


Approximately 15% of American adults (37.5 million) ages 18 and over report some trouble hearing. The incidence increases with age. About 2 to 3 out of every 1,000 children in the United States are born with a detectable level of hearing loss in one or both ears. About 5% of adults ages 45 to 54 have disabling hearing loss. The rate increases to 10% for adults ages 55 to 64 years. Approximately 22% of those ages 65 to 74 and 55% of those who are 75 years and older have disabling hearing loss.
Most hearing loss develops slowly over time. However, sudden hearing loss occurs in about 1 in 5,000 to 1 in 10,000 people each year in the United States.
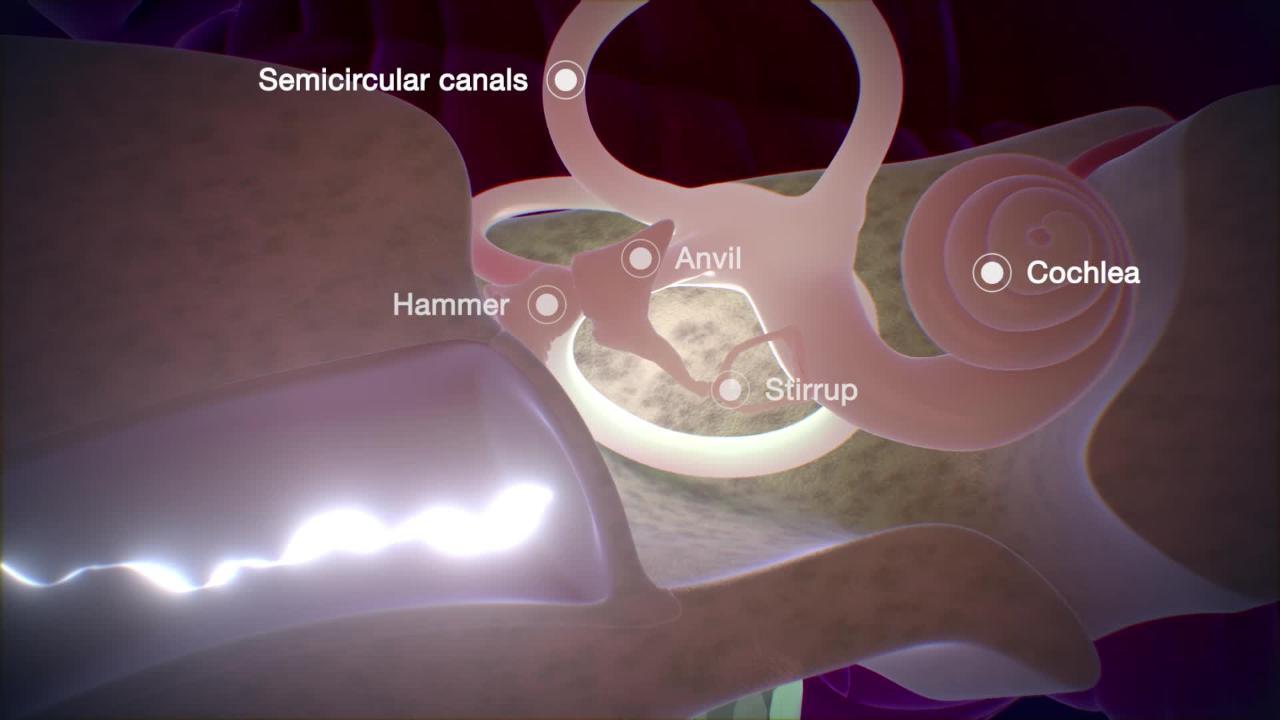
(See also Biology of the Ears.)
Causes of Hearing Loss
Hearing loss has many causes (see table Some Causes and Features of Hearing Loss ). Different parts of the hearing pathway can be affected, and loss is classified as conductive, sensorineural, or mixed, depending on the part of the pathway that is affected.
Conductive hearing loss occurs when something blocks sound from reaching the sensory structures in the inner ear. The problem may involve the external ear canal, the eardrum (tympanic membrane—TM), or the middle ear.
Sensorineural hearing loss occurs when sound reaches the inner ear, but either sound cannot be translated into nerve impulses (sensory loss) or nerve impulses are not carried to the brain (neural loss). The distinction between sensory and neural loss is important because sensory hearing loss is sometimes reversible and is seldom life threatening. A neural hearing loss rarely goes away and may be due to a potentially life-threatening brain tumor—commonly a cerebellopontine angle tumor (usually a vestibular schwannoma). An additional type of sensorineural loss is termed auditory neuropathy spectrum disorder, when sound can be detected but the signal is not sent correctly to the brain.
Mixed loss involves both conductive and sensorineural loss. It may be caused by severe head injury, chronic infection, or one of many rare genetic disorders.
Common causes of hearing loss
The most common causes overall are
Noise
Aging
Ear infections (particularly among children and young adults)
Earwax accumulation is the most common cause of treatable hearing loss, especially among older adults.
Noise can cause sudden or gradual sensorineural hearing loss. Exposure to a single, extreme noise (such as a nearby gunshot or explosion) can cause a sudden hearing loss referred to as acoustic trauma. Some people with acoustic trauma also develop ringing or buzzing in the ears (tinnitus). Hearing loss from acoustic trauma usually goes away within a day (unless there is also blast damage to the eardrum or middle ear), though there may be subtle damage to the inner ear that might accelerate age-related hearing loss years later. However, long-term exposure to noise causes most noise-induced hearing loss. Noise louder than about 85 decibels (dB) can cause hearing loss if exposure continues long enough. Although people vary somewhat in susceptibility to noise-induced hearing loss, nearly everyone loses some hearing if they are exposed to sufficiently intense noise for a long enough time.
Aging, together with noise exposure and genetic factors, is a common risk factor for hearing loss. Age-related hearing loss (presbycusis) limits a person’s ability to hear higher frequencies more than lower frequencies.
Ear infections are a common cause of temporary mild to moderate hearing loss (mainly in children). Most children regain normal hearing in 3 to 4 weeks after an ear infection resolves, but a few have persistent hearing loss. Persistent hearing loss is more likely in children who have recurring ear infections.
Less common causes
Less common causes include the following:
Systemic rheumatic and other autoimmune disorders
Congenital disorders
Medications that damage the ear (ototoxic medications)
Injuries
Some Causes and Features of Hearing Loss
Cause* | Common Features† | Diagnostic Approach‡ |
|---|---|---|
External ear (conductive loss) | ||
Obstruction (as caused by wax, a foreign body [object], an outer ear infection, or, rarely, a tumor) | Visible during a doctor's examination | A doctor's examination |
Middle ear (conductive loss) | ||
Usually an eardrum that looks abnormal (seen during a doctor's examination) Sometimes dizziness, pain or fullness in the ear, or a discharge from the ear Often many previous ear infections | Tympanometry (placement of a device in the ear to measure how well sound passes through the ear) Imaging for severe or recurrent infections | |
Often visible perforation of the eardrum, blood in the canal or behind the eardrum, or both In a person with an obvious recent injury | A doctor's examination | |
Otosclerosis | Often family members with similar hearing loss Hearing loss that slowly worsens Hearing loss that often starts in the 20s and 30s | Tympanometry |
Tumors (cancerous or not) | Often visible tumor during a doctor's examination Hearing loss in only one ear | CT or MRI using a contrast agent (gadolinium) |
Inner ear (sensory loss) | ||
Genetic disorders | Often family members with similar hearing loss Often accompanied by disease in other organ systems | Genetic testing CT and/or MRI using a contrast agent (gadolinium) of the inner ear |
Noise exposure | Usually apparent by history Temporary or permanent hearing loss, depending on how loud the noise and how long the exposure are | A doctor's examination |
Older age (over 55 years in men and over 65 years in women) Progressive loss of hearing in both ears Normal neurologic examination | A doctor's examination | |
Medications that can damage the ear (ototoxic medications), such as | In a person who recently used a causative medication Hearing loss in both ears Sometimes dizziness and loss of balance | A doctor's examination Sometimes measurement of the level of medication in the blood |
Infections, such as
| Obvious history of infection Hearing loss during or shortly after an infection | A doctor's examination |
Systemic rheumatic and other autoimmune disorders such as
| Sometimes joint inflammation and a rash Often in a person known to have the disorder | Blood tests |
Autoimmune inner ear disease | Hearing loss in both ears that can come and go and may worsen over time | Blood tests to check for other autoimmune disorders |
Meniere syndrome (including Meniere disease) | Episodes of low-frequency hearing loss (typically in only one ear) Sense of fullness in the ear Sometimes ringing or buzzing in the ear (tinnitus) and/or a false sensation of spinning or moving (vertigo) | MRI using a contrast agent (gadolinium) to rule out tumor |
Pressure changes (barotrauma, as may occur during diving) | Deafness in one or both ears Sudden onset during causative activity (for example, scuba diving, rapid descent in airplane) or after a blow to the ear Sometimes accompanied by pain, an explosive sound, dizziness, or ringing in the ear | Tympanometry Balance testing with electronystagmography (a test to record involuntary movements of the eye caused by a condition known as nystagmus) CT or MRI using a contrast agent (gadolinium) |
Head injury (often with fracture of the base of the skull)§ | In a person with an obvious recent severe injury Possibly dizziness or drooping facial muscles Sometimes fluid (bloody, blood-tinged, or clear) coming from the affected ear or blood behind the eardrum | CT or MRI using a contrast agent (gadolinium) |
Auditory neuropathy | Good sound detection, but poor word understanding | Specialized auditory testing MRI using a contrast agent (gadolinium) |
Nervous system (neural loss) | ||
Tumors, such as
| Hearing loss in only one ear, often with tinnitus Often dizziness or vertigo, trouble with balance Sometimes drooping facial muscles and/or numbness of the face and taste abnormalities | MRI using a contrast agent (gadolinium) |
Demyelinating disorders, such as multiple sclerosis | Hearing loss in only one ear Sometimes weakness or numbness that comes and goes and that occurs in different parts of the body | MRI of the brain and spinal cord using a contrast agent (gadolinium) Sometimes a spinal tap (lumbar puncture) |
* Causes in each group are listed in approximate order of frequency. | ||
† Features include symptoms and the results of the doctor's examination. Features mentioned are typical but not always present. | ||
‡ Although a doctor's examination with audiologic testing is always done, it is only mentioned in this column if the diagnosis can sometimes be made only by the doctor's examination and audiologic testing without any additional testing. In other words, additional tests may not be needed. | ||
§ Mixed conductive and sensorineural loss may be present. | ||
CT = computed tomography; MRI = magnetic resonance imaging. | ||
Evaluation of Hearing Loss
The following information can help people decide when to see a doctor and know what to expect during the evaluation.
Warning signs
In people with hearing loss, certain symptoms and characteristics are cause for concern. They include
Hearing loss in only one ear
Any neurologic abnormalities (such as difficulty chewing or speaking, numbness of the face, dizziness, or loss of balance)
When to see a doctor
People with warning signs should see a doctor right away. People with hearing loss and no warning signs should see their doctor very soon.
Because people may not notice gradual hearing loss, doctors recommend routine screening hearing tests for children and older adults. Childhood screening should begin at birth so that hearing deficits can be found and treated before they interfere with language development. Doctors often routinely screen older adults by asking them specific questions about their ability to hear in certain situations. Such screening, while important, should be followed up with formal audiologic testing because many older adults who might benefit from treatment do not realize or may even deny that they have a hearing problem.
What the doctor does
Doctors first ask questions about the person's symptoms and medical history. Doctors then do a physical examination. What they find during the history and physical examination may suggest a cause of the hearing loss and the tests that may need to be done, including audiogram, and if warranted, imaging of the ear (such as computed tomography [CT] or magnetic resonance imaging [MRI]).
Doctors ask how long people have noticed hearing loss, whether the loss is in one or both ears, and whether the loss followed any sudden event (for example, a head injury, sudden change in pressure, or starting of a medication). It is also important for them to note the following:
Ear symptoms, such as pain or fullness, ringing or buzzing in the ears (tinnitus), or discharge
Balance symptoms, such as disorientation in the dark or a false sensation of spinning or moving (vertigo)
Neurologic symptoms, such as headache, weakness of the face, or an abnormal sense of taste
In children, important associated symptoms include delays in speech or language development and delayed motor development.
Doctors explore people's medical history for disorders that might cause hearing loss, including repeated ear infections, chronic exposure to loud noise, head injury, and systemic rheumatic disorders such as rheumatoid arthritis and systemic lupus erythematosus. Doctors note whether people have a family history of hearing loss. Doctors also ask people whether they are taking medications that can damage the ear (ototoxic medications). For young children, doctors review the birth history to determine if there were any birth complications or infections prior to birth.
The physical examination focuses on the ears and hearing and the neurologic examination. Doctors inspect the external ear for obstruction, infection, malformations that are present at birth (congenital), and other visible abnormalities. The eardrum is examined for tears (perforations), drainage, and signs of acute or chronic infection. Doctors often do several tests using a tuning fork to differentiate conductive from sensorineural hearing loss.
Testing
Testing includes
Audiologic tests
Sometimes MRI or CT
Doctors perform audiologic tests on all people who have hearing loss. Audiologic tests help doctors understand the type of hearing loss and determine what other testing may be needed.
Audiometry is the first step in hearing testing. In this test, a person wears headphones that play tones of different frequency (pitch) and loudness into one ear or the other. The person signals when a tone is heard, usually by raising the corresponding hand. For each pitch, the test identifies the quietest tone the person can hear in each ear. The results are presented in comparison to what is considered normal hearing. Because loud tones presented to one ear may also be heard by the other ear, a sound other than the test tone (usually white noise) is presented to the ear not being tested.
Tuning fork tests are sometimes done during a person's first evaluation by a doctor, but rarely by specialists or audiologists, who have more precise ways to assess hearing. Tuning fork tests can help distinguish between conductive and sensorineural hearing loss. The Rinne test and the Weber test are 2 types of tuning fork tests:
The Rinne test compares how well a person hears sounds conducted by air with how well the person hears sounds conducted by the skull bones. To test hearing by air conduction, the tuning fork is placed near the ear. To test hearing by bone conduction, the base of a vibrating tuning fork is placed against the head so the sound bypasses the middle ear and goes directly to the nerve cells of the inner ear. If hearing by air conduction is reduced but hearing by bone conduction is normal, the hearing loss is conductive. If both air and bone conduction hearing are reduced, the hearing loss is sensorineural or mixed. People with sensorineural hearing loss may need further evaluation to look for other conditions, such as Meniere disease or brain tumors.
In the Weber test, the stem of a vibrating tuning fork is placed on the top of the head in the middle. The person indicates in which ear the tone is louder. In one-sided conductive hearing loss, the tone is louder in the ear with hearing loss. In one-sided sensorineural hearing loss, the tone is louder in the normal ear because the tuning fork stimulates both inner ears equally and the person hears the stimulus with the unaffected ear.
Speech threshold audiometry measures how loudly words have to be spoken to be understood. A person listens to a series of two-syllable, equally accented words (spondees), such as "railroad," "stairway," and "baseball," presented at different volumes. The volume at which the person can correctly repeat half of the words (spondee threshold) is recorded.
Discrimination, the ability to hear differences between words that sound similar, is tested by presenting pairs of similar one-syllable words. The percentage of words correctly repeated is the discrimination score. People with a conductive hearing loss usually have a normal discrimination score, although at a higher volume. People with sensorineural hearing loss may have abnormal discrimination at all volumes. Doctors sometimes test people's ability to recognize words within full sentences. This test helps decide which people who do not have acceptable results with a hearing aid might benefit from an implanted device.
Tympanometry tests how well sound can pass through the eardrum and middle ear. This test does not require the active participation of the person being tested and is commonly used in children. A device containing a microphone and a sound source is placed snugly in the ear canal, and sound waves are bounced off the eardrum as the device varies the pressure in the ear canal. Abnormal tympanometry results suggest a conductive type of hearing loss.
Auditory brain stem response is a test that measures nerve impulses in the brain stem resulting from sound signals in the ears. The information helps determine what kind of signals the brain is receiving from the ears. Test results are abnormal in people with some sensorineural types of hearing loss and in people with many types of brain disorders. Auditory brain stem response is used to test infants and also can be used to monitor certain brain functions in people who are comatose or undergoing brain surgery.
Electrocochleography measures the activity of the cochlea and the auditory nerve by means of an electrode placed on, or through, the eardrum. This test and the auditory brain stem response can be used to measure hearing in people who cannot or will not respond voluntarily to sound. For example, these tests are used to find out whether infants and very young children have profound hearing loss (deafness).
Otoacoustic emissions testing uses sound to stimulate the inner ear (cochlea). The ear itself then generates a very low-intensity sound that matches the stimulus. These cochlear emissions are recorded using sophisticated electronics and are used routinely in many nurseries to screen newborns for congenital hearing loss and to monitor the hearing of people who are using ototoxic medications. This test is also used in adults to help determine the reason for a hearing loss.

Other tests can measure the ability to interpret and understand distorted speech, understand a message presented to one ear when a competing message is presented to the other ear, fuse incomplete messages to each ear into a meaningful message, and determine where a sound is coming from when it is presented to both ears at the same time.
People who have an abnormal neurologic examination or who have certain findings on audiologic tests also need a gadolinium-enhanced MRI of the head. This type of MRI can help doctors detect certain disorders of the inner ear, brain tumors near the ear, or tumors in the nerves coming from the ear.
Many genetic causes of deafness also cause problems in other organ systems. Therefore, children with unexplained hearing loss should also have additional testing, such as an eye examination, an electrocardiogram (ECG) to look for long QT syndrome, or other organ-specific tests, and genetic testing.
Prevention of Hearing Loss
Limiting exposure to loud noise can help prevent hearing loss. Both the duration and intensity of noise should be limited. People regularly exposed to loud noise must wear ear protectors (such as plastic plugs in the ear canals or glycerin-filled muffs over the ears). The Occupational Safety and Health Administration (OSHA) of the U.S. Department of Labor and similar agencies in many other countries have standards regarding the length of time that people can be exposed to noise. The louder the noise, the shorter is the permissible time of exposure. Earplugs or other ear protectors can also be considered if even brief exposure to very loud noises is anticipated, such as at concerts.
Treatment of Hearing Loss
Any cause of hearing loss is treated. For example, doctors remove benign or cancerous growths. When possible, they stop giving ototoxic medications (unless the need for the medication outweighs the risk of additional hearing loss).
Many causes of hearing loss have no cure, and treatment involves compensating for the hearing loss with hearing aids and various assistive strategies and technologies.
Assistive strategies and technologies
Several types of assistive devices are available for people who have significant hearing loss. Alerting systems that use light let people with hearing loss know when the doorbell is ringing, a smoke detector is sounding, or a baby is crying. Special sound systems transmitting infrared or FM radio signals help people hear in theaters, churches, or other places where competing noise exists. Many television programs carry closed captioning. Telephone communication devices are also available.
Lip reading and other strategies for coping with hearing loss are sometimes taught by hearing professionals in a program called aural rehabilitation. In addition to training in lip reading, people are taught to gain control over their listening environment by learning to anticipate difficult communication situations and modifying or avoiding them.
People with profound hearing loss often communicate by using sign language. American Sign Language (ASL) is the most common version in the United States. Other forms of language using visual signs include Signed English, Signing Exact English, and Cued Speech. Around the world, it has been estimated that there are over 300 unique sign languages, with different countries, cultures, and villages having their own unique form of sign language.
Single-sided deafness
People with hearing loss in only one ear (single-sided deafness [SSD]) usually do not have communication limitations in one-on-one situations. However, with noisy backgrounds or complex acoustic environments (for example, classrooms, parties, and meetings), people with SSD are unable to hear and communicate effectively. Further, people who hear out of only one ear are unable to determine the origin of sounds (sound localization). For many people, SSD can be life-altering and lead to significant disability at work and in social situations.
Treatment for SSD includes Contralateral Routing of Signal (CROS) hearing aids or bone-anchored hearing implants that pick up sound from the deaf side and transfer it to the hearing ear. Although these technologies improve hearing in noisy settings, they do not allow sound localization. Cochlear implants are increasingly being used with success in people with SSD, particularly if the SSD is accompanied by severe tinnitus (ringing or buzzing in the ears). Implants have also been shown to provide sound localization.

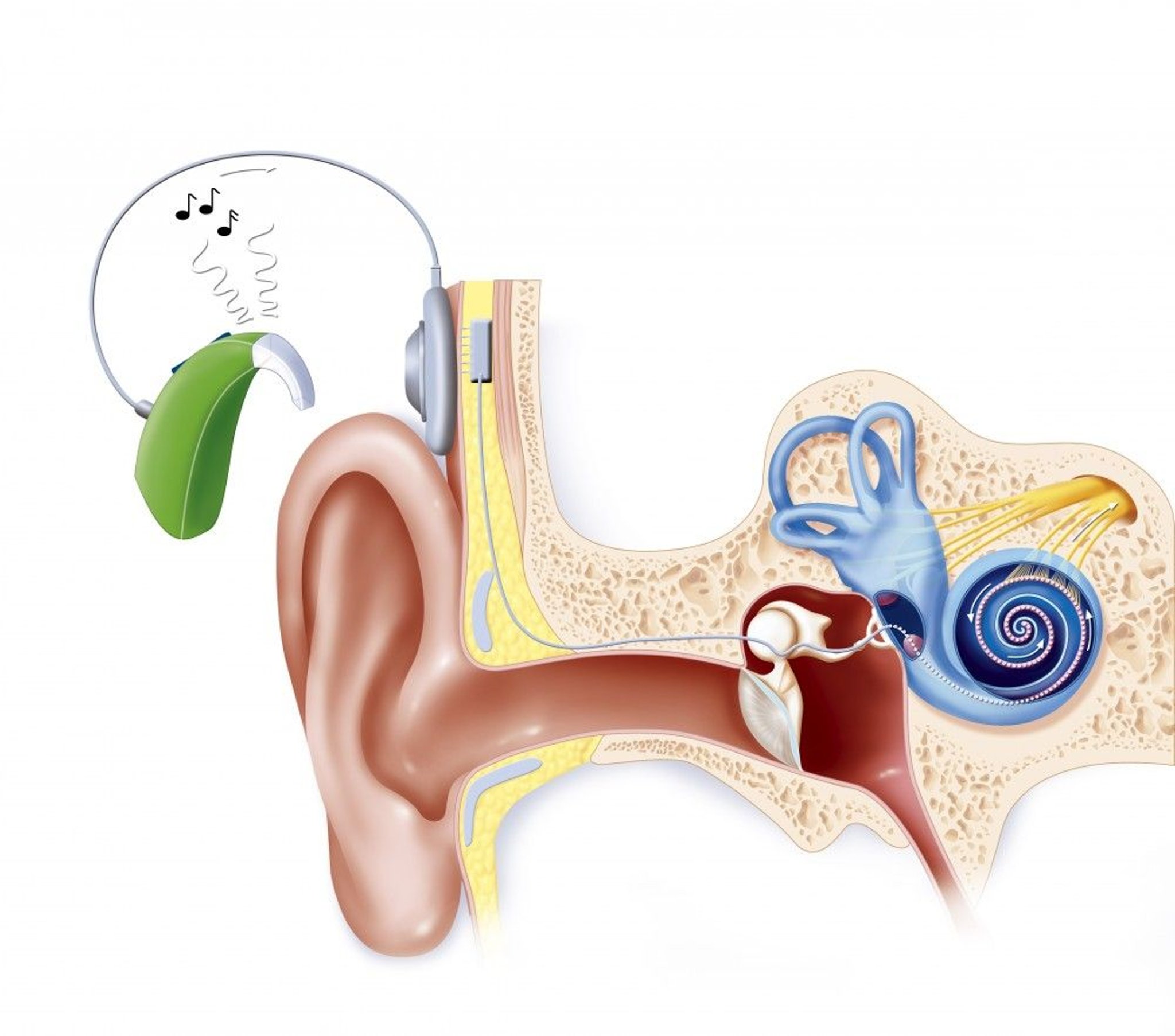
JACOPIN/BSIP/SCIENCE PHOTO LIBRARY
Treatment in children
In addition to having any cause treated and hearing aids provided, children with hearing loss require support of language development with appropriate therapy. Because children must be able to hear language to learn it spontaneously, most deaf children develop language only with special training. Ideally, this training begins as soon as the hearing loss is identified. An exception would be a deaf child growing up with deaf parents who are fluent sign language users. Deaf infants also need a way to communicate before they learn to speak. For example, a sign language that is tailored to infants can provide a foundation for later development of spoken language if a cochlear implant is not available. However, for children, there is no substitute for access to the sounds of speech (phonemes) to enable a refined and nuanced understanding of speech and language.
A cochlear implant may be helpful for infants who have profound hearing loss in both ears and who cannot hear sounds with a hearing aid. The sooner the implant can be placed in deaf children, the greater hearing improves. Although cochlear implants help many children with either congenital or acquired deafness hear, they are usually more effective in children who already have developed language. Sometimes the inner ear hardens into bone (ossifies) in children who become deaf after having meningitis. In such cases, cochlear implants should be used early to maximize effectiveness. Children whose acoustic nerves have been destroyed by tumors may be helped by having electrodes implanted in the base of the brain (brain stem) as well. Children with cochlear implants may have a slightly greater risk of meningitis than children without cochlear implants or adults with cochlear implants.
Children who are deaf in only one ear should be allowed to use a special system in the classroom, such as an FM auditory trainer. With these systems, the teacher speaks into a microphone that sends signals to a hearing aid in the child’s normal ear. This process improves the child’s greatly impaired ability to hear speech against a noisy background. Also, children who are deaf in only one ear may benefit from a cochlear implant in their deaf ear.
Essentials for Older Adults: Hearing Loss
Older adults typically have a progressive decrease in hearing, called presbycusis. About 5% of adults ages 45 to 54 have disabling hearing loss. The rate increases to 10% for adults ages 55 to 64 years. Approximately 22% of those ages 65 to 74 and 55% of those who are 75 years and older have disabling hearing loss. Even so, doctors should evaluate older adults with hearing loss because the cause may not be aging. Some people may have a tumor, a neurologic or autoimmune or systemic rheumatic disorder, or an easily correctable cause of hearing loss.
Even mild hearing loss makes understanding speech difficult and causes older adults with hearing loss to exhibit certain common behaviors. An older adult with mild hearing loss may avoid conversations. Understanding speech may be particularly difficult if there is background noise or more than one person is talking, such as in a restaurant or at a family gathering. Constantly asking others to talk louder can frustrate both the listener and the speaker. People with hearing loss may misunderstand a question and give an apparently bizarre answer, leading others to believe they are confused. They may misjudge the loudness of their own speech and thus shout, discouraging others from conversing with them. Thus, hearing loss can lead to social isolation, inactivity, loss of social support, and depression. In a person with dementia, hearing loss can make communicating even more difficult. For people affected by dementia, correcting a hearing loss makes dementia easier to cope with. Correcting hearing loss has clear physical and psychosocial health benefits.
Presbycusis
Presbycusis is age-related hearing loss. It probably results from a combination of age-related deterioration and the effects of a lifetime of noise exposure and genetics.
Hearing loss usually affects the highest sound frequencies first, usually beginning at about age 55 to 65 years (sometimes sooner). The loss of high-frequency hearing makes speech particularly hard to understand, even when the overall loudness of speech seems normal. That is because certain consonants (such as C, D, K, P, S, T) are high-frequency sounds. These consonant sounds are the most important for speech recognition. For example, when the words “shoe,” “blue,” “true,” “too,” or “new” are spoken, many people with presbycusis can hear the “oo” sound, but they cannot recognize which word has been spoken because they cannot distinguish the consonants. Affected people typically think the speaker is mumbling. A speaker attempting to speak louder usually accentuates vowel sounds (which are low frequency), doing little to improve speech recognition. Excessive background noise makes speech comprehension particularly difficult.
Screening
Screening older adults for hearing loss is important because many do not notice it themselves. Family members or doctors can ask the person a series of questions using a screening tool such as the Hearing Handicap Inventory for the Elderly–Screening Version, which asks:
Does a hearing problem cause you to feel embarrassed when you meet people?
Does a hearing problem cause you to feel frustrated when talking to a family member?
Do you have difficulty hearing when someone whispers?
Do you feel handicapped by a hearing problem?
Does a hearing problem cause you difficulty when visiting friends, relatives, or neighbors?
Does a hearing problem cause you to attend religious services less often than you would like?
Does a hearing problem cause you to have arguments with family members?
Does a hearing problem cause you difficulty when listening to the television or radio?
Do you feel that any difficulty with your hearing hampers your personal or social life?
Does a hearing problem cause you difficulty when in a restaurant with relatives or friends?
For each question, a “no” answer = 0 points, “sometimes” = 2 points, and “yes” = 4 points. A score over 10 suggests significant hearing loss, and follow up with a hearing specialist is recommended.
Key Points
Earwax, infections, aging, and noise exposure are the most common causes of hearing loss.
All people with hearing loss should have audiologic testing.
People with neurologic symptoms (such as dizziness or vertigo) usually should undergo imaging tests.
Treatments include correction of preventable causes (such as noises or medications), surgery (for example, to remove benign or cancerous growths), hearing aids, cochlear implants, and various assistive technologies.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
National Institute on Deafness and Other Communication Disorders: Information regarding hearing loss and other communication disorders, spanning functions of hearing, balance, taste, smell, voice, speech, and language
The National Institute for Occupational Safety and Health (NIOSH)—Noise and Hearing Loss Prevention: Reviews occupational regulations and standards, noise control strategies, and hearing protective devices, as well as hearing loss prevention programs, risk factors, and information for specific industries and occupations
Occupational Safety and Health Administration (OSHA): Occupational Noise Exposure: Information on hearing damage from workplace noise exposure, including a link to download a tool that measures sound levels and provides noise exposure parameters to help reduce occupational noise-induced hearing loss







