

Complete examination of all systems is essential to detect peripheral and systemic effects of cardiac disorders and evidence of noncardiac disorders that might affect the heart (1). Examination includes the following:
General appearance
Vital sign measurement
Pulse palpation and auscultation
Vein observation
Chest inspection and palpation
Cardiac percussion, palpation, and auscultation
Lung examination, including percussion, palpation, and auscultation
Extremity and abdomen examination
Cardiac auscultation is discussed in a separate topic. Despite the ever-increasing use of cardiac imaging, bedside auscultation remains useful as it is always available and can be repeated as often as desired without cost.
Examination also includes the collection of other patient data.
General reference
1. Fang JC, O'Gara PT: History and Physical Examination: An Evidence-Based Approach. In Libby P, Bonoow RO, Mann DL, et al (eds): Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, 12th ed. Philadelphia, Elsevier, 2022, pp 123-140.
Vital Signs
Vital signs include
Blood pressure
Heart rate and rhythm
Respiratory rate
Temperature
Peripheral oxygen saturation (SpO2)
Weight and height provide additional important data.
Blood pressure (BP) is measured in both arms and, for suspected congenital cardiac disorders or peripheral vascular disorders, in both legs. The bladder of an appropriately sized cuff encircles 80% of the limb’s circumference, and the bladder’s width is 40% of the circumference. When measured by auscultation, the first sound heard as the mercury column falls is systolic pressure; disappearance of the sound is diastolic pressure (fifth-phase Korotkoff sound). Up to a 15 mm Hg pressure differential between the right and left arms is normal; a greater differential suggests a vascular abnormality (eg, dissecting thoracic aorta) or a peripheral vascular disorder. Leg pressure is usually 15 to 20 mm Hg higher than arm pressure due to normal pulse amplification (1). In many clinical settings, blood pressure is measured using an automated device (2). To obtain an accurate blood pressure measurement, the patient should
Be seated in a chair (not on the examination table) for > 5 minutes, feet on floor, back supported
Have the limb supported at heart level with no clothing covering the area of cuff placement
Abstain from exercising, consuming caffeine, or using tobacco for at least 30 minutes before the measurement is taken


JIM VARNEY/SCIENCE PHOTO LIBRARY
Heart rate and rhythm are assessed by palpating the carotid or radial pulse, by using a pulse oximeter or automated blood pressure cuff with that function, or, if arrhythmia is suspected, by cardiac auscultation; some heartbeats during arrhythmias may be audible but do not generate a palpable pulse. Heart rate normally varies with respiration (respiratory sinus arrhythmia), increasing in inspiration due to changes in venous return and vagal nerve tone; this effect is more pronounced in the children, adolescents, and healthy young adults.
Respiratory rate, if abnormal, may indicate cardiac decompensation or a primary lung disorder. The rate increases in patients with heart failure or anxiety and decreases or becomes intermittent in patients who are moribund. Shallow, rapid respirations may indicate pleuritic pain.
Temperature may be elevated by acute rheumatic fever or cardiac infection (eg, endocarditis). After a myocardial infarction, low grade fever is very common. Other causes are sought only if fever persists > 72 hours.
Weight is collected at each clinic visit with the patient on a standing scale and, ideally, while wearing a similar amount of clothing. In patients with heart failure, weight gain may indicate hypervolemia, while weight loss may indicate cardiac cachexia (unintentional, non-edematous weight loss of > 5% within the last 12 months—3). History and additional findings from the physical examination (jugular veins, lung and extremity examinations) are required to determine whether weight changes are related to changes in volume status and/or amount of muscle or fat.
Peripheral arterial oxygen saturation (SpO2) (pulse oximetry) measures the oxygen saturation of hemoglobin in arterial blood and serves as a rapid, noninvasive estimation of tissue oxygenation. Pulse oximetry is obtained by using a probe attached to a finger or earlobe. SpO2 ≥ 95% is considered normal, whereas values < 95% suggest hypoxemia. Baseline oxygen saturation is lower in many patients with chronic obstructive pulmonary disease (COPD); in these patients, when supplemental oxygen is used, the target SpO2 is typically 88 to 92%. When hypoxemia is present, potential cardiac etiologies include pulmonary edema in patients with heart failure and right-to-left intracardiac shunts (a patent foramen ovale in patients with pulmonary hypertension and cyanotic congenital heart disease such as tetralogy of Fallot).
Ankle-brachial index (ABI)
The ankle-brachial index (ABI) is the ratio of systolic blood pressure (BP) in the ankle to that in the arm. With the patient recumbent, the ankle blood pressure is measured in both the dorsalis pedis and posterior tibial artery, and the arm blood pressure is measured in both arms at the brachial artery. The index is calculated for each lower extremity by dividing the higher of the dorsalis pedis or posterior tibial pressure in that extremity by the higher of the 2 brachial artery systolic pressures. This ratio is normally > 1. A Doppler probe may be used to measure blood pressure at the ankle if the pedal pulses are not easily palpable.
A low (≤ 0.90) ankle-brachial index suggests peripheral arterial disease, which can be classified as mild (index 0.71 to 0.90), moderate (0.41 to 0.70), or severe (≤ 0.40). A high index (> 1.30) may indicate noncompressible leg vessels, as may occur in conditions that are associated with blood vessel calcification (eg, diabetes, end-stage renal disease, Mönckeberg arteriosclerosis). A high index may suggest that further vascular studies are needed (toe-brachial index or arterial duplex studies).
Orthostatic changes
Blood pressure and heart rate are measured with the patient supine, seated, and standing; a 1-minute interval is needed between each change in position. Orthostatic hypotension is typically defined as a decrease in systolic blood pressure of > 20 mm Hg or diastolic blood pressure > 10 mm Hg within 3 minutes of standing; the difference in blood pressure tends to be a little greater in older patients due to loss of vascular elasticity (4). The patient should be asked about symptoms of cerebral hypoperfusion, including lightheadedness or vision changes. However, the sensitivity of these measurements to detect hypovolemia (eg, secondary to blood loss) is low.
Causes of abnormal orthostatic vital signs include hypovolemia, baroreflex dysfunction (eg, due to neurodegenerative disorders such as autonomic neuropathies, peripheral neuropathies, older age) and, less commonly, valvular disease (eg, aortic stenosis), heart failure, or arrhythmias. Certain medications (eg, diuretics, vasodilators) can also contribute to abnormal orthostatic vital signs (5, 6).
Additionally, heart rate changes may be helpful to diagnosis various conditions. For example, an increase upon standing of ≥ 30 beats per minute (≥ 40 beats per minute in adolescents) compared to supine or sitting can indicate hypovolemia or postural orthostatic tachycardia syndrome (7).
Pulsus paradoxus
Normally during inspiration, systolic arterial blood pressure can decrease as much as 10 mm Hg. An exaggeration of this normal response with a greater decrease in systolic blood pressure or weakening of the pulse during inspiration is considered pulsus paradoxus. Pulsus paradoxus occurs in
Cardiac tamponade (commonly)
Chronic obstructive pulmonary disease (occasionally)
Severe asthma
Severe pulmonary embolism
Hypovolemic shock (rarely)
During inspiration, negative intrathoracic decreases LV preload and increased LV afterload, thus decreasing cardiac output and blood pressure. This mechanism (and the drop in systolic BP) is exaggerated in disorders that cause high negative intrathoracic pressure (eg, asthma) or that also restrict RV filling (eg, cardiac tamponade, cardiomyopathy) or outflow (eg, pulmonary embolism) (8).
Pulsus paradoxus is quantified by inflating a BP cuff to just above systolic BP and deflating it very slowly (eg, ≤ 2 mm Hg/heartbeat). The pressure is noted when Korotkoff sounds are first heard (at first, only during expiration) and when Korotkoff sounds are heard continuously. The difference between the pressures is the “amount” of pulsus paradoxus, and a difference of > 10 mm Hg is considered abnormal.
Vital signs references
1. Sheppard JP, Albasri A, Franssen M, et al: Defining the relationship between arm and leg blood pressure readings: a systematic review and meta-analysis. J Hypertens 37(4):660–670, 2019. doi:10.1097/HJH.0000000000001958
2. Whelton PK, Carey RM, Aronow WS, et al: 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 138(17):e484–e594, 2018. doi:10.1161/CIR.0000000000000596
3. Lena A, Ebner N, Anker MS: Cardiac cachexia. Eur Heart J Suppl 21 (Suppl L): L24–L27, 2019.
4. Shen WK, Sheldon RS, Benditt DG, et al: 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society [published correction appears in Circulation 2017 Oct 17;136(16):e271-e272. doi: 10.1161/CIR.0000000000000537]. Circulation 136(5):e60–e122, 2017. doi:10.1161/CIR.0000000000000499
5. Fedorowski A, Ricci F, Hamrefors V, et al: Orthostatic Hypotension: Management of a Complex, But Common, Medical Problem [published correction appears in Circ Arrhythm Electrophysiol 2023 Aug;16(8):478. doi: 10.1161/HAE.0000000000000088]. Circ Arrhythm Electrophysiol 15(3):e010573, 2023. doi:10.1161/CIRCEP.121.010573
6. Wieling W, Kaufmann H, Claydon VE, et al: Diagnosis and treatment of orthostatic hypotension. Lancet Neurol 21(8):735–746, 2022. doi:10.1016/S1474-4422(22)00169-7
7. Mar PL, Raj SR: Postural Orthostatic Tachycardia Syndrome: Mechanisms and New Therapies. Annu Rev Med 71:235-248, 2020. doi:10.1146/annurev-med-041818-011630
8. Spodick DH: The normal and diseased pericardium: current concepts of pericardial physiology, diagnosis and treatment. J Am Coll Cardiol 1(1):240–251, 1983. doi:10.1016/s0735-1097(83)80025-4
Pulses
Peripheral pulses
Major peripheral pulses in the arms and legs are palpated for symmetry and volume (intensity). Elasticity of the arterial wall is noted. Absence of pulses may suggest an arterial disorder (eg, atherosclerosis) or systemic embolism. Peripheral pulses may be difficult to feel in patients with obesity or in those who are muscular. In disorders with a rapid runoff of arterial blood (eg, arteriovenous communication, aortic regurgitation), the pulse has a rapid upstroke, then collapses. The pulse is rapid and bounding in hyperthyroidism and hypermetabolic states; it is slow and sluggish in hypothyroidism. If pulses are asymmetric, auscultation over peripheral vessels may detect a bruit due to stenosis.
Carotid pulses
Observation, palpation, and auscultation of both carotid pulses may suggest a specific disorder (see table ). Aging and arteriosclerosis lead to vessel rigidity, which tends to eliminate the characteristic findings. In very young children, the carotid pulse may be normal, even when severe aortic stenosis is present.
Auscultation over the carotid arteries can distinguish bruits from cardiac murmurs. Murmurs originate in the heart or great vessels and are usually louder over the upper precordium and diminish toward the neck. Bruits are higher-pitched, are heard only over the arteries, and seem more superficial. An arterial bruit must be distinguished from a venous hum. Unlike an arterial bruit, a venous hum is usually continuous, heard best with the patient sitting or standing, and is eliminated by compression of the ipsilateral internal jugular vein.
Carotid Pulse Amplitude and Associated Disorders
Carotid Pulse Amplitude | Associated Disorder |
|---|---|
Bifid (double-peaked) with normal or delayed rise | Combined aortic stenosis and aortic regurgitation |
Bounding and prominent | Disorders with a rapid rise and fall of pressure (eg, patent ductus arteriosus) Hypermetabolic states with increased stroke volume |
Diminished unilaterally or bilaterally, often with a systolic bruit | Extracranial carotid stenosis due to atherosclerosis |
Bifid with a rapid rise | |
Jerky, with full expansion followed by sudden collapse (Corrigan’s or water-hammer pulse) | |
Low in amplitude and volume with a delayed peak | Aortic stenosis (obstructing left ventricular outflow) |
Veins
Peripheral veins
The peripheral veins are observed for varicosities, arteriovenous malformations (AVMs), and shunts, and for overlying inflammation and tenderness due to thrombophlebitis. An AVM or a shunt produces a continuous murmur (heard on auscultation) and often a palpable thrill (because resistance is always lower in the vein than in the artery during systole and diastole).
Neck veins
The neck veins are examined to estimate venous wave height and waveform. Height is proportional to right atrial pressure, and waveform reflects events in the cardiac cycle; both are best observed in the internal jugular vein.
The jugular veins are usually examined with the patient reclining at 45°. The top of the venous column is normally just above the clavicles (upper limit of normal: 4 cm above the sternal notch in a vertical plane) (1). The venous column is elevated in right heart failure, intravascular volume overload, cardiac tamponade, constrictive pericarditis, tricuspid stenosis, tricuspid regurgitation, superior vena cava obstruction, or reduced compliance of the right ventricle. If such conditions are severe, the venous column can extend to jaw level, and its top can be detected only when the patient sits upright or stands. The venous column is low in hypovolemia.


DR P. MARAZZI/SCIENCE PHOTO LIBRARY
Normally, the venous column can be briefly elevated by firm hand pressure on the abdomen (hepatojugular or abdominojugular reflux); the column falls back in a few seconds (maximum 3 respiratory cycles or 15 seconds) despite continued abdominal pressure (because a compliant RV increases its stroke volume via the Frank-Starling mechanism). However, the column remains elevated (> 3 cm) during abdominal pressure in disorders that cause a dilated and poorly compliant RV or in obstruction of RV filling by tricuspid stenosis or right atrial tumor.
Normally, the venous column falls slightly during inspiration as lowered intrathoracic pressure draws blood from the periphery into the vena cava. A rise in the venous column during inspiration (Kussmaul sign) occurs typically in chronic constrictive pericarditis, right ventricular myocardial infarction, and chronic obstructive pulmonary disease (COPD), and can also occur in heart failure and tricuspid stenosis.
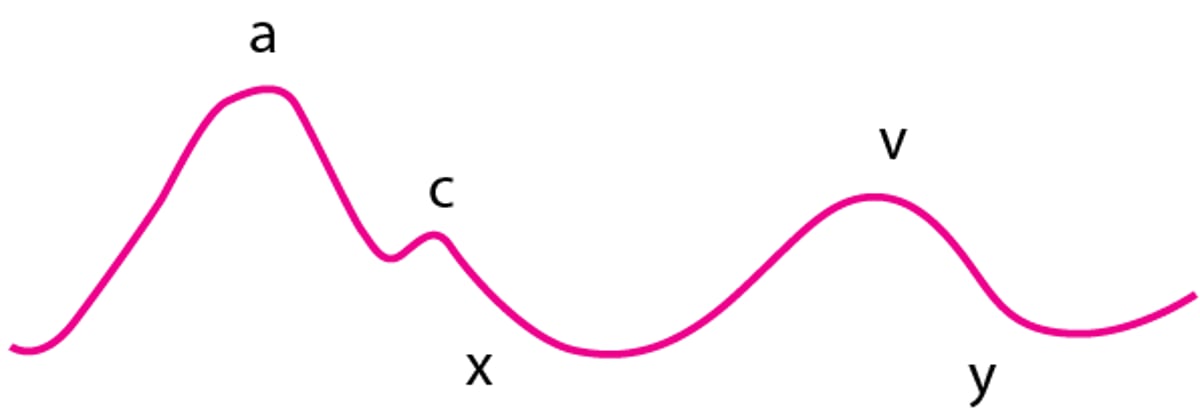
Jugular vein waves (see figure ) can usually be discerned clinically but are better seen on the screen during central venous pressure monitoring (2).
Normal Jugular Vein Waves
The a wave is caused by right atrial contraction (systole) and is followed by the x descent, which is caused by atrial relaxation. The c wave, an interruption of the x descent, is caused by the transmitted carotid pulse; it is seldom discerned clinically. The v wave is caused by right atrial filling during ventricular systole (tricuspid valve is closed). The y descent is caused by rapid filling of the right ventricle during ventricular diastole before atrial contraction. |

The a waves are increased in pulmonary hypertension and tricuspid valve stenosis. Giant a waves (Cannon waves) occur in atrioventricular dissociation when the atrium contracts while the tricuspid valve is closed. The a waves disappear in atrial fibrillation and are accentuated when RV compliance is poor (eg, in pulmonary hypertension or pulmonic stenosis). The v waves are very prominent in tricuspid regurgitation. The x descent is steep in cardiac tamponade. When RV compliance is poor, the y descent is very abrupt because the elevated column of venous blood rushes into the RV when the tricuspid valve opens, only to be stopped abruptly by the rigid RV wall (in restrictive cardiomyopathy) or the pericardium (in constrictive pericarditis).
Veins references
1. Sinisalo J, Rapola J, Rossinen J, Kupari M: Simplifying the estimation of jugular venous pressure. Am J Cardiol 100(12):1779–1781, 2007. doi:10.1016/j.amjcard.2007.07.030
2. Devine PJ, Sullenberger LE, Bellin DA, Atwood JE: Jugular venous pulse: window into the right heart. South Med J 100(10):1022–1004, 2007. doi:10.1097/SMJ.0b013e318073c89c
Chest Inspection and Palpation
Chest contour and any visible cardiac impulses are inspected. The precordium is palpated for pulsations (determining apical impulse and thus cardiac situs) and thrills.
Inspection
Chest wall deformities may occur in a number of disorders.
Pectus carinatum (a prominent birdlike sternum) may be associated with Marfan syndrome (which may be accompanied by aortic root or mitral valve disease) or Noonan syndrome (which may be accompanied by pulmonic stenosis, atrial septal defects, or hypertrophic cardiomyopathy). Rarely, a localized upper chest bulge indicates aortic aneurysm due to syphilis.
Pectus excavatum (depressed sternum) with a narrow anteroposterior chest diameter and an abnormally straight thoracic spine may be associated with hereditary disorders involving congenital cardiac defects (eg, Turner syndrome, Noonan syndrome) and sometimes Marfan syndrome.


DR P. MARAZZI / SCIENCE PHOTO LIBRARY
Shield chest is a broad chest with widely spaced nipples, often associated with Turner syndrome.


By permission of the publisher. From Shulman D, Bercu B: Atlas of Clinical Endocrinology: Neuroendocrinology and Pituitary Disease. Edited by S Korenman (series editor) and ME Molitch. Philadelphia, Current Medicine, 2000.
Palpation
The patient lays at approximately a 30 to 45° angle. Approaching the patient from the right side, the clinician systematically palpates the precordium.
The apical impulse in healthy individuals should be palpable between the fourth and fifth intercostal space just medial to the midclavicular line and cover an area < 2 to 3 cm in diameter.
A central precordial heave, also called a parasternal heave or lift, is a palpable lifting sensation under the sternum and anterior chest wall to the left of the sternum; it suggests significant right ventricular hypertrophy or dilation. Occasionally, in congenital disorders that cause severe RV hypertrophy, the precordium visibly bulges asymmetrically to the left of the sternum.
A sustained thrust at the apex (easily differentiated from the less focal, somewhat diffuse precordial heave of RV hypertrophy) suggests LV hypertrophy.
Abnormal focal systolic impulses in the precordium can sometimes be felt in patients with a dyskinetic ventricular aneurysm. An abnormal diffuse systolic impulse lifts the precordium in patients with severe mitral regurgitation. The lift occurs because the left atrium expands, causing anterior cardiac displacement. A diffuse and inferolaterally displaced apical impulse is found when the LV is dilated and hypertrophied (eg, in mitral regurgitation).
Thrills are a palpable buzzing sensation present with particularly loud murmurs. Their location suggests the cause (see table ).
Location of Thrills and Associated Disorder
Location of Thrill | Associated Disorder |
|---|---|
Over the base of the heart at the second intercostal space, just to the right of the sternum, during systole | |
At the apex during systole | |
To the left of the sternum at the second intercostal space | |
To the left of the sternum at the fourth intercostal space | Small muscular ventricular septal defect (Roger disease) |
A sharp impulse at the second intercostal space to the left of the sternum may result from exaggerated pulmonic valve closure in pulmonary hypertension. A similar early systolic impulse at the cardiac apex may represent closure of a stenotic mitral valve; opening of the stenotic valve sometimes can be felt at the beginning of diastole. These findings coincide with an augmented first heart sound (S1) and an opening snap of mitral stenosis, heard on auscultation.
Lung Examination
The lungs are examined for signs of pleural effusion and pulmonary edema, which may occur with cardiac disease such as heart failure. The lung examination includes percussion, palpation, and auscultation (1).
Percussion is the primary physical maneuver used to detect the presence and level of pleural effusion. Finding areas of dullness during percussion signifies underlying fluid or, less commonly, consolidation.
Palpation includes tactile fremitus (vibration of the chest wall felt while a patient is speaking); fremitus is decreased in pleural effusion and pneumothorax and increased in pulmonary consolidation (eg, lobar pneumonias).
Auscultation of the lungs is an important component of the examination of patients with suspected cardiac disease.
The character and volume of breath sounds are useful in differentiating cardiac from pulmonary disorders. Adventitious sounds are abnormal sounds, such as crackles, rhonchi, wheezes, and stridor. Crackles (previously called rales) and wheezes are abnormal lung sounds that may occur in heart failure as well as non-cardiac diseases.
Crackles are discontinuous adventitious breath sounds. Fine crackles are short high-pitched sounds; coarse crackles are longer-lasting low-pitched sounds. Crackles have been compared to the sound of crinkling plastic wrap and can be simulated by rubbing strands of hair together between 2 fingers near one’s ear. They occur most commonly with atelectasis, alveolar filling processes (eg, pulmonary edema in heart failure), and interstitial lung disease (eg, pulmonary fibrosis); they signify opening of collapsed airways or alveoli.
Wheezes are whistling, musical breath sounds that are worse during expiration than inspiration. Wheezing can be a physical finding or a symptom and is usually associated with dyspnea. Wheezes occur most commonly with asthma but can also occur in cardiac disease such as heart failure, or when posterior structures such as the left atrium or pulmonary artery branches become dilated and compress the airways.

Lung examination reference
1. Mootz WC, Matuschak GM: Chapter 14. Conduct and Interpretation of the Basic Chest Examination. In Lechner AJ, Matuschak GM, Brink DS (eds): Respiratory: An Integrated Approach to Disease. New York, McGraw-Hill, 2012.
Abdominal and Extremity Examination
The abdomen and extremities are examined for signs of fluid overload, which may occur with heart failure as well as noncardiac disorders (eg, renal, hepatic, lymphatic).
Abdomen
In the abdomen, significant fluid overload manifests as ascites. Marked ascites causes visible abdominal distention, which is tense and nontender to palpation, with shifting dullness on abdominal percussion and a fluid wave. The liver may be distended and slightly tender, with a hepatojugular reflux present.
Extremities
In the extremities (primarily the legs), fluid overload is manifest as edema, which is swelling of soft tissues due to increased interstitial fluid. Edema may be visible on inspection, but modest amounts of edema in patients who are very obese or muscular may be difficult to recognize visually. Thus, extremities are palpated for presence and degree of pitting (visible and palpable depressions caused by pressure from the examiner’s fingers, which displaces the interstitial fluid). The area of edema is examined for extent, symmetry (ie, comparing both extremities), warmth, erythema, and tenderness. With significant fluid overload, edema may also be present over the sacrum, genitals, or both. Pitting edema is graded on a scale of 1 to 4, but there is no agreed-upon definition for these grades.
Tenderness, erythema, or both, particularly when unilateral, suggests an inflammatory cause (eg, cellulitis or thrombophlebitis). Nonpitting edema is more suggestive of lymphatic or vascular obstruction than fluid overload.
Point-of-Care Ultrasound (POCUS)
(See also Echocardiography.)
Cardiac point-of-care ultrasound (POCUS), also called focused cardiac ultrasound (FoCUS), is a complement to the physical examination that uses small, inexpensive, portable ultrasound devices operated by the treating clinician at the bedside. Both 2-dimensional and color Doppler techniques can be used. A brief, focused ultrasound examination can improve detection of various cardiac anomalies and confirm findings from physical examination or sometimes make a diagnosis in the absence of physical findings. Common uses include identification of (1, 2, 3):
Left ventricular systolic dysfunction (with global or regional wall motion abnormality)
Left ventricular regional wall motion abnormality (with reduced or normal systolic function)
Elevated left heart filling pressures (enlarged left atrium)
Valvular abnormalities
Pulmonary edema (vertical B-lines in the lung fields)
Pleural effusion
Systemic venous congestion (dilated inferior vena cava)
Pericardial effusion and cardiac tamponade
Adequate training in doing brief ultrasound examinations is essential to ensure high image quality and accurate interpretation (2). Importantly, POCUS should be used to augment rather than replace the physical examination; neither does it replace complete echocardiography when that is indicated.
Point-of-care ultrasound references
1. Kimura BJ: Point-of-care cardiac ultrasound techniques in the physical examination: better at the bedside. Heart 103:987–994, 2017. doi: 10.1136/heartjnl-2016-309915
2. Spencer KT, Kimura BJ, Korcarz CE, et al: Focused Cardiac Ultrasound: Recommendations from the American Society of Echocardiography. J Am Soc Echocardiogr 26:567–581, 2013. doi: 10.1016/j.echo.2013.04.001
3. Kirkpatrick JN, Panebianco N, Díaz-Gómez JL, et al: Recommendations for Cardiac Point-of-Care Ultrasound Nomenclature. J Am Soc Echocardiogr July 11:S0894-7317(24)00222-0, 2024 doi:10.1016/j.echo.2024.05.001





