barium sulfate before imaging. For certain indications (eg, obscuregastrointestinal bleeding, small-bowel tumors, chronic ischemia), a biphasic contrast-enhanced MDCT study is done.
CT enterography and CT colonography have largely supplanted standard small-bowel series, enteroclysis, and barium enema examinations.
Magnetic resonance (MR) enterography can also be used in a similar fashion to CT enterography. It is typically reserved for younger patients, especially those with inflammatory bowel disease, to reduce lifetime radiation exposure risk. MR enterography is more expensive than CT enterography (3).
CT scanning of the abdomen references
1. Yee J, Dachman A, Kim DH, et al. CT Colonography Reporting and Data System (C-RADS): Version 2023 Update [published correction appears in Radiology. 2024 Feb;310(2):e249004. doi: 10.1148/radiol.249004]. Radiology. 2024;310(1):e232007. doi:10.1148/radiol.232007
2. Sha J, Chen J, Lv X, Liu S, Chen R, Zhang Z.. Computed tomography colonography versus colonoscopy for detection of colorectal cancer: a diagnostic performance study. BMC Med Imaging. 2020;20(1):51. Published 2020 May 18. doi:10.1186/s12880-020-00446-7
3. Gandhi NS, Dillman JR, Grand DJ, Huang C, Fletcher JG, Al-Hawary MM, Anupindi SA, Baker ME, Bruining DH, Chatterji M, Fidler JL. Computed tomography and magnetic resonance enterography protocols and techniques: survey of the Society of Abdominal Radiology Crohn’s Disease Disease-Focused Panel. Abdominal Radiology. 2020 Apr;45:1011-7







