



- Overview of Coronary Artery Disease
- Angina Pectoris
- Microvascular Angina
- Vasospastic Angina
- Overview of Acute Coronary Syndromes (ACS)
- Unstable Angina
- Acute Myocardial Infarction (MI)
- Complications of Acute Coronary Syndromes
- Medications for Acute Coronary Syndromes
- Overview of Revascularization for Acute Coronary Syndromes
- Percutaneous Coronary Interventions (PCI)
- Coronary Artery Bypass Grafting (CABG)






Numerous complications can occur as a result of an acute coronary syndrome and increase morbidity and mortality. Complications can be roughly categorized as
Electrical dysfunction (conduction disturbance, arrhythmias)
Mechanical dysfunction (heart failure, myocardial rupture or aneurysm, papillary muscle dysfunction)
Thrombotic complications (recurrent coronary ischemia, mural thrombosis)
Inflammatory complications (pericarditis, post-myocardial infarction syndrome)
Electrical dysfunction occurs in > 90% of patients with myocardial infarction (MI) (see also Arrhythmias and Conduction Disorders). Electrical dysfunction that commonly causes mortality in the first 72 hours includes tachycardia (from any focus) rapid enough to reduce cardiac output and lower blood pressure, Mobitz type II block (second degree) or complete (third degree) atrioventricular (AV) block, ventricular tachycardia (VT), and ventricular fibrillation (VF). Asystole is uncommon, except as a terminal manifestation of progressive left ventricular failure and shock. Patients with disturbances of cardiac rhythm are evaluated for hypoxia and electrolyte abnormalities, which can be causative or contributory.
Sinus Node Disturbances
If the artery supplying the sinus node is affected by an acute coronary syndrome, sinus node disturbances can occur; they are more likely if there is a preexisting sinus node disorder (common among older patients).
Sinus bradycardia
Sinus bradycardia, the most common sinus node disturbance, is usually not treated unless there is hypotension or the heart rate is < 50 beats/minute. A lower heart rate, if not extreme, means reduced cardiac workload and possibly reduced infarct size.
For bradycardia with hypotension (which may reduce myocardial perfusion), atropine 0.5 to 1 mg IV is used; it can be repeated after several minutes if response is inadequate. Several small doses are best because high doses may induce tachycardia. Occasionally, a temporary transvenous pacemaker must be inserted.For bradycardia with hypotension (which may reduce myocardial perfusion), atropine 0.5 to 1 mg IV is used; it can be repeated after several minutes if response is inadequate. Several small doses are best because high doses may induce tachycardia. Occasionally, a temporary transvenous pacemaker must be inserted.
Sinus tachycardia
Persistent sinus tachycardia is usually ominous, often reflecting left ventricular failure and low cardiac output. Without heart failure or another evident cause, this arrhythmia may respond to a beta-blocker, given orally or intravenously depending on degree of urgency.
Atrial Arrhythmias
Atrial arrhythmias (atrial ectopic beats, atrial fibrillation, and, less commonly, atrial flutter) occur in approximately 10 to 20% of patients who have had a myocardial infarction and may reflect left ventricular failure or right atrial infarction (1).
Paroxysmal atrial tachycardia is uncommon and usually occurs in patients who have had previous episodes of it.
Atrial ectopy is usually benign, but if frequency increases, causes, particularly heart failure, are sought. Frequent atrial ectopic beats may respond to a beta-blocker.
Atrial fibrillation
Atrial fibrillation is usually transient if it occurs within the first 24 hours (see figure Atrial Fibrillation). Risk factors include age > 70 years, heart failure, previous history of myocardial infarction, large anterior infarction, atrial infarction, pericarditis, hypokalemia, hypomagnesemia, a chronic lung disorder, and hypoxia.
Atrial Fibrillation

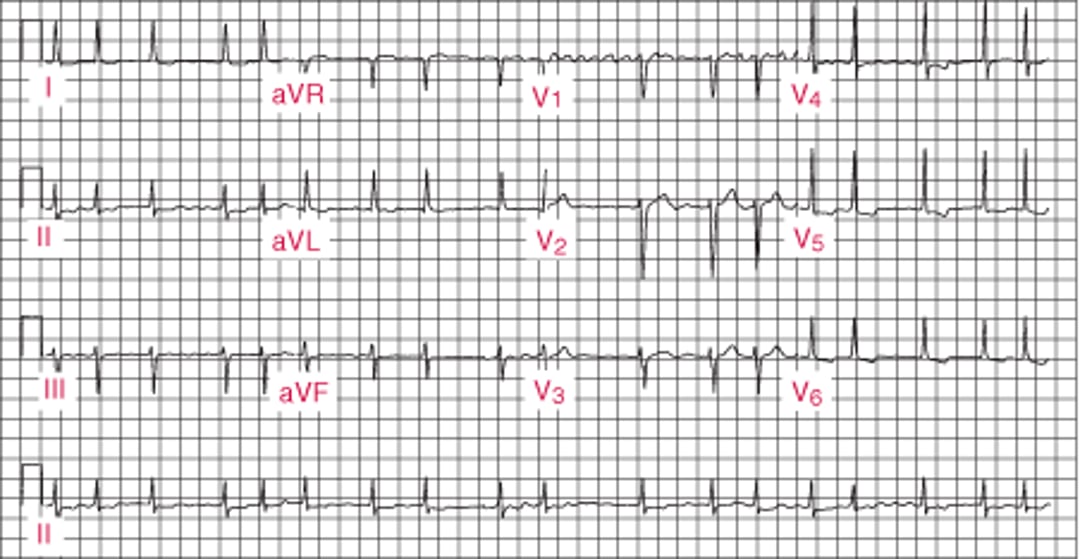
Fibrinolytics reduce incidence of atrial fibrillation.
Recurrent paroxysmal atrial fibrillation is a poor prognostic sign and increases risk of systemic emboli.
For atrial fibrillation, a heparin (unfractionated or low molecular weight) is usually used because of the risk of systemic emboli. For atrial fibrillation, a heparin (unfractionated or low molecular weight) is usually used because of the risk of systemic emboli.
Intravenous beta-blockers (eg, atenolol 2.5 to 5.0 mg over 2 minutes to total dose of 10 mg in 10 to 15 minutes, metoprolol 2 to 5 mg every 2 to 5 minutes to a total dose of 15 mg in 10 to 15 minutes) rapidly slow the ventricular rate and are typically given when heart rate is > 100 beats per minute. Heart rate and blood pressure are closely monitored. Treatment is withheld when ventricular rate decreases satisfactorily or systolic blood pressure is Intravenous beta-blockers (eg, atenolol 2.5 to 5.0 mg over 2 minutes to total dose of 10 mg in 10 to 15 minutes, metoprolol 2 to 5 mg every 2 to 5 minutes to a total dose of 15 mg in 10 to 15 minutes) rapidly slow the ventricular rate and are typically given when heart rate is > 100 beats per minute. Heart rate and blood pressure are closely monitored. Treatment is withheld when ventricular rate decreases satisfactorily or systolic blood pressure is< 100 mm Hg.
Intravenous digoxin, which is not as effective as beta-blockers, is used cautiously and only in patients with atrial fibrillation and left ventricular systolic dysfunction. Usually, Intravenous digoxin, which is not as effective as beta-blockers, is used cautiously and only in patients with atrial fibrillation and left ventricular systolic dysfunction. Usually,digoxin takes at least 2 hours to effectively slow heart rate and may rarely aggravate ischemia in patients with recent acute coronary syndrome.
For patients without evident left ventricular systolic dysfunction or conduction delay manifested by a wide QRS complex, the IV calcium channel blockers verapamil or diltiazem may be used for rate control when beta-blockers are contraindicated or if adequate ventricular rate control is not achieved with other agents. For patients without evident left ventricular systolic dysfunction or conduction delay manifested by a wide QRS complex, the IV calcium channel blockers verapamil or diltiazem may be used for rate control when beta-blockers are contraindicated or if adequate ventricular rate control is not achieved with other agents.Diltiazem may be given as a continuous IV infusion to control heart rate for long periods.
Intravenous amiodarone may also be used for treatment of acute atrial fibrillation, especially when IV beta-blockade or calcium channel blockade is not appropriate or contraindicated (such as in patients with low blood pressure or active asthma). Intravenous amiodarone may also be used for treatment of acute atrial fibrillation, especially when IV beta-blockade or calcium channel blockade is not appropriate or contraindicated (such as in patients with low blood pressure or active asthma).
Due to a high risk of recurrent atrial fibrillation in patients with acute MI, an initial cardioversion strategy may not be preferred. However, if atrial fibrillation compromises circulatory status (eg, causing left ventricular failure, hypotension, or chest pain), urgent electrical synchronized cardioversion is done. If atrial fibrillation returns after cardioversion, IV amiodarone should be considered for patients who continue to experience symptoms (eg chest pain) or remain hemodynamically compromised.is done. If atrial fibrillation returns after cardioversion, IV amiodarone should be considered for patients who continue to experience symptoms (eg chest pain) or remain hemodynamically compromised.
Atrial flutter
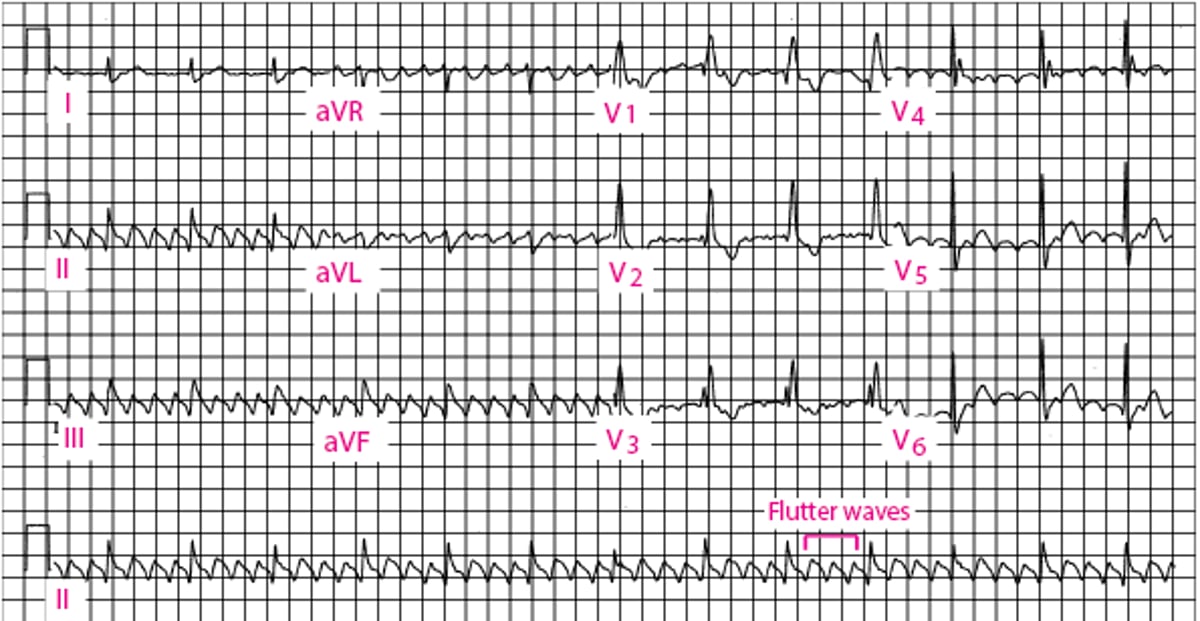
For atrial flutter (see also figure Atrial Flutter), rate is controlled as for atrial fibrillation; a heparin (unfractionated or low molecular weight) is required because the risk of thromboembolism is similar to that with atrial fibrillation. Rate control for atrial flutter in patients with acute MI is usually unsatisfactory. Low-energy direct current (DC) ), rate is controlled as for atrial fibrillation; a heparin (unfractionated or low molecular weight) is required because the risk of thromboembolism is similar to that with atrial fibrillation. Rate control for atrial flutter in patients with acute MI is usually unsatisfactory. Low-energy direct current (DC)synchronized cardioversion will usually terminate atrial flutter.
Atrial Flutter
(Note: Conducted with right bundle branch block.) |

Atrial arrhythmia reference
1. January CT, Wann LS, Calkins H, et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in Collaboration With the Society of Thoracic Surgeons [published correction appears in Circulation 2019 Aug 6;140(6):e285]. Circulation 2019;140(2):e125-e151. doi:10.1161/CIR.0000000000000665
Conduction Defects
Mobitz type I block (Wenckebach block, progressive prolongation of PR interval with eventual dropped beats) is relatively common with an inferior-diaphragmatic infarction (see figure Mobitz Type I Second-Degree Atrioventricular Block); it is usually self-limited and rarely progresses to higher grade block.
Classic Mobitz Type I Second-Degree Atrioventricular Block
The PR interval progressively lengthens with each beat until the atrial impulse is not conducted and the QRS complex is dropped (Wenckebach phenomenon); atrioventricular nodal conduction resumes with the next beat, which has the shortest PR interval, and the sequence is repeated. |


Mobitz type II block (dropped beats) usually indicates massive anterior myocardial infarction, as does complete heart block with wide QRS complexes (atrial impulses do not reach the ventricle); both are uncommon.
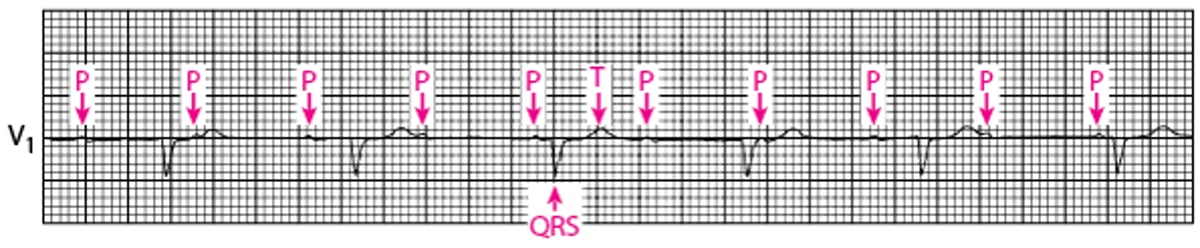
Frequency of third degree atrioventricular (complete) block depends on site of infarction (see figure Third-Degree Atrioventricular Block). Complete AV block occurs in 5 to 10% of patients with inferior infarction and is usually transient. It occurs in < 5% of patients with uncomplicated anterior infarction but in up to 26% of those with right bundle branch block and left posterior hemiblock. Even transient complete AV block with an anterior myocardial infarction is an indication for permanent pacemaker insertion because without pacing the risk of sudden death is significant.
Third-Degree Atrioventricular Block

Treatment of heart block following MI
Mobitz type I block usually does not warrant treatment.
For true Mobitz type II block with dropped beats or for AV block with slow, wide QRS complexes, temporary transvenous pacing is the treatment of choice. External pacing can be used until a temporary transvenous pacemaker can be placed. A permanent pacemaker is required for patients with third degree block and those with persistent second degree AV block, especially if symptomatic.
Although isoproterenol infusion may restore rhythm and rate temporarily, it is not used because it increases oxygen demand and risk of rhythm abnormalities. IV atropine (eg, 0.5 mg IV every 3 to 5 minutes to a total dose of 3 mg) may be useful for narrow-complex Although isoproterenol infusion may restore rhythm and rate temporarily, it is not used because it increases oxygen demand and risk of rhythm abnormalities. IV atropine (eg, 0.5 mg IV every 3 to 5 minutes to a total dose of 3 mg) may be useful for narrow-complexatrioventricular block with a slow ventricular rate but is not recommended for new wide-complex atrioventricular block.
Ventricular Arrhythmias
Ventricular arrhythmias are common and may result from hypoxia, electrolyte imbalance (hypokalemia, possibly hypomagnesemia), or sympathetic overactivity in ischemic cells adjacent to infarcted tissue (which is not electrically active). Treatable causes of ventricular arrhythmias are sought and corrected.
Serum potassium should be kept above 4.0 mEq/L (4.0 mmol/L). IV potassium chloride is recommended; usually 10 mEq/hour (10 mmol/hour) can be infused, but for severe hypokalemia (potassium level Serum potassium should be kept above 4.0 mEq/L (4.0 mmol/L). IV potassium chloride is recommended; usually 10 mEq/hour (10 mmol/hour) can be infused, but for severe hypokalemia (potassium level< 2.5 mEq/L [2.5 mmol/L]), 20 to 40 mEq/hour (20 to 40 mmol/hour) can be infused through a central venous line.
Ventricular ectopic beats, which are common after myocardial infarction, do not warrant specific treatment.
An IV beta-blocker early in myocardial infarction followed by continued oral beta-blockers reduces the incidence of ventricular arrhythmias (including ventricular fibrillation) and mortality in patients who do not have heart failure or hypotension (1). Prophylaxis with other medications (eg, lidocaine) increases mortality risk and is not recommended.). Prophylaxis with other medications (eg, lidocaine) increases mortality risk and is not recommended.
After the acute phase, the presence of complex ventricular arrhythmias or nonsustained ventricular tachycardia, especially with significant left ventricular systolic dysfunction, increases mortality risk. An implantable cardioverter-defibrillator (ICD) should be considered and is indicated when the left ventricular ejection fraction is < 35%. Programmed endocardial stimulation can help select the most effective antiarrhythmics or determine the need for an ICD. Before treatment with an antiarrhythmic or ICD, coronary angiography and other tests are done to look for recurrent myocardial ischemia, which may require percutaneous coronary intervention or coronary artery bypass grafting.
Ventricular tachycardia
Nonsustained ventricular tachycardia (ie, < 30 seconds) and even sustained slow ventricular tachycardia (accelerated idioventricular rhythm) without hemodynamic instability do not usually require treatment in the first 24 to 48 hours (see figure Broad QRS Ventricular Tachycardia).
Synchronized cardioversion is done for
Polymorphic ventricular tachycardia
Sustained (≥ 30 seconds) monomorphic ventricular tachycardia
Any ventricular tachycardia with symptoms of instability (eg, heart failure, hypotension, chest pain)
Ventricular tachycardia without hemodynamic instability may be treated with IV lidocaine, procainamide, or amiodarone. Some clinicians also treat complex ventricular arrhythmias with magnesium sulfate 2 g IV over 5 minutes whether or not serum magnesium level is low. Ventricular tachycardia without hemodynamic instability may be treated with IV lidocaine, procainamide, or amiodarone. Some clinicians also treat complex ventricular arrhythmias with magnesium sulfate 2 g IV over 5 minutes whether or not serum magnesium level is low.
Ventricular tachycardia may occur months after myocardial infarction. Late ventricular tachycardia is more likely to occur in patients with transmural infarction and to be sustained.
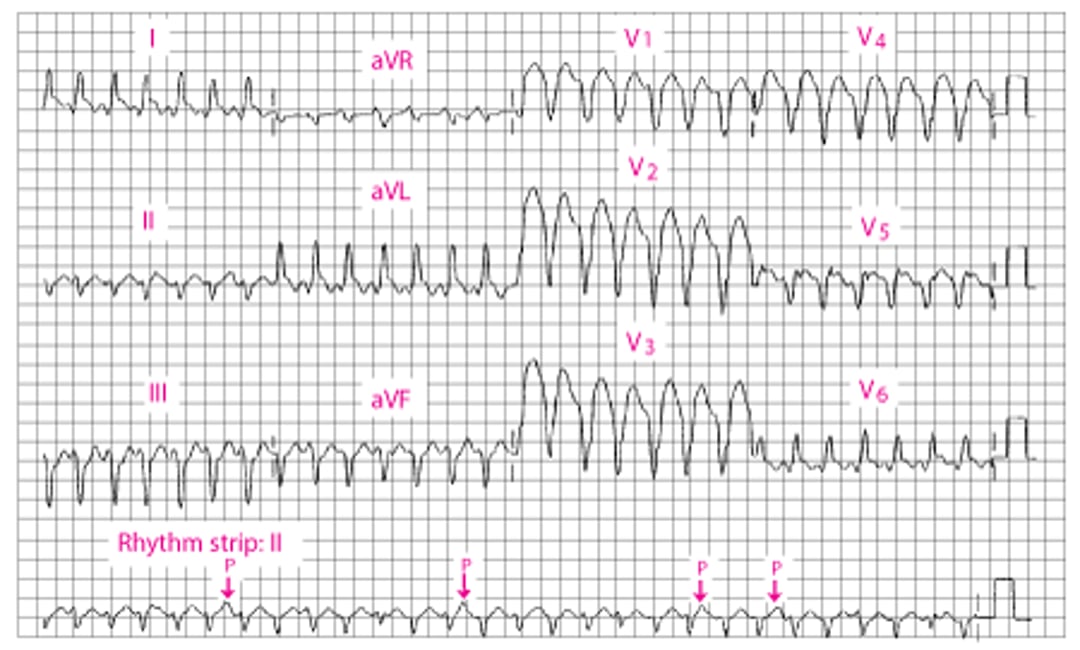
Broad QRS Ventricular Tachycardia
The QRS duration is 160 millisecond. An independent P wave can be seen in II (arrows). There is a leftward mean frontal axis shift. |

Ventricular fibrillation


© Springer Science+Business Media
Ventricular fibrillation occurs in some patients during the first 24 hours after myocardial infarction, usually within 6 hours. Late ventricular fibrillation usually indicates continued or recurrent myocardial ischemia and, when accompanied by hemodynamic deterioration, is a poor prognostic sign. Ventricular fibrillation is treated with immediate unsynchronized cardioversion.
Ventricular arrhythmias reference
1. Freemantle N, Cleland J, Young P, Mason J, Harrison J. beta Blockade after myocardial infarction: systematic review and meta regression analysis. BMJ 1999;318(7200):1730-1737. doi:10.1136/bmj.318.7200.1730
Heart Failure
Heart failure is more likely in patients with
Large infarctions (determined by ECG or cardiac biomarkers)
Mechanical complications (eg, myocardial rupture or aneurysm, papillary muscle dysfunction)
Diastolic dysfunction
Clinical findings depend on infarct size, elevation of left ventricular filling pressure, and degree of reduction in cardiac output. Dyspnea, inspiratory crackles at the lung bases, and hypoxemia are common.
Treatment depends on severity. For mild cases, a loop diuretic (eg, furosemide 20 to 40 mg IV once or twice a day) to reduce ventricular filling pressure is often sufficient. For severe cases, vasodilators (eg, IV nitroglycerin, nitroprusside) are often used to reduce preload and afterload; these agents are effective acutely (eg, in acute Treatment depends on severity. For mild cases, a loop diuretic (eg, furosemide 20 to 40 mg IV once or twice a day) to reduce ventricular filling pressure is often sufficient. For severe cases, vasodilators (eg, IV nitroglycerin, nitroprusside) are often used to reduce preload and afterload; these agents are effective acutely (eg, in acutepulmonary edema) and may be continued over 24 to 72 hours as necessary. During treatment, pulmonary artery occlusion pressure may be measured via right heart (pulmonary artery) catheterization, especially if the response to therapy is not as desired.
Angiotensin-converting enzyme (ACE) inhibitors are used as long as systolic blood pressure remains > 100 mm Hg. A short-acting ACE inhibitor given in low doses (eg, captopril 3.125 to 6.25 mg orally every 4 to 6 hours, increasing doses as tolerated) is best for initial treatment. Once the maximum dose is reached (eg, maximum for captopril, 50 mg 3 times a day), a longer-acting ACE inhibitor (eg, fosinopril, lisinopril, perindopril, ramipril) is substituted for the long-term. If the patient remains in New York Heart Association class II or worse (see table 100 mm Hg. A short-acting ACE inhibitor given in low doses (eg, captopril 3.125 to 6.25 mg orally every 4 to 6 hours, increasing doses as tolerated) is best for initial treatment. Once the maximum dose is reached (eg, maximum for captopril, 50 mg 3 times a day), a longer-acting ACE inhibitor (eg, fosinopril, lisinopril, perindopril, ramipril) is substituted for the long-term. If the patient remains in New York Heart Association class II or worse (see tableClassification of Heart Failure), an aldosterone inhibitor (eg, eplerenone, spironolactone) should be added. ), an aldosterone inhibitor (eg, eplerenone, spironolactone) should be added.
For severe heart failure, an intraarterial counterpulsation balloon pump or an implantable intravascular ventricular assist pump may provide temporary hemodynamic support until the patient stabilizes or the decision is made to provide more advanced support. When revascularization or surgical repair is not feasible, heart transplantation is considered. Long-term left ventricular or biventricular implantable assist devices may be used as a bridge to transplantation. If transplantation is impossible, the left ventricular assist device is increasingly used as permanent treatment (destination therapy). Occasionally, use of such a device results in recovery and can be removed in 3 to 6 months.
Papillary Muscle Disorders
Functional papillary muscle insufficiency occurs in about 35 to 40% of patients during the first few hours of infarction (1). Papillary muscle ischemic dysfunction causes incomplete coaptation of the mitral valve leaflets, which is transient in most patients. But in some patients, papillary muscle or free wall scarring causes permanent mitral regurgitation. Functional papillary muscle insufficiency is characterized by an apical late systolic murmur and typically resolves without treatment.
Papillary muscle rupture occurs most often after an inferoposterior infarct due to right coronary artery occlusion. It causes acute, severe mitral regurgitation. Papillary muscle rupture is characterized by the sudden appearance of a loud apical holosystolic murmur and thrill, usually with pulmonary edema. Occasionally, severe regurgitation is silent. An abrupt hemodynamic deterioration raises clinical suspicion of papillary muscle rupture; echocardiography should always be done to make the diagnosis. Urgent mitral valve repair or replacement is necessary and effective.
Papillary muscle disorders reference
1. Tanimoto T, Imanishi T, Kitabata H, et al. Prevalence and clinical significance of papillary muscle infarction detected by late gadolinium-enhanced magnetic resonance imaging in patients with ST-segment elevation myocardial infarction. Circulation 2010;122(22):2281-2287. doi:10.1161/CIRCULATIONAHA.109.935338
Myocardial Rupture
Interventricular septum or free wall rupture occurs in 1% of patients with acute myocardial infarction. It causes 15% of hospital mortality.
Interventricular septum rupture, although rare, is 8 to 10 times more common than papillary muscle rupture. Interventricular septum rupture is characterized by the sudden appearance of a loud systolic murmur and thrill medial to the apex along the left sternal border in the third or fourth intercostal space, accompanied by hypotension with or without signs of left ventricular failure. Diagnosis may be confirmed using a balloon-tipped catheter and comparing blood oxygen saturation or partial pressure of oxygen (PO2) of right atrial, right ventricular, and pulmonary artery samples. A significant increase in right ventricular PO2 is diagnostic, as is Doppler echocardiography, which may demonstrate the actual shunt of blood across the ventricular septum.
Treatment is surgery, which should be delayed if possible for up to 6 weeks after MI so that infarcted myocardium can heal maximally; if hemodynamic instability persists, earlier surgery is indicated despite a high mortality risk.
Free wall rupture increases in incidence with age and is more common among women. It is characterized by sudden loss of arterial pressure with momentary persistence of sinus rhythm and often by signs of cardiac tamponade. Surgery is rarely successful. Rupture of a free wall is almost always fatal.
Ventricular Aneurysm
A localized bulge in the ventricular wall, usually the left ventricular wall, can occur at the site of a large infarction. Ventricular aneurysms are common, especially with a large transmural infarct (usually anterior). Aneurysms may develop in a few days, weeks, or months. They are unlikely to rupture but may lead to recurrent ventricular arrhythmias, low cardiac output, and mural thrombosis with systemic embolism.
A ventricular aneurysm may be suspected when paradoxical precordial movements are seen or felt, ECG shows persistent ST-segment elevation, and chest x-ray shows a characteristic bulge of the cardiac shadow. Because these findings are not diagnostic of an aneurysm, echocardiography is done to confirm the diagnosis and determine whether a thrombus is present.
Surgical excision may be indicated when left ventricular failure or arrhythmia persists. Early revascularization and probably the use of angiotensin-converting enzyme (ACE) inhibitors during acute myocardial infarction modify left ventricular remodeling and have reduced the incidence of aneurysm.
Pseudoaneurysm is incomplete rupture of the free left ventricular wall; it is limited by the pericardium. Pseudoaneurysms may be large, contributing to heart failure, almost always contain a thrombus, and often rupture completely. They are repaired surgically.
Hypotension and Cardiogenic Shock
Hypotension
Hypotension may be due to
Decreased ventricular filling
Loss of contractile force secondary to massive myocardial infarction
Marked hypotension (eg, systolic blood pressure < 90 mm Hg) with tachycardia and symptoms of end-organ hypoperfusion (reduced urine output, mental confusion, diaphoresis, cold extremities) is termed cardiogenic shock. Pulmonary congestion develops rapidly in cardiogenic shock.
Decreased left ventricular filling is most often caused by reduced venous return secondary to hypovolemia, especially in patients receiving intensive loop diuretic therapy, but it may reflect right ventricular infarction. Marked pulmonary congestion suggests loss of left ventricular contractile force (left ventricular failure) as the cause.
Treatment depends on the cause. In some patients, determining the cause requires use of a pulmonary artery catheter to measure intracardiac pressures.
For hypotension due to hypovolemia, cautious fluid replacement with 0.9% saline is usually possible without left heart overload (excessive rise in left atrial pressure). However, sometimes left ventricular function is so compromised that adequate fluid replacement sharply increases pulmonary artery occlusion pressure to levels associated with pulmonary edema (> 25 mm Hg). If left atrial pressure is high, hypotension is probably due to left ventricular failure, and if diuretics are ineffective, inotropic therapy or circulatory support may be required.
Cardiogenic shock
Approximately 5 to 10% of patients with acute myocardial infarction have cardiogenic shock (1).
In cardiogenic shock, an alpha-agonist or beta-agonist may be temporarily effective. Dopamine, a catecholamine with alpha and beta 1 effects, is given IV at 0.5 to 1 mcg/kg/minute, increased until response is satisfactory or the dose is about 10 mcg/kg/minute. Higher doses induce vasoconstriction and atrial and ventricular arrhythmias. In cardiogenic shock, an alpha-agonist or beta-agonist may be temporarily effective. Dopamine, a catecholamine with alpha and beta 1 effects, is given IV at 0.5 to 1 mcg/kg/minute, increased until response is satisfactory or the dose is about 10 mcg/kg/minute. Higher doses induce vasoconstriction and atrial and ventricular arrhythmias.
Dobutamine, a beta-agonist, is another agent that may be given IV at 2.5 to 10 mcg/kg/minute or in higher doses. It often causes or exacerbates hypotension; it is most effective when hypotension is secondary to low cardiac output with increased peripheral vascular resistance. Dopamine is more effective than Dobutamine, a beta-agonist, is another agent that may be given IV at 2.5 to 10 mcg/kg/minute or in higher doses. It often causes or exacerbates hypotension; it is most effective when hypotension is secondary to low cardiac output with increased peripheral vascular resistance. Dopamine is more effective thandobutamine when a vasopressor effect is also required.
In refractory cases of cardiogenic shock, dobutamine and dopamine may be combined. The combination of In refractory cases of cardiogenic shock, dobutamine and dopamine may be combined. The combination ofdobutamine plus a drug with more alpha-adrenergic effects (phenylephrine, plus a drug with more alpha-adrenergic effects (phenylephrine,norepinephrine) may be effective without causing excessive arrhythmias.
An intraortic counterpulsation balloon pump may often temporarily support the patient, but it is not clear whether there is short-term or long-term benefit to this approach. Alternatives include a percutaneous or surgically implanted left ventricular assist device and occasionally heart transplantation.
Definitive treatment for postinfarction cardiogenic shock is revascularization by thrombolysis of the clot, angioplasty, or emergency coronary artery bypass grafting. Revascularization usually greatly improves ventricular function. If coronary anatomy is suitable, percutaneous coronary intervention or coronary artery bypass grafting may be considered for persistent ischemia, refractory ventricular arrhythmia, hemodynamic instability, or shock.
Hypotension and cardiogenic shock reference
1. Lauridsen MD, Rørth R, Lindholm MG, et al. Trends in first-time hospitalization, management, and short-term mortality in acute myocardial infarction-related cardiogenic shock from 2005 to 2017: A nationwide cohort study. Am Heart J 2020;229:127-137. doi:10.1016/j.ahj.2020.08.012
Right Ventricular Ischemia or Infarction
Right ventricular infarction rarely occurs in isolation; it usually accompanies inferior left ventricular infarction. The first sign may be hypotension developing in a previously stable patient.
Right-sided ECG leads may show ST-segment changes. Volume loading with 1 to 2 L of 0.9% saline is often effective. Dobutamine or milrinone (which has better dilating effects on the pulmonary circulation) may help. Nitrates and diuretics are not used; they reduce preload (and hence cardiac output), causing severe hypotension. Increased right-sided filling pressure should be maintained by IV fluid infusion, but excessive volume overload may compromise left ventricular filling and cardiac output.Right-sided ECG leads may show ST-segment changes. Volume loading with 1 to 2 L of 0.9% saline is often effective. Dobutamine or milrinone (which has better dilating effects on the pulmonary circulation) may help. Nitrates and diuretics are not used; they reduce preload (and hence cardiac output), causing severe hypotension. Increased right-sided filling pressure should be maintained by IV fluid infusion, but excessive volume overload may compromise left ventricular filling and cardiac output.
Pearls & Pitfalls
|
Recurrent Ischemia
Any chest pain that remains or recurs 12 to 24 hours after myocardial infarction may represent recurrent ischemia. Post-MI ischemic pain indicates that more myocardium is at risk of infarction. Usually, recurrent ischemia can be identified by reversible ST-T changes on the ECG; blood pressure may be elevated.
Recurrent ischemia is silent (ECG changes without pain) in up to one third of patients, so serial ECGs are routinely done every 8 hours for 1 day and then daily. Recurrent ischemia is treated similarly to unstable angina. Sublingual or IV nitroglycerin is usually effective. Coronary angiography and Recurrent ischemia is silent (ECG changes without pain) in up to one third of patients, so serial ECGs are routinely done every 8 hours for 1 day and then daily. Recurrent ischemia is treated similarly to unstable angina. Sublingual or IV nitroglycerin is usually effective. Coronary angiography andrevascularization with percutaneous coronary intervention or coronary artery bypass grafting should be considered to salvage ischemic myocardium.
Mural Thrombosis
A retrospective cohort study including 2136 patients with acute anterior MI who were treated with PCI found that 3.9% of patients developed a left ventricular mural thrombosis during the hospitalization (1). Because risk is low, routine prophylaxis with anticoagulation is not indicated.
Anticoagulant therapy may be considered for patients with STEMI and anterior wall akinesis or dyskinesis, but the patient's risk of bleeding must also be evaluated in light of dual antiplatelet therapy and resultant triple therapy should anticoagulation be chosen. Anticoagulants are recommended for patients after ACS with concomitant:
Atrial fibrillation and high thromboembolic risk (eg, see table CHA2DS2-VASc score of ≥ 2)
Mechanical heart valves
Venous thromboembolism
Hypercoagulable disorders
It also is reasonable to give anticoagulants to patients with STEMI and asymptomatic confirmed LV mural thrombi (2).
The American Heart Association has published guidelines regarding the management of patients at risk for left ventricular thrombus, including patients at risk after acute MI (2).
Mural thrombus references
1. Boivin-Proulx LA, Ieroncig F, Demers SP, et al. Contemporary incidence and predictors of left ventricular thrombus in patients with anterior acute myocardial infarction. Clin Res Cardiol 2023;112(4):558-565. doi:10.1007/s00392-023-02158-8
2. Levine GN, McEvoy JW, Fang JC, et al. Management of Patients at Risk for and With Left Ventricular Thrombus: A Scientific Statement From the American Heart Association. Circulation 2022;146(15):e205-e223. doi:10.1161/CIR.0000000000001092
Pericarditis
Pericarditis results from extension of myocardial necrosis through the wall to the epicardium; it develops in about one third of patients with acute transmural myocardial infarction, although the rate appears to be much less in patients who have early reperfusion done.
A friction rub usually begins 24 to 96 hours after myocardial infarction onset. Earlier onset of the friction rub is unusual, although hemorrhagic pericarditis occasionally complicates the early phase of myocardial infarction. Acute tamponade is rare.
Pericarditis is diagnosed by ECG, which shows diffuse ST-segment elevation and sometimes PR-interval depression. Echocardiography is frequently done, but results are usually normal. Occasionally, small pericardial effusions and even unsuspected tamponade are detected.
Aspirin or another nonsteroidal anti-inflammatory drug (NSAID) usually relieves symptoms. Colchicine 0.5 to 1 mg orally once a day, alone, and especially added to conventional treatment, speeds recovery and helps prevent recurrences. High doses or prolonged use of NSAIDs or corticosteroids may impair infarct healing and should be avoided; corticosteroids may also increase the likelihood of recurrence. Anticoagulation is not contraindicated in early peri-infarction pericarditis but is contraindicated in later post-MI (Dressler) syndrome.Aspirin or another nonsteroidal anti-inflammatory drug (NSAID) usually relieves symptoms. Colchicine 0.5 to 1 mg orally once a day, alone, and especially added to conventional treatment, speeds recovery and helps prevent recurrences. High doses or prolonged use of NSAIDs or corticosteroids may impair infarct healing and should be avoided; corticosteroids may also increase the likelihood of recurrence. Anticoagulation is not contraindicated in early peri-infarction pericarditis but is contraindicated in later post-MI (Dressler) syndrome.
Post-MI Syndrome (Dressler Syndrome)
Post-MI syndrome develops in a few patients several days to weeks or even months after acute myocardial infarction; incidence also appears to have decreased in recent years. It is characterized by fever, pericarditis with a friction rub, pericardial effusion, pleuritis, pleural effusions, pulmonary infiltrates, and joint pain. This syndrome is caused by an autoimmune reaction to material from necrotic myocytes. It may recur.
Differentiating post-MI syndrome from extension or recurrence of infarction may be difficult. However, in post-MI syndrome, cardiac biomarkers do not increase significantly, and ECG changes are nonspecific.
NSAIDs are usually effective, but the syndrome can recur several times. Colchicine is effective for treatment and to prevent recurrences. In severe cases, a short, intensive course of another NSAID or a corticosteroid may be necessary. High doses of an NSAID or a corticosteroid are not used for more than a few days because they may interfere with early ventricular healing after an acute myocardial infarction.NSAIDs are usually effective, but the syndrome can recur several times. Colchicine is effective for treatment and to prevent recurrences. In severe cases, a short, intensive course of another NSAID or a corticosteroid may be necessary. High doses of an NSAID or a corticosteroid are not used for more than a few days because they may interfere with early ventricular healing after an acute myocardial infarction.







