



Renovascular hypertension is blood pressure elevation due to partial or complete occlusion of one or more renal arteries or their branches. It is usually asymptomatic unless long-standing. A bruit can be heard over one or both renal arteries in < 50% of patients. Diagnosis is by physical examination and renal imaging with duplex ultrasound, CT angiography, or magnetic resonance angiography. Treatment is with medications and sometimes revascularization by percutaneous angioplasty or surgery.
")
")
(See also Hypertension.)
Renovascular disease is one of the most common causes of reversible hypertension but accounts for < 1% of all cases of hypertension (1). Stenosis or occlusion of a main renal artery, an accessory renal artery, or any of their branches can cause hypertension by stimulating release of renin from juxtaglomerular cells of the affected kidney. The area of the arterial lumen must be decreased by ≥ 70% and a significant poststenotic gradient must be present before stenosis is likely to contribute to blood pressure (BP) elevation.
Overall, about 80% of cases are caused by renal atherosclerosis and 20% by fibromuscular dysplasia. Atherosclerosis is more common among men > 50 years and affects mainly the proximal one-third of the renal artery. Fibromuscular dysplasia is more common among younger patients (usually women) and usually affects the distal two-thirds of the main renal artery and the branches of the renal arteries. Rarer causes include emboli, trauma, inadvertent ligation during surgery, and extrinsic compression of the renal pedicle by tumors.
Renovascular hypertension is characterized by high cardiac output and high peripheral resistance.
General reference
1. Dworkin LD, Cooper CJ. Clinical practice. Renal-artery stenosis. N Engl J Med 361(20):1972-1978, 2009. doi:10.1056/NEJMcp0809200
Symptoms and Signs of Renovascular Hypertension
Renovascular hypertension is usually asymptomatic. A systolic-diastolic bruit in the epigastrium, usually transmitted to one or both upper quadrants and sometimes to the back, is almost pathognomonic, but it is present in only about 50% of patients with fibromuscular dysplasia and is rare in patients with renal atherosclerosis.
Renovascular hypertension should be suspected if
Diastolic hypertension develops abruptly
New or previously stable hypertension rapidly worsens over a period of 6 months
Hypertension is initially severe (eg, systolic BP > 180 mm Hg)
There is unexplained worsening renal function
Hypertension is resistant to medications
A history of trauma to the back or flank or acute pain in this region with or without hematuria suggests renovascular hypertension (possibly due to arterial injury), but these findings are rare.
Asymmetric renal size (> 1 cm difference) discovered incidentally during imaging tests, and recurrent episodes of unexplained acute pulmonary edema or heart failure also suggest renovascular hypertension.
Diagnosis of Renovascular Hypertension
Initial identification with ultrasound, magnetic resonance angiography, or CT angiography
Confirmation with renal angiography (also may be therapeutic)
If renovascular hypertension is suspected, ultrasound, magnetic resonance angiography, or CT angiography are reasonable non-invasive initial tests. Noninvasive testing is less reliable for detecting fibromuscular dysplasia because of the location of the stenotic lesion (which typically involves the intrarenal portion of the renal artery).
Renal angiography is the definitive test, which may be done when noninvasive testing is inconclusive and the clinical suspicion is high.
Duplex Doppler ultrasound can assess renal blood flow and is a reliable, noninvasive method for identifying significant stenosis (eg, > 60%) in the main renal arteries. Sensitivity and specificity are 85 to 90% when experienced technicians do the test (1). It is less accurate in patients with branch stenosis.
Magnetic resonance angiography is a more accurate and specific noninvasive test to assess the renal arteries (2). However, concerns about gadolinium-associated complications, including nephrogenic systemic fibrosis, limit its use, particularly among patients with renal insufficiency.

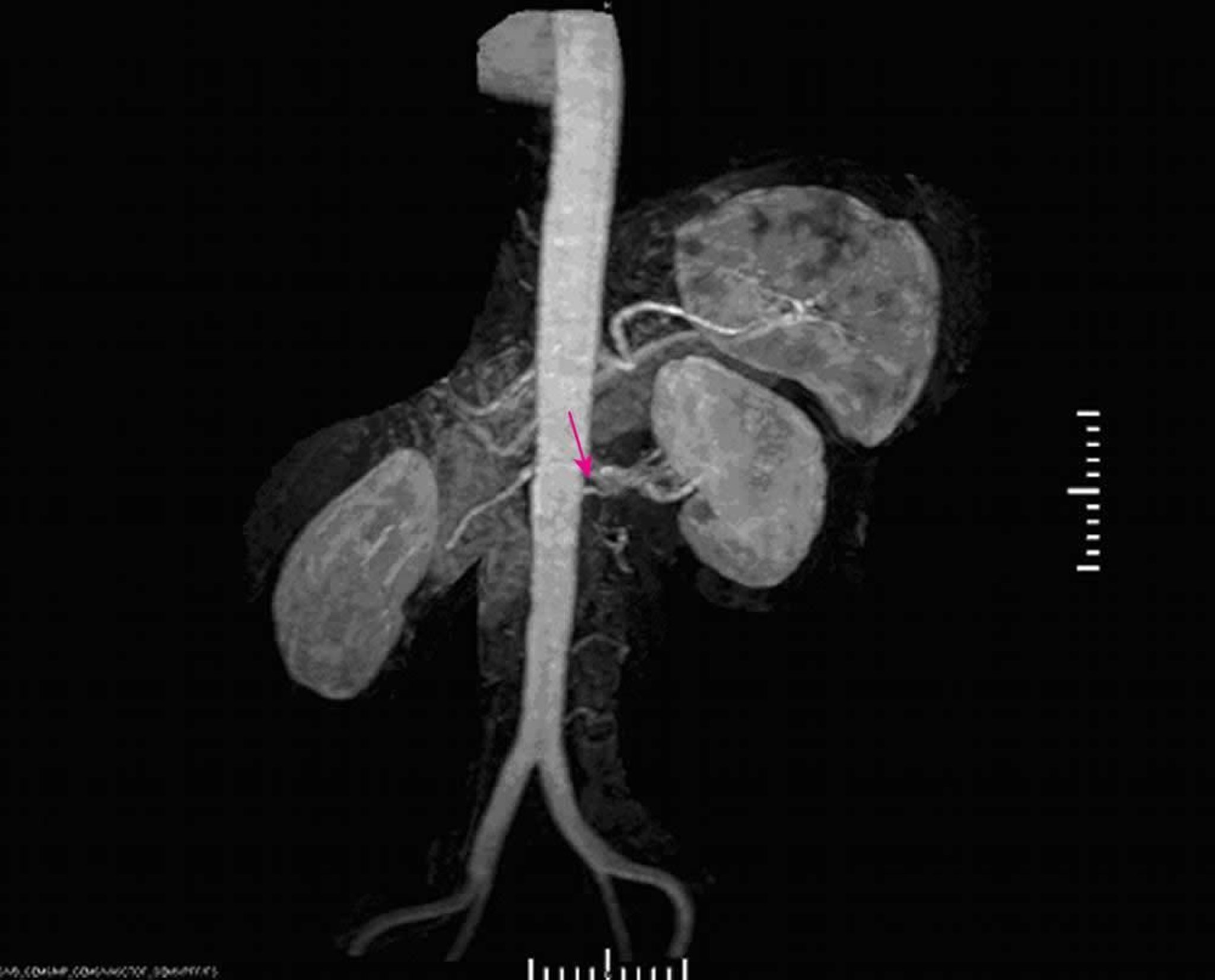
Image provided by Jan N. Basile, MD.
CT angiography is another noninvasive test with sensitivities and specificities in the range of 95% (3). Its use is also limited by exposure to radiocontrast media in patients with renal insufficiency.
Renal angiography is done if noninvasive imaging methods indicate a lesion amenable to angioplasty or stenting or if the results of other screening tests are inconclusive. Digital subtraction angiography with selective injection of the renal arteries can also confirm the diagnosis, but angioplasty or stent placement cannot be done in the same procedure.
Radionuclide imaging is rarely used for diagnostic purposes and is occasionally used as a functional test to compare blood flow and filtration between the kidneys. Imaging is performed before and after an oral dose of captopril. The angiotensin-converting enzyme (ACE) inhibitor causes the affected artery to narrow, decreasing perfusion on the scintiscan. Narrowing also causes an increase in serum renin, which is measured before and after Radionuclide imaging is rarely used for diagnostic purposes and is occasionally used as a functional test to compare blood flow and filtration between the kidneys. Imaging is performed before and after an oral dose of captopril. The angiotensin-converting enzyme (ACE) inhibitor causes the affected artery to narrow, decreasing perfusion on the scintiscan. Narrowing also causes an increase in serum renin, which is measured before and aftercaptopril administration. This test may be less reliable in patients with decreased renal function.


Image provided by Jan N. Basile, MD.
Measurements of renal vein renin activity are sometimes misleading and, unless surgery is being considered, are not necessary. However, in unilateral disease, a renal vein renin activity ratio of > 1.5 (affected to unaffected side) usually predicts a good outcome with revascularization. The test is done when patients are depleted of sodium, stimulating the release of renin.
Diagnosis references
1. Williams GJ, Macaskill P, Chan SF, et al. Comparative accuracy of renal duplex sonographic parameters in the diagnosis of renal artery stenosis: paired and unpaired analysis. AJR Am J Roentgenol 2007;188(3):798-811. doi:10.2214/AJR.06.0355
2. Postma CT, Joosten FB, Rosenbusch G, Thien T. Magnetic resonance angiography has a high reliability in the detection of renal artery stenosis. Am J Hypertens 1997;10(9 Pt 1):957-963. doi:10.1016/s0895-7061(97)00157-x
3. Olbricht CJ, Paul K, Prokop M, et al. Minimally invasive diagnosis of renal artery stenosis by spiral computed tomography angiography. Kidney Int 1995;48(4):1332-1337. doi:10.1038/ki.1995.418
Treatment of Renovascular Hypertension
Aggressive medical management of hypertension, atherosclerosis, and related disorders
For fibromuscular dysplasia, sometimes angioplasty with or without stent placement
Rarely bypass grafting
Without treatment, the prognosis is similar to that for patients with untreated primary hypertension.
All patients should have aggressive medical management of their hypertension.
Atherosclerotic renal artery stenosis
For patients with atherosclerotic renal artery stenosis, data from a large, randomized trial (the cardiovascular outcomes in renal atherosclerotic lesions [CORAL] trial) showed that stent placement did not improve outcomes compared to medical management alone (1). Although stent placement did provide a small (-2 mm Hg), statistically significant decrease in systolic blood pressure, there was no significant clinical benefit for prevention of stroke, myocardial infarction, heart failure, death due to cardiovascular or renal disease, or progression of kidney disease (including the need for renal replacement therapy). Importantly, all patients in the CORAL study received aggressive medical management of their hypertension and diabetes (if present), along with antiplatelet medications and a statin to manage atherosclerosis.
Thus, the decision to eschew angioplasty must be accompanied by strict adherence to current medical management guidelines (2). If serum creatinine increases by > 50% with optimal medical treatment for blood pressure, renal artery stenting may help preserve kidney function (3). For patients unable to strictly adhere to medical management guidelines and with a > 70% renal artery stenosis, stent placement may still be considered.
Fibromuscular dysplasia
For most patients with fibromuscular dysplasia of the renal artery, percutaneous transluminal angioplasty (PTA) is recommended. Placement of a stent reduces the risk of restenosis; antiplatelet medications (eg, aspirin, clopidogrel) are given afterward. Saphenous vein bypass grafting is recommended only when extensive disease in the renal artery branches makes PTA technically unfeasible. Sometimes complete surgical revascularization requires microvascular techniques that can only be done ex vivo with autotransplantation of the kidney. Cure rate is 90% in appropriately selected patients; surgical mortality rate is (PTA) is recommended. Placement of a stent reduces the risk of restenosis; antiplatelet medications (eg, aspirin, clopidogrel) are given afterward. Saphenous vein bypass grafting is recommended only when extensive disease in the renal artery branches makes PTA technically unfeasible. Sometimes complete surgical revascularization requires microvascular techniques that can only be done ex vivo with autotransplantation of the kidney. Cure rate is 90% in appropriately selected patients; surgical mortality rate is< 1% (4).
Medical treatment is always preferable to nephrectomy in patients whose kidneys cannot be revascularized for technical reasons.
Treatment references
1. Cooper CJ, Murphy TP, Cutlip DE, et al: Stenting and medical therapy for atherosclerotic renal-artery stenosis. N Engl J Med 370:13–22, 2014. doi: 10.1056/NEJMoa1310753
2. Whelton PK, Carey RM, Aronow WS, et al: 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 71(6):e13–e115, 2018. doi: 10.1161/HYP.0000000000000065
3. Bhalla V, Textor SC, Beckman JA, et al. Revascularization for Renovascular Disease: A Scientific Statement From the American Heart Association. Hypertension 2022;79(8):e128-e143. doi:10.1161/HYP.0000000000000217
4. Modrall JG, Rosero EB, Smith ST, et al. Operative mortality for renal artery bypass in the United States: Results from the National Inpatient Sample. J Vasc Surg 48(2):317-322, 2008. doi:10.1016/j.jvs.2008.03.014
Key Points
Stenosis (> 70%) or occlusion of a renal artery can cause hypertension by stimulating release of renin from juxtaglomerular cells of the affected kidney.
About 80% of cases are caused by atherosclerosis, and 20% by fibromuscular dysplasia.
Suspect a renovascular cause if diastolic hypertension develops abruptly; if new or previously stable hypertension rapidly worsens within 6 months; or if hypertension is initially severe (systolic > 180 mm Hg), associated with worsening renal function, or highly refractory to treatment with medication.
Do ultrasound, magnetic resonance angiography, or CT angiography to identify patients who should have renal angiography, the definitive test.
Give aggressive medical treatment of hypertension, atherosclerosis, and related disorders.
For patients with fibromuscular dysplasia, consider percutaneous transluminal angioplasty and/or stent placement or rarely a vascular bypass graft.







