



")





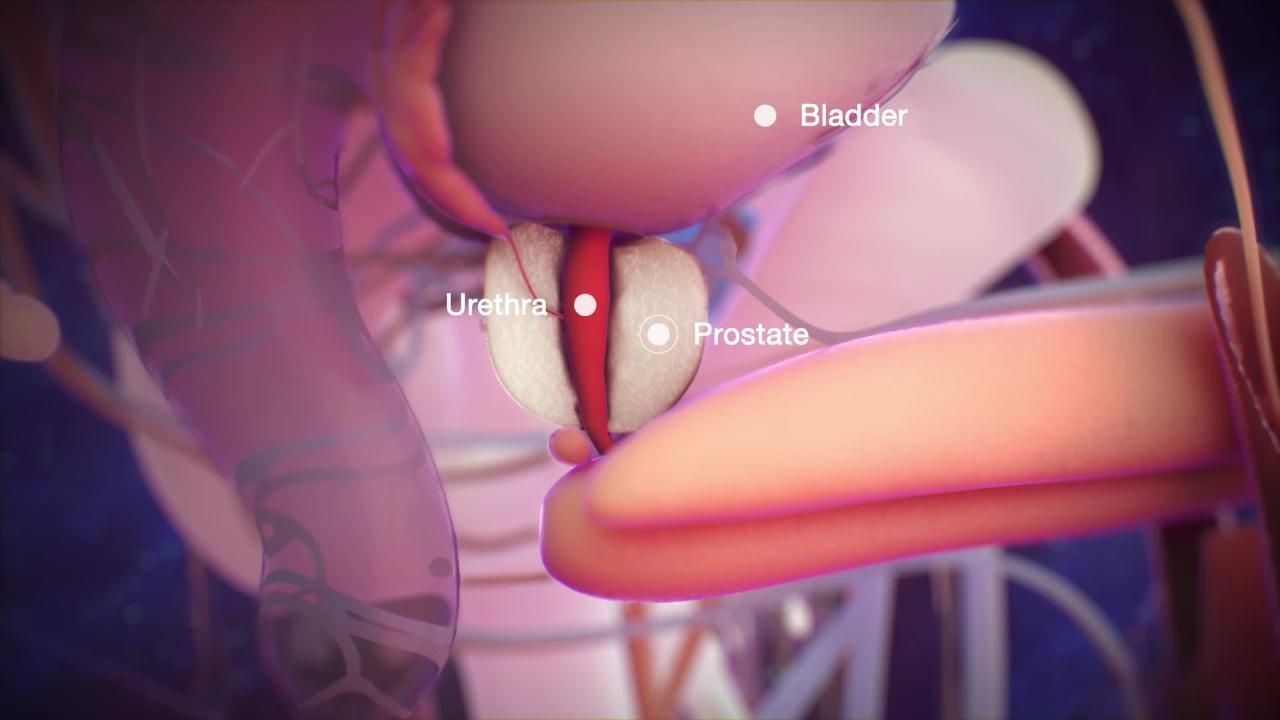
Prostate cancer begins in the prostate gland, an organ found only in males.
The risk of prostate cancer increases as men age.
Symptoms, such as difficulty urinating, a need to urinate frequently and urgently, and blood in the urine, usually occur only after the cancer is advanced.
The cancer can spread, most commonly to bones and lymph nodes.
Doctors may do a digital rectal examination to examine the prostate using a gloved finger in the rectum and a blood test (PSA) to check for prostate cancer in men without symptoms.
If cancer is suspected, imaging and a biopsy of prostate tissue are done.
Treatment may involve active surveillance, removal of the prostate gland, radiation therapy, or hormonal or newer medications to slow cancer growth.
Among men in the United States, prostate cancer is the most common cancer and 1 of the most common causes of cancer death. Every year, more than 299,010 new cases are diagnosed and 35,250 people die of prostate cancer (2024 estimates). The chance of developing prostate cancer increases with age and is greater for
Men who are Black, particularly those from the Caribbean
Men whose close relatives had the disease
Men who have relatives with other cancers such as breast or ovarian cancer
Prostate cancer usually grows very slowly and may take decades to cause symptoms. Thus, particularly because it occurs more often in older men, far more men have prostate cancer than die from it. Many men with prostate cancer die from other causes without ever knowing that they had prostate cancer. Some prostate cancers, however, grow rapidly or spread outside the prostate.

The cause of prostate cancer is not known.
Symptoms of Prostate Cancer
Prostate cancer usually causes no symptoms until it reaches an advanced stage. Sometimes, symptoms similar to those of benign prostatic hyperplasia (BPH) develop, including difficulty urinating and a need to urinate frequently or urgently. However, these symptoms do not develop until after the cancer grows large enough to compress the urethra and partially block the flow of urine. Later, prostate cancer may cause bloody urine or a sudden inability to urinate.
In some men, symptoms of prostate cancer develop only after it spreads (metastasizes). The areas most often affected by cancer spread are bones (typically the pelvis, ribs, or vertebrae). Bone metastasis tends to be painful and may weaken a bone enough for it to easily fracture. Spread to the bones of the spine (vertebrae) affects the spinal cord and can cause pain, numbness, weakness, or urinary incontinence. After the cancer spreads, anemia is common.
Did You Know...
|
Diagnosis of Prostate Cancer
Screening blood tests (with or without a digital rectal examination [DRE])
Biopsy
Imaging tests
Doctors may suspect prostate cancer based on the symptoms, the results of DRE, or the results of screening blood tests. The most commonly used screening blood test is a measurement of the prostate-specific antigen (PSA) level. PSA is a substance produced only by prostate gland tissue.
In some men, doctors recommend an MRI that focuses on the prostate to obtain detailed images that could indicate more aggressive cancer. The radiologist reading the MRI identifies abnormal areas that may help doctors choose which areas to biopsy (the MRI does not make biopsy unnecessary).
If results of these tests suggest cancer, ultrasound imaging is usually done. In men with prostate cancer, an ultrasound may or may not reveal the cancer but is used to guide biopsy of the prostate.

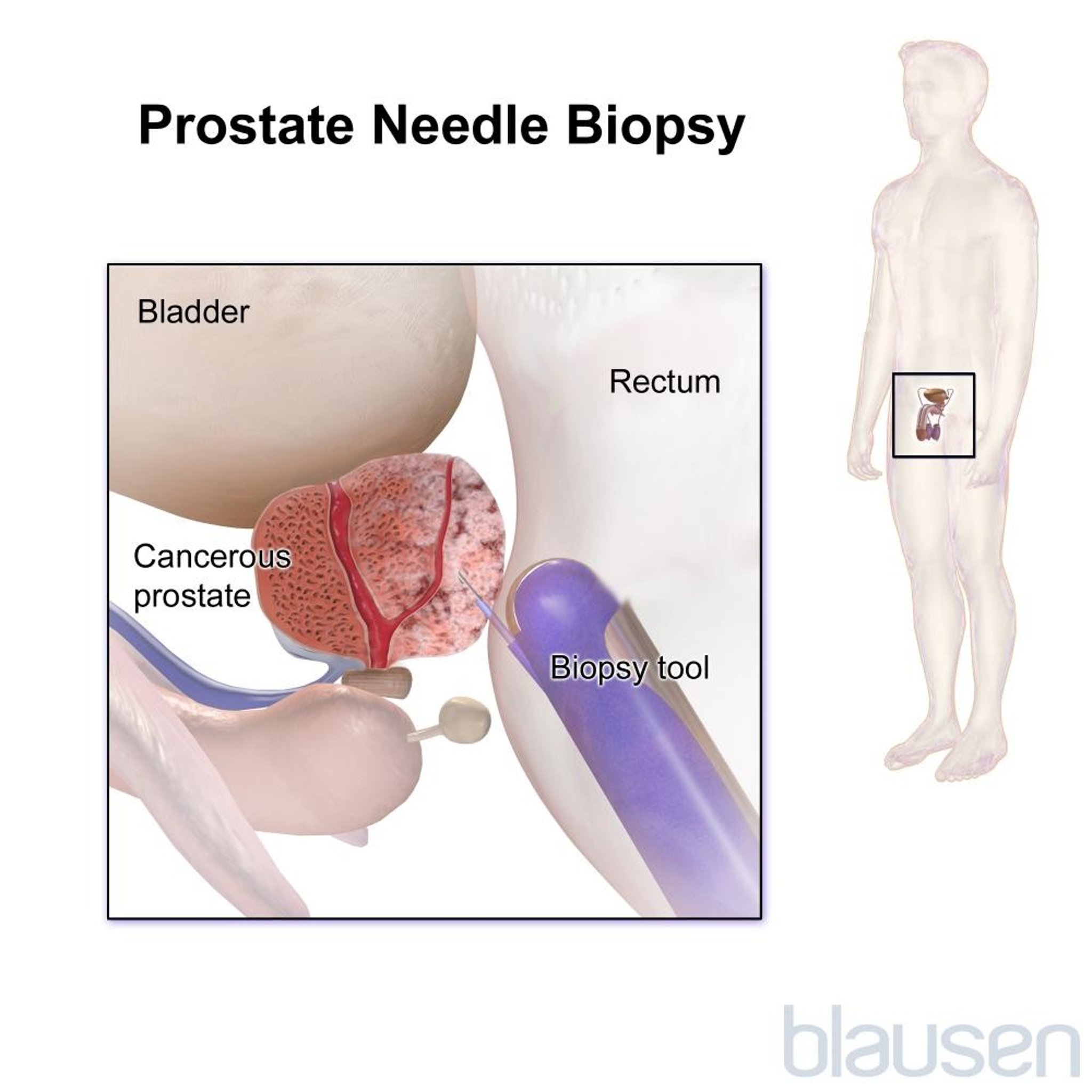
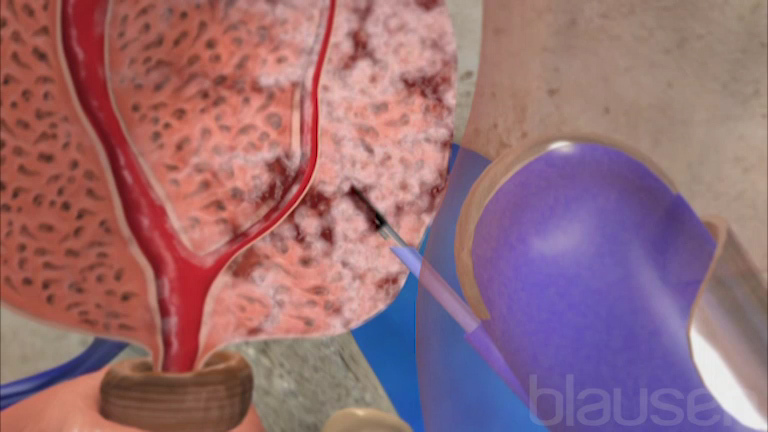
If the results of a digital rectal examination or PSA test suggest prostate cancer, tissue samples from the prostate are taken and analyzed (biopsy). When doing a biopsy, doctors usually first obtain images of the prostate by inserting an ultrasound probe (transducer) into the rectum (transrectal ultrasonography). The biopsy sample may be obtained through the rectal probe or through the skin between the rectum and the scrotum (transperineally). Usually, 10 to 12 samples are taken from the prostate. Taking many samples increases the likelihood of finding a small cancer. This procedure takes about 20 minutes, and men are usually given local anesthesia.
If cancer is found in the biopsy sample, grading and staging of the tissue help doctors determine the likely course and the best treatment of the cancer.
Grading
The Gleason Grade Group system is the most common way to grade prostate cancer (previously the Gleason Scoring system was used). Based on the microscopic examination of tissues obtained from the biopsy, a number is assigned based on how distorted the cells appear. The current version of this scoring system gives each cancer a grade between 1 and 5, while the older Gleason Scoring system assigned a score between 6 and 10. The higher the number (high grade), the more aggressive the cancer is and the more likely it is that the cancer will spread.
Gleason Grade Group 1 = Gleason Score 6 (3+3)
Gleason Grade Group 2 = Gleason Score 7 (3+4)
Gleason Grade Group 3 = Gleason Score 7 (4+3)
Gleason Grade Group 4 = Gleason Score 8
Gleason Grade Group 5 = Gleason Score 9 and 10
Gleason Grade, PSA level, and clinical stage together predict the prognosis better than any of them alone and help guide appropriate treatment decisions.
Staging
Prostate cancers are staged according to 3 criteria:
How far the cancer has spread within the prostate
Whether the cancer has spread to lymph nodes in areas near the prostate
Whether the cancer has spread to bones or other organs far from the prostate (metastatic cancer)
Testing to stage the cancer is often done when cancer is diagnosed. However, such testing may not be necessary when the likelihood of spread beyond the prostate is extremely low. Likelihood of spread is low when cancers have a Grade Group of 2 or less, the PSA level is less than 10 ng/mL (10 mcg/L), and the cancer has not penetrated the surface of the gland. Results of the digital rectal examination, ultrasound imaging, and biopsy reveal how far the cancer has spread within the prostate.
If the likelihood of spread is not low, doctors usually do computed tomography (CT) or magnetic resonance imaging (MRI) of the abdomen and pelvis. Sometimes an MRI of the prostate is done using a special coil inserted into the rectum. A nuclear medicine (NM) bone scan may be done in people who have pain in their bones or who have a very high prostate-specific antigen (PSA) or high Gleason Grade Group.
If spread to the brain or spinal cord is suspected, CT or MRI of those organs is done.
Screening for Prostate Cancer
Because prostate cancer is common and sometimes fatal, and because symptoms may not develop until the cancer has become advanced, many doctors offer screening tests to men with no symptoms.
To screen for prostate cancer, doctors do a blood test to measure prostate-specific antigen (PSA) levels. If the PSA level is elevated, prostate cancer is more likely. However, PSA levels can be misleading. The PSA level can be normal when prostate cancer is present and can be elevated for reasons other than prostate cancer. PSA levels normally increase with age and with disorders such as benign prostatic hyperplasia and prostatitis.
Screening has the advantage of finding aggressive cancers early—when they might be cured. However, experts disagree about whether and when screening is helpful for a variety of reasons:
Screening tests may be positive in many men who do not have cancer.
Some prostate cancers grow so slowly that they may not require treatment.
Rarely, some more aggressive cancers may not be detected by standard PSA testing.
Screening using the PSA blood test is considered in all men older than 45 and in some who are younger who have risk factors, such as being Black, having a family history of prostate cancer, or having a specific genetic mutation. Benefits of screening may decrease with age. The United States Preventive Services Task Force recommendations indicate that men aged 45 to 75 should discuss with their doctor the benefits versus harms of screening with the PSA blood test.
Screening may find cancers that would probably not hurt or kill a man even if they were never detected. In such cancers, the side effects of treatment (for example, erectile dysfunction or urinary incontinence) can be more damaging than leaving the cancer untreated. Because it is not always clear early on which prostate cancers will be aggressive (for example, for cancers with low Gleason Grade Group and that involve only a small part of the prostate), doctors had historically recommended treatment to all men whose biopsy showed cancer. Thus, many more men were treated for prostate cancer than would have died or had serious complications from the cancer. As a result, many of the men treated derived no benefit from treatment but still risked side effects. However, more recently, as the understanding of prostate cancer has improved, doctors now offer certain men with a positive biopsy the option of close monitoring (active surveillance), delaying treatment until results of periodic checkups and tests indicate the need for treatment (for example, that the cancer is enlarging or becoming more aggressive).
Because the best course of action is still not clear and because men may have different values and preferences, the harms and benefits of screening, biopsy, and treatment should be discussed with their doctor. For example, men who would rather risk a substantial likelihood of side effects resulting from treatment than even a very small risk of death caused by a prostate cancer may choose to be screened. Men who would not want to risk the side effects of treatment unless it was absolutely necessary may choose not to be screened.
Treatment of Prostate Cancer
Surgery
Radiation therapy
Hormonal therapy
Active surveillance
Choosing among treatment options can be complicated. Because studies have not directly compared 1 treatment to another, doctors may be uncertain which treatment is most effective. Furthermore, for some men, doctors are not sure whether treatment will prolong life. Such men include those who are not expected to live very long (either because of old age or serious health problems) and those with low prostate-specific antigen (PSA) levels who have low-grade cancer confined to the prostate. Men who are not expected to live very long often make their decision by balancing their degree of discomfort in living with a cancer against the possible side effects of treatment. Men with low PSA who have low-grade cancer confined to the prostate also need to balance the benefit of treating a cancer that might not harm them against the possible side effects of treatment. Surgery, radiation therapy, and hormonal therapy may cause incontinence, erectile dysfunction (impotence), or other problems. For all of these reasons, men’s preferences are a bigger consideration in choosing treatment for prostate cancer than they are for many other disorders.
Strategies for treatment
Treatment for prostate cancer usually involves 1 of 3 strategies based on the aggressiveness of the cancer and how far the cancer has spread:
Active surveillance
Curative treatment
Palliative treatment
Active surveillance means doctors give no treatment unless the cancer is progressing or changing. The advantage of this strategy is avoiding or postponing the potential side effects of treatment. Active surveillance should be considered for men whose cancers are unlikely to spread or cause symptoms. For example, most cancers that are confined to a small area within the prostate and have low Gleason Grade Group grow very slowly. Thus, older men, particularly those who have other serious health problems, are far more likely to die of other causes before such cancers kill them or cause symptoms. In younger men, particularly those who are healthy, even a slow-growing cancer may eventually cause problems. In such men, active surveillance may be less preferred but should still be considered. During active surveillance, doctors periodically ask about symptoms, measure the PSA level, do digital rectal examinations, and repeat biopsies (with or without MRI guidance) to determine whether the cancer is causing symptoms, growing rapidly, or spreading. If testing shows growth or spread, doctors offer curative or palliative treatment.
Curative treatment aims to remove or kill all of the cancer and includes
Surgery
Radiation therapy
Less often, focal therapy (an imaging-guided technique for directly destroying the cancerous tissue with either lasers, electricity, or high-frequency ultrasound)
Cryotherapy (freezing)
Curative (also called definitive) treatment is a common strategy for men with cancers confined to the prostate that are likely to cause troublesome symptoms or death. Such cancers include those that are growing rapidly as well as some small, slowly growing cancers in men who are likely to live for some time (perhaps at least 10 or 15 years). Such men are typically those who are healthy, younger (particularly those under 60), or both. Curative treatment is not pursued if cancer has spread widely, but it can benefit some men with cancers that have spread to the area just outside the prostate. Such cancers are likely to cause symptoms within a relatively short period. However, curative treatment is most likely to be successful with cancers that are still confined to the area near the prostate. Curative treatment can prolong life and reduce or eliminate severe symptoms resulting from some cancers. Side effects, although less common with newer treatments, can still develop and diminish quality of life. These can include, for example, erectile dysfunction and, less often, urinary incontinence (most often as a result of surgery) and pain or bleeding during defecation and irritation or bleeding when urinating (as a result of radiation therapy).
Palliative treatment aims to treat the symptoms rather than cure the cancer. Palliative therapies include
Hormonal therapy
Chemotherapy
Radiation therapy
Palliative treatment is best suited to men with widespread prostate cancer, which is not curable. The growth or spread of such cancers can usually be slowed or temporarily reversed, relieving symptoms. Besides trying to slow the cancer’s growth and spread, doctors may try to relieve symptoms resulting from the effects of cancer in other organs and tissues (such as the bones). However, because these treatments cannot cure the cancer, symptoms eventually worsen. Death due to the disease eventually follows.
Surgery
Surgically removing the prostate (prostatectomy) is useful for cancer that is confined to the prostate. Prostatectomy is usually not done if staging tests show the cancer has spread. Prostatectomy is very effective in curing low-grade, slowly growing cancers but is less effective in high-grade, fast-growing cancers. Such cancers are more likely to have spread even if spread is not detectable with staging tests at the time of diagnosis.
Prostatectomy requires general or spinal anesthesia, an overnight hospital stay, and a surgical incision. Following surgery, men must have a catheter in their penis for a week or 2 until the connection between the bladder and urethra heals. Doctors do not routinely give chemotherapy or hormone therapy before or after surgery. In men whose prostate cancer is found to be aggressive (high grade, fast growing) at the time of surgery and whose PSA increases, consideration is given to radiation therapy (with hormone therapy) after surgery.
Prostatectomy may lead to permanent erectile dysfunction and urinary incontinence. Erectile dysfunction may occur because the nerves to the penis that control erection run across the prostate and may be damaged during surgery. Incontinence may occur—and potentially be long term—because part of the sphincter that closes the opening at the bottom of the bladder must be removed during surgery. However, most men recover continence within 6 months following prostatectomy. Erectile function recovery is more variable, depending in part on men's erectile function prior to surgery, the aggressiveness of the prostate cancer, and the surgical technique.
Techniques for doing prostatectomy include open radical prostatectomy and laparoscopic or robot-assisted radical prostatectomy. In open radical prostatectomy, the entire prostate, the seminal vesicles, and part of the vas deferens are removed through an incision in the lower abdomen or, rarely, in the area between the scrotum and anus. Lymph nodes may also be removed to check for cancer. In laparoscopic or robot-assisted laparoscopic radical prostatectomy, the same structures are removed, but these procedures are done through smaller incisions and result in less postoperative pain and blood loss and typically a faster recovery.
Radical prostatectomy, irrespective of technique, is the surgery done when trying to cure prostate cancer. More than 90% of men with cancer confined to the prostate live at least 10 years after radical prostatectomy. Younger men who can otherwise expect to live at least 10 to 15 more years are most likely to benefit from radical prostatectomy. However, the procedure causes some leakage of urine in up to 10% of men. Temporary incontinence develops in most men and may last for several months. Incontinence is less likely in younger men.
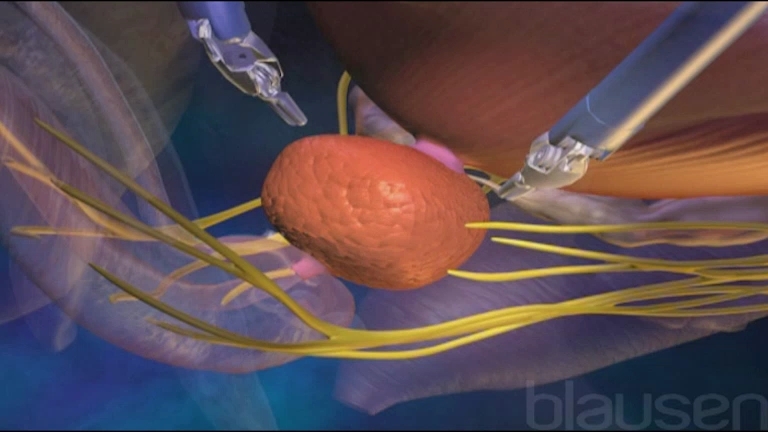
A degree of erectile dysfunction develops in most men after radical prostatectomy, particularly in those who experienced difficulty with erections before surgery. Usually prostatectomy can be done in such a way that some of the nerves needed to achieve erection are spared—this procedure is called nerve-sparing radical prostatectomy. This procedure cannot be used to treat cancer that has invaded the nerves and blood vessels of the prostate. Nerve-sparing radical prostatectomy is less likely than non–nerve-sparing radical prostatectomy to cause erectile dysfunction. Most men are diagnosed early and, thus, can be treated with nerve-sparing radical prostatectomy.
Blockage of urine flow caused by narrowing of part of the bladder or scarring of the urethra (urethral stricture) develops in 7 to 20% of men. Blockage can usually be easily treated (see Urinary Tract Obstruction: Treatment).
Radiation therapy
Radiation therapy may cure cancers that are confined to the prostate, as well as cancers that have invaded tissues around the prostate. Although radiation therapy cannot cure cancer that has spread to distant organs, it can help relieve the pain resulting from the spread of prostate cancer to bone.
Doctors sometimes give radiation therapy after surgery to treat the areas around the prostate or if PSA is found in the blood after surgery. PSA in the blood after surgery suggests that surgery has not removed all of the cancer.
For many stages of prostate cancer, 10-year survival rates after radiation therapy are nearly as high as those achieved with surgery. More than 90% of men with cancer confined to the prostate live at least 10 years after undergoing radiation therapy. Radiation therapy can be delivered as
External beam radiation therapy (used to treat cancer within the prostate gland and prostate cancer that has spread to bone)
Radioactive implants (used to treat low-risk cancer within the prostate gland but not prostate cancer that has spread to bone)
Radium-223 (an intravenous agent used to treat prostate cancer that has spread to bone, but not cancer within the prostate gland)
External beam radiation therapy uses a machine to send beams of radiation to the prostate and surrounding tissues. Computed tomography (CT) is often used to help focus the radiation beams more precisely on the cancer by precisely identifying the structures affected. This approach is called 3-dimensional conformal radiation therapy. Treatments are usually given 5 days per week for 7 to 8 weeks. Although some degree of erectile dysfunction can occur in up to 40% of men, it is less likely to develop during the period soon after radiation therapy than during the period soon after prostatectomy. However, after months or years, erectile dysfunction seems to be as likely after radiation therapy as after prostatectomy. Incontinence is rare when 3-dimensional conformal radiation therapy is used. IMRT (intensity-modulated radiation therapy) and SBRT (stereotactic body radiation therapy) are modifications of standard radiation therapy. Sometimes, for more aggressive cancers, doctors also give hormonal therapy for up to 2 or 3 years in addition to the radiation therapy.
Scars that narrow the urethra and impede the flow of urine (urethral strictures) develop in about 5 to 10% of men treated with external beam radiation therapy. Other troublesome but usually temporary side effects include burning during urination, having to urinate frequently, blood in the urine, diarrhea that is sometimes bloody, radiation proctitis (usually causing irritation of the rectum and diarrhea), and sudden urges to defecate. Rarely, men develop cancers in the surrounding organs (bladder, rectum) caused by radiation therapy.
A different form of external beam radiation therapy is proton beam therapy, which uses a different form of radiation that allows the radiation to be delivered more precisely to cancer cells while avoiding healthy cells. Proton beam therapy has been shown to be beneficial for other cancers, but it is not clear if it has fewer side effects in prostate cancer than standard external beam radiation therapy.
Recent advances in prostate cancer radiation therapy include
Placing markers around the prostate to improve targeting
Using a transrectal needle to place hydrogel spacers in the rectum to reduce radiation's toxic effects (these hydrogel spacers eventually break down and are resorbed into the tissues)
Dividing large doses of radiation up over time and administering them over a shorter period (fewer days or weeks) than traditional radiation
Radioactive implants can be inserted into the prostate (brachytherapy). The implants are small, seedlike pieces of radioactive material. Doctors inject the implants into the prostate gland through the area between the scrotum and anus using ultrasound imaging or CT to guide placement. Brachytherapy can be done in less than 2 hours, does not require repeated treatment sessions, and can be done using spinal anesthesia. Brachytherapy also can deliver high doses of radiation to the prostate while often sparing healthy surrounding tissues and causing fewer side effects. However, brachytherapy may cause urethral strictures in up to 10% of men. The radioactivity of the seeds decreases with time. Seeds may later be passed in the urine. Men treated with these seeds should avoid close contact with pregnant women and young children for a period of time after the procedure because the radioactivity can be harmful to a fetus or young child. Cure rates 10 to 15 years after brachytherapy are similar to rates obtained with other treatments for some men. Combined treatment with brachytherapy and external beam radiation therapy is sometimes recommended for more aggressive cancers. Temporary brachytherapy implants (requiring an overnight hospital stay) are available at some centers.
Radium-223 is a drug given intravenously that emits a particular type of radiation (alpha radiation). Unlike beam radiation and brachytherapy, it is not directed at a particular target. Radium-223 is used to treat bone metastases from prostate cancer rather than the prostate cancer in the prostate gland. Once in the bloodstream, radium-223 seeks out areas of bone affected by prostate cancer, where it helps destroy cancer cells. Because it targets bone tissue and does not scatter radiation (like radiation beams or seeds), it may spare nearby tissues from radiation damage.
Focal therapies
Focal therapies use imaging-guided techniques to deliver different treatments to cancerous areas in the prostate.
High-intensity focused ultrasound (HIFU) uses intense ultrasound energy administered through a probe placed in the rectum to destroy prostate tissue. It has been used for many years in Europe and Canada and has recently become more widely available in the United States. The role of this technology in the management of prostate cancer is still evolving. HIFU is best suited for treating prostate cancer that recurs after surgery as well as localized low-risk cancers.
Electroporation is another form of focal therapy. This imaging-guided technique uses either lasers or electricity to directly destroy cancer cells while sparing the surrounding tissue. Tiny needles are placed through the skin between the rectum and the scrotum (transperineally) into the areas of prostate cancer. Electricity or laser beams are then pulsed through those needles to destroy the cancer cells.
Cryotherapy is the destruction of prostate cancer cells by freezing, which is accomplished by using a cryoprobe to deliver argon gas to the cancerous tissue, followed by thawing. Cryotherapy is not the therapy of choice in the United States, but it may be used if radiation therapy is unsuccessful. Side effects of the procedure include blockage of urinary flow from the bladder (bladder outlet obstruction), urinary incontinence, erectile dysfunction, and rectal pain or injury.
Hormonal therapy
Because most prostate cancers require testosterone to grow or spread, treatments that block the effects of this hormone (hormonal therapy) can slow progression of the tumors. Hormonal therapy is commonly used to delay the spread of the cancer that has come back after surgery or radiation therapy or to treat widespread (metastatic) prostate cancer. Hormonal therapy is sometimes combined with other treatments such as radiation therapy. Hormonal therapy is not curative on its own but can prolong life as well as decrease symptoms. Eventually, however, hormonal therapy is likely to lose effectiveness, and the disease progresses.
Hormonal medications used to treat prostate cancer in the United States include leuprolide, goserelin, triptorelin, buserelin, histrelin, degarelix, and relugolix, which prevent the pituitary gland from stimulating the testes to make Hormonal medications used to treat prostate cancer in the United States include leuprolide, goserelin, triptorelin, buserelin, histrelin, degarelix, and relugolix, which prevent the pituitary gland from stimulating the testes to maketestosterone. Except for relugolix (given by mouth), these medications are given by injection in a doctor’s office every 1, 3, 4, or 12 months, usually for the rest of the man’s life. For some men, this treatment may only be given for a year or 2 and possibly resumed at a later time.. Except for relugolix (given by mouth), these medications are given by injection in a doctor’s office every 1, 3, 4, or 12 months, usually for the rest of the man’s life. For some men, this treatment may only be given for a year or 2 and possibly resumed at a later time.
Medications that block testosterone’s effects (such as flutamide, bicalutamide, and nilutamide) may also be used. These medications are taken daily by mouth.’s effects (such as flutamide, bicalutamide, and nilutamide) may also be used. These medications are taken daily by mouth.
Side effects of hormonal therapy may include hot flashes, osteoporosis, loss of energy, reduction in muscle mass, fluid weight gain, reduction of libido, decrease in body hair, erectile dysfunction, and breast enlargement (gynecomastia).
The oldest form of hormonal therapy involves the removal of both testes (bilateral orchiectomy). The effects of bilateral orchiectomy on testosterone level are equivalent to those produced by leuprolide, goserelin, buserelin, and related medications. The physical and psychological effects of bilateral orchiectomy and other hormonal therapies make these therapies difficult for some men to accept.level are equivalent to those produced by leuprolide, goserelin, buserelin, and related medications. The physical and psychological effects of bilateral orchiectomy and other hormonal therapies make these therapies difficult for some men to accept.
Getting physical exercise, taking vitamin D and calcium supplements, stopping smoking, and avoiding excess alcohol are recommended for men on hormonal therapy to help minimize symptoms.Getting physical exercise, taking vitamin D and calcium supplements, stopping smoking, and avoiding excess alcohol are recommended for men on hormonal therapy to help minimize symptoms.
In men with widespread prostate cancer, hormonal therapy may become ineffective after a few years. When cancer eventually progresses despite hormonal therapy, men may live only a few more years.
Other medications
Cancer that does not respond to hormonal therapy that successfully decreases testosterone levels is called castrate-resistant prostate cancer (CRPC).
Recently, many other treatments that prolong life have become available and are being used earlier to treat metastatic prostate cancer, either in the initial treatment with hormone therapy or when hormone therapy fails. These treatments include sipuleucel-T (a vaccine that targets prostate cancer cells); pembrolizumab (an immunotherapy); abiraterone, enzalutamide, apalutamide, darolutamide (types of oral hormonal therapy); docetaxel and cabazitaxel (chemotherapy medications); and poly (ADP-ribose) polymerase (PARP) inhibitors in people who have CRPC with DNA repair defects or BRCA1/2 gene mutations. Radium-223, a radioactive medication given intravenously, can prolong life and prevent certain complications due to bone spread (such as spinal cord damage). Other treatments are under investigation. Recently, many other treatments that prolong life have become available and are being used earlier to treat metastatic prostate cancer, either in the initial treatment with hormone therapy or when hormone therapy fails. These treatments include sipuleucel-T (a vaccine that targets prostate cancer cells); pembrolizumab (an immunotherapy); abiraterone, enzalutamide, apalutamide, darolutamide (types of oral hormonal therapy); docetaxel and cabazitaxel (chemotherapy medications); and poly (ADP-ribose) polymerase (PARP) inhibitors in people who have CRPC with DNA repair defects or BRCA1/2 gene mutations. Radium-223, a radioactive medication given intravenously, can prolong life and prevent certain complications due to bone spread (such as spinal cord damage). Other treatments are under investigation.
Medications used to treat osteoporosis, such as zoledronic acid and denosumab, can be used to strengthen bone that has been weakened by cancer or by hormonal therapy, which tends to weaken bones. These medications help treat and prevent problems such as pain and the tendency to fracture.Medications used to treat osteoporosis, such as zoledronic acid and denosumab, can be used to strengthen bone that has been weakened by cancer or by hormonal therapy, which tends to weaken bones. These medications help treat and prevent problems such as pain and the tendency to fracture.
Common Methods and Strategies for Treating Prostate Cancer
Characteristics of the Cancer | Treatment Strategy | Method of Treatment |
|---|---|---|
Cancer confined to prostate in men | Active surveillance (to monitor and watch for symptoms or changes in the cancer, treating only when it becomes necessary) Curative treatment (to remove all traces of the cancer) | Surgery or radiation therapy |
Small, slow-growing cancer, confined to prostate in men | Active surveillance (to monitor and watch for symptoms or changes in the cancer, treating only when it becomes necessary) | No initial treatment |
Large or fast-growing cancer, confined to prostate | Curative treatment | Surgery or radiation therapy |
Cancer spread to areas outside the prostate, but not to distant areas | Palliative (aimed at slowing progression and relieving symptoms and that may prolong life but will not cure the cancer) or curative treatment | Radiation therapy with hormone therapy |
Widespread cancer | Palliative treatment (aimed at slowing progression and relieving symptoms and that may prolong life but will not cure the cancer) | Hormonal therapy, chemotherapy, sipuleucel-T, pembrolizumab, poly (ADP-ribose) polymerase (PARP) inhibitors, or radium-223Hormonal therapy, chemotherapy, sipuleucel-T, pembrolizumab, poly (ADP-ribose) polymerase (PARP) inhibitors, or radium-223 |
Follow-up
After all forms of treatment, PSA levels are measured at regular intervals (usually every 3 to 4 months for the first year, and then every 6 months for the rest of the man’s life). By 1 month after surgery, PSA should not be detected. Following radiation therapy, PSA decreases more slowly and usually does not become undetectable but should remain stable at a low level. Increases in the PSA level may indicate that the cancer has recurred.
Prognosis for Prostate Cancer
Prognosis for most men with localized prostate cancer is very good. Most older men with prostate cancer tend to live as long as other men their age who have similar general health and do not have prostate cancer. For many men, long-term remission or even cure is possible.
The prognosis depends upon the cancer’s grade and stage. High-grade cancers have a poor prognosis unless treated very early. Cancers that have spread to surrounding tissues also have a poorer prognosis. Metastatic prostate cancer has no cure. Most men with metastatic cancer live about 1 to 3 years after diagnosis, but some live for many years.
Prevention of Prostate Cancer
There have been no confirmed approaches to reliably preventing prostate cancer, but following a healthy lifestyle is considered a reasonable approach. This includes
Exercising
Eating a well-balanced diet (which includes limiting red meat and saturated fats, and eating lots of leafy green vegetables)
Limiting alcohol intake
Not smoking







