


Acute trauma or chronic irritation causes changes in the vocal cords that can lead to polyps, nodules, or granulomas. All cause hoarseness and a breathy voice. Persistence of these symptoms for > 3 weeks dictates visualization of the vocal cords. Diagnosis is based on laryngoscopy and on biopsy in selected cases to rule out cancer. Judicious surgical removal restores the voice, and removal of the irritating source prevents recurrence.


Etiology
Polyps and nodules result from injury to the lamina propria of the true vocal cords. Granulomas result from injury to the perichondrium overlying the vocal processes of the arytenoid cartilages.
Vocal cord polyps may occur at the mid third of the membranous cords and are more often unilateral. Polyps tend to be larger and more protuberant than nodules and often have a dominant surface blood vessel. They frequently result from an initiating acute phonatory injury. Other polypoid changes, often bilateral, may have several other causes, including gastroesophageal reflux, untreated hypothyroid states, chronic laryngeal allergic reactions, or chronic inhalation of irritants, such as industrial fumes or cigarette smoke. Acute injury usually causes pedunculated polyps, whereas polypoid edema results from chronic irritation.
Vocal cord nodules occur bilaterally at the junction of the anterior and middle third of the cords. Their main cause is chronic voice trauma—yelling, shouting, singing loudly, or using an unnaturally low frequency.
Vocal cord granulomas occur in the posterior glottis adjacent to the vocal processes of the arytenoid cartilage. They can be bilateral or unilateral. They usually result from intubation trauma but may be aggravated by reflux disease.
Vocal cord papillomas can result from infection with some human papillomaviruses (HPVs). In pediatric patients, papillomas most commonly occur between age 1 and 4 years, although they can develop at any time including throughout adulthood. The disorder is also called recurrent respiratory papillomatosis.
(See also Overview of Laryngeal Disorders.)
Laryngeal disorders
When relaxed, the vocal cords normally form a V-shaped opening that allows air to pass freely through to the trachea. The cords open during inspiration and close during swallowing or speech. When a mirror is held in the back of a patient’s mouth, the vocal cords can often be seen and checked for disorders, such as contact ulcers, polyps, nodules, paralysis, and cancer. Paralysis may affect one (unilateral) or both vocal cords (bilateral—not shown). |

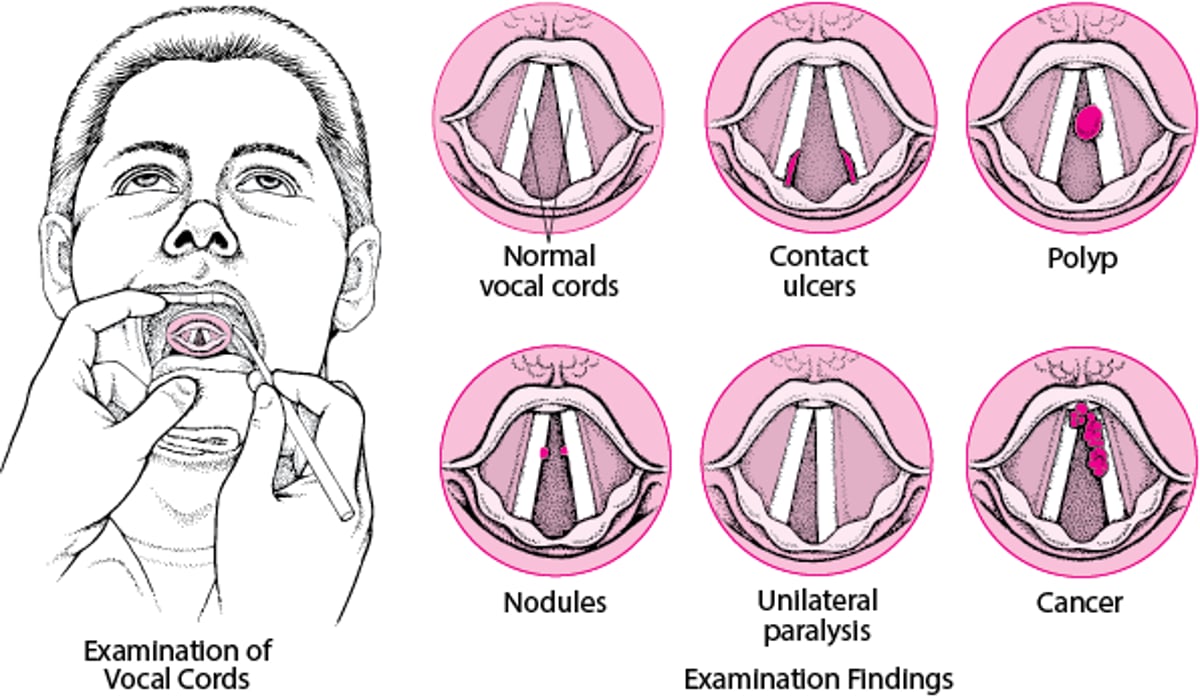

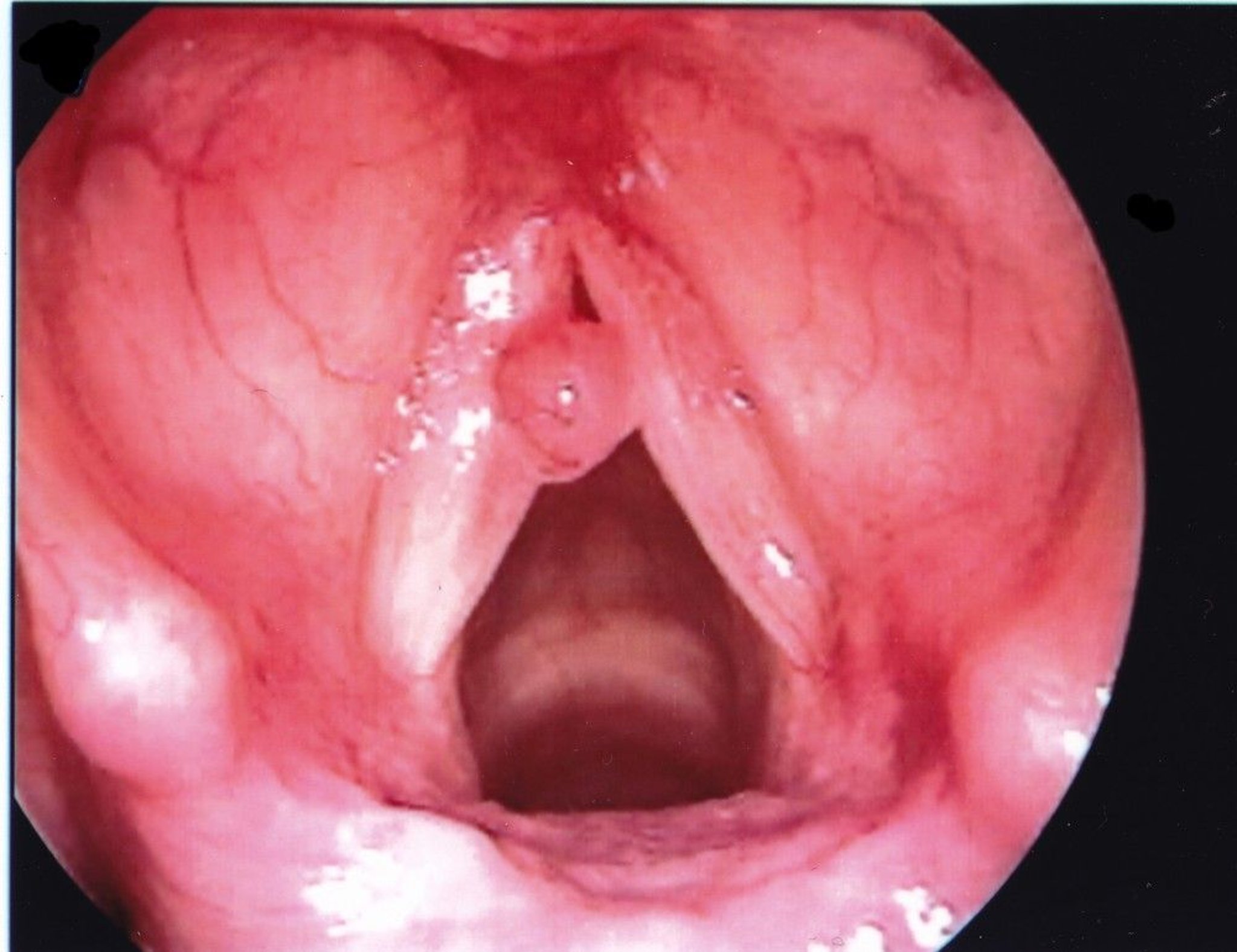
Image provided by Eiji Yanagisawa, MD.

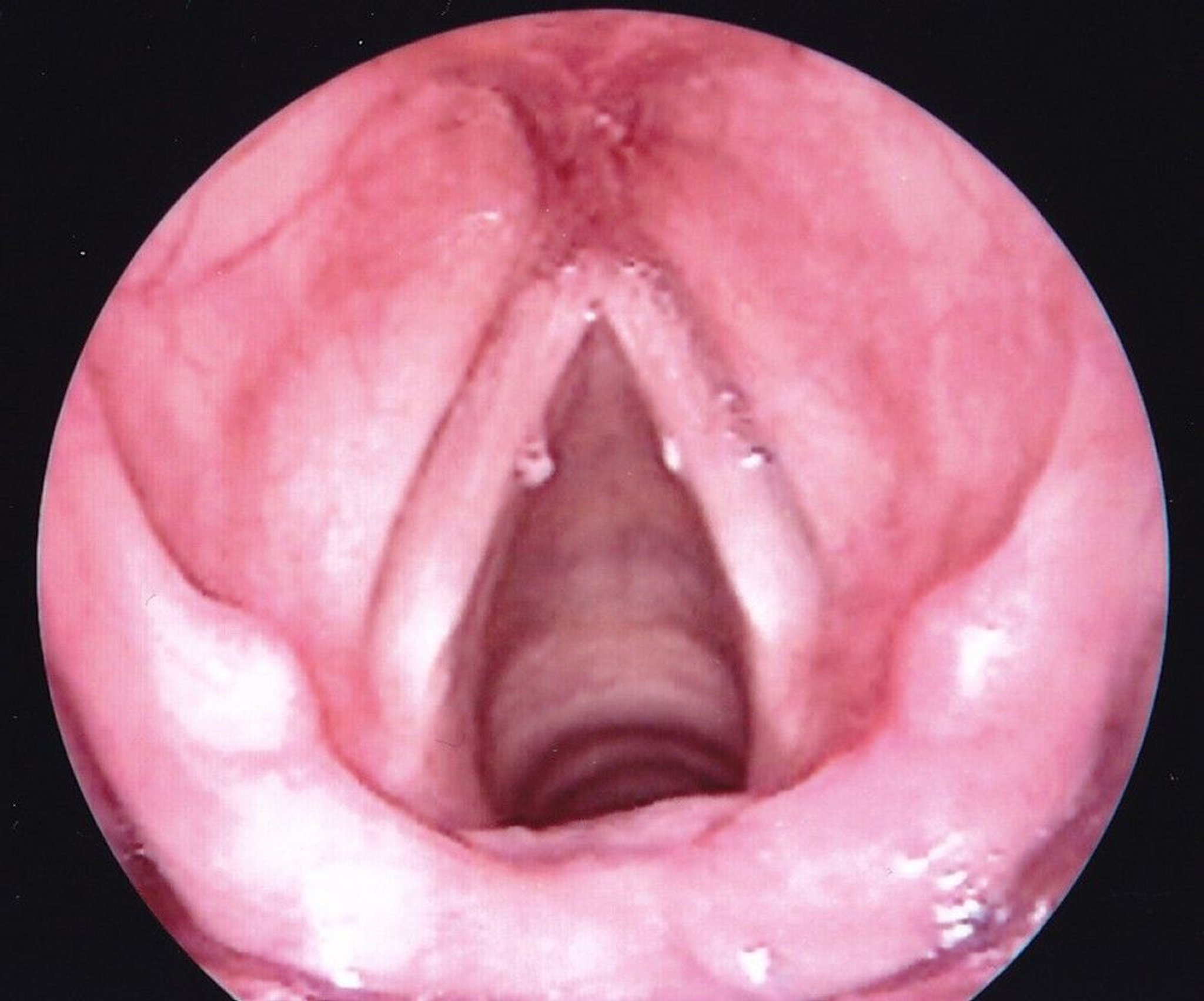
Image provided by Eiji Yanagisawa, MD.

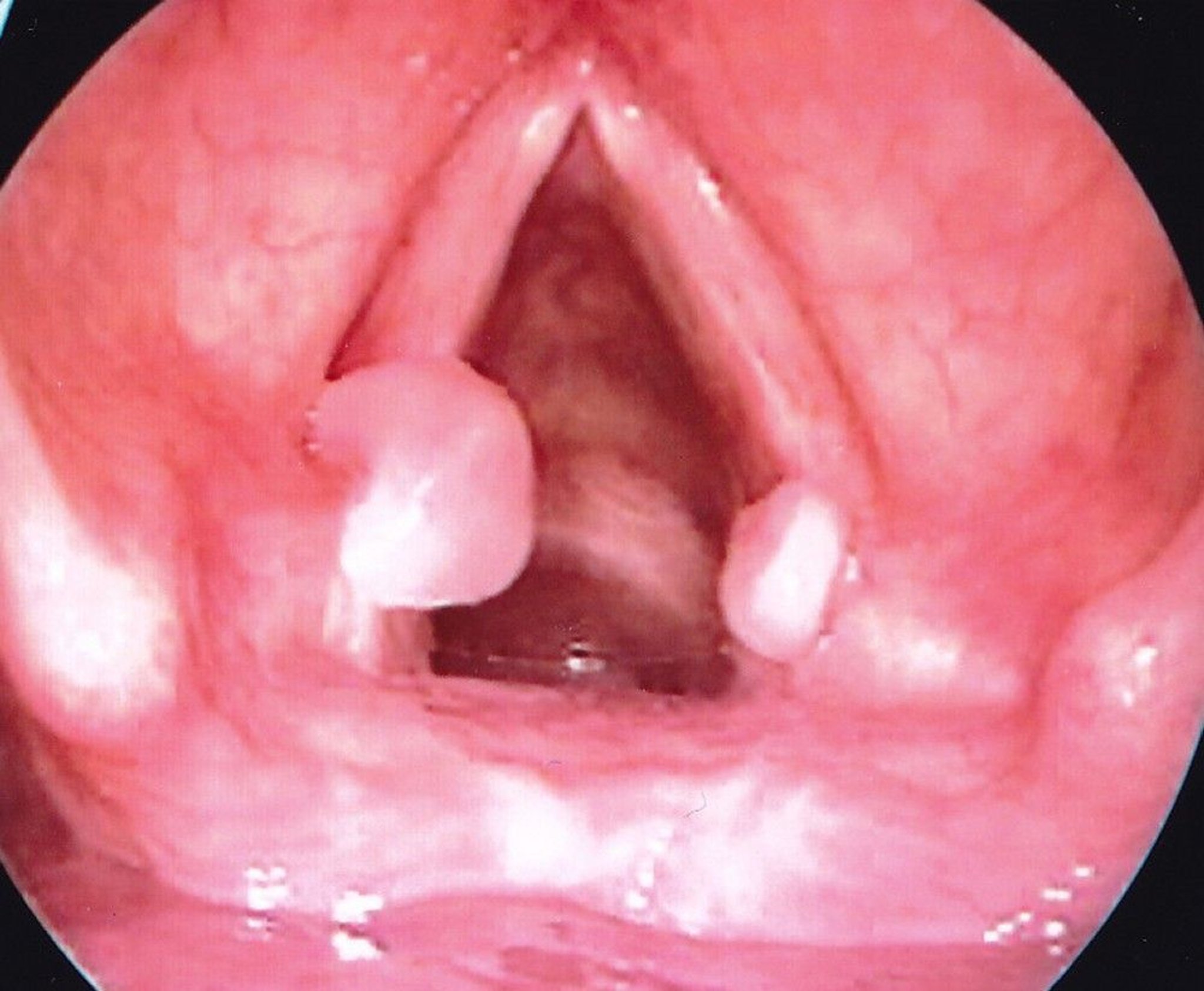
Image provided by Eiji Yanagisawa, MD.
Symptoms and Signs
All polyps, nodules, and granulomas result in slowly developing hoarseness and a breathy voice.
Symptoms of vocal cord papillomas can include hoarseness or a weak cry early, but airway obstruction is possible in advanced disease.
Diagnosis
Laryngoscopy
Sometimes biopsy
Diagnosis of polyps, nodules, granulomas, and papillomas is based on direct or indirect visualization of the larynx with a mirror or laryngoscope (see table Differentiating Vocal Polyps, Nodules, and Granulomas). Biopsy of discrete lesions to exclude carcinoma is done by microlaryngoscopy (see Laryngeal Cancer).
Differentiating Vocal Polyps, Nodules, and Granulomas
Type | Causes | Features | Treatment |
|---|---|---|---|
Polyps | Acute vocal trauma (most common), gastroesophageal reflux, untreated hypothyroid states, chronic laryngeal allergic reactions, chronic inhalation of irritants (eg, industrial fumes, cigarette smoke) | Traumatic lesions are typically unilateral Bilateral polyps are often due to other causes Occur at the mid membranous cord Larger than nodules Often a surface blood vessel | Surgical removal of traumatic polyps Medical treatment, initially, of other polypoid lesions Speech rehabilitative therapy to alter harsh vocal habits |
Nodules | Chronic voice trauma (eg, from yelling, shouting, singing loudly, using an unnaturally low frequency) | Bilateral Occur at the junction of the anterior and middle third of the cords | Behavior modification (eg, decreasing musculoskeletal laryngeal tension when speaking), voice therapy, antireflux therapy |
Granulomas | Cough, reflux disease, endotracheal intubation | Often bilateral but can be unilateral Occur at vocal processes (posterior cords) Larger than nodules | Voice therapy, antireflux therapy For granulomas that do not regress, surgical removal |
Treatment
Avoidance of cause
For polyps, usually surgical removal
Correction of the underlying voice abuse cures most nodules and granulomas and prevents recurrence. Removal of the offending irritants (including treatment of any gastroesophageal reflux) allows healing and is necessary to prevent recurrence. Voice therapy with a speech therapist reduces the trauma to the vocal cords caused by improper singing or protracted loud speaking. Nodules usually regress with voice therapy alone. Granulomas that do not regress can be removed surgically but tend to recur.
Traumatic polyps must be surgically removed to restore a normal voice. Other polypoid lesions, often bilateral, arising from tobacco abuse or hypothyroid states, should initially receive medical management. Cold-knife microsurgical excision during direct microlaryngoscopy is preferable to laser excision, which is more likely to cause collateral thermal injury if improperly applied.
Papillomas are generally treated with laser or surgery. Human papillomaviruses vaccination can be preventive.
In microlaryngoscopy, an operating microscope is used to examine, biopsy, and operate on the larynx. Images can be recorded on video as well. The patient is anesthetized, and the airway is secured by high-pressure jet ventilation through the laryngoscope, endotracheal intubation, or, for an inadequate upper airway, tracheotomy. Because the microscope allows observation with magnification, tissue can be removed precisely and accurately, minimizing damage (possibly permanent) to the vocal mechanism. Laser surgery can be done through the optical system of the microscope to allow for precise cuts. Microlaryngoscopy is preferred for almost all laryngeal biopsies, for procedures involving benign tumors, and for many forms of phonosurgery.
Key Points
Vocal cord polyps, nodules, and granulomas result from acute trauma or chronic irritation; vocal cord papillomas result from human papillomavirus infection.
Symptoms persisting > 3 weeks dictate visualization of the vocal cords.
Biopsy may be necessary to rule out cancer.
After excision, removal of the irritating source is necessary to prevent recurrence.







