




Any cancer may metastasize to bone, but metastases from carcinomas are the most common, particularly those arising in the following areas:
Prostate cancer in men and breast cancer in women are the most common types of cancers. Lung cancer is the most common cause of cancer death in both sexes. Breast cancer is the most common cancer to metastasize to bone. Any bone may be involved with metastases. Metastatic disease does not commonly spread to bone below the mid forearm or mid calf, but when it occurs in those sites, it results most often from lung or sometimes kidney cancer.
The American Cancer Society: Cancer Facts & Figures 2022 project that the incidence of breast cancer in females (287,850) will be higher than lung cancer incidence of males and females combined (236,740). However, the incidence of lung cancer deaths, whether male (68,820) or female (61,360), will be higher than the incidence of breast cancer deaths in females (42,350) or prostate cancer in males (34,500). Published case series of orthopedic surgical management of metastatic lesions in cancer centers show that breast cancer remains the most common cancer requiring orthopedic intervention. Usually medically treated metastatic breast cancer patients survive longer before they succumb to lung, liver, and brain metastasis compared to other solid organ metastatic lesions.
(See also Overview of Bone and Joint Tumors.)
Symptoms and Signs of Metastatic Bone Tumors
Metastases manifest as bone pain, although they may remain asymptomatic for some time. Bone metastases may cause symptoms before the primary tumor is suspected or may appear in patients with a known diagnosis of cancer.
Diagnosis of Metastatic Bone Tumors
X-ray of the entire bone
Whole body radionuclide technecium-99m bone scanning to identify metastases
Advanced imaging (CT, MRI, and/or whole body PET-CT scanning for selected purposes)
Clinical evaluation and testing to diagnose the primary tumor (if unknown)
Often biopsy if the primary tumor is unknown after assessment
Metastatic bone tumors are considered in all patients with unexplained bone pain, but particularly in patients who have
Known cancer
Pain or radiographic abnormalities at more than one site
Findings on imaging studies that suggest metastases
Prostate cancer is most often blastic, lung cancer is most often lytic, and breast cancer may be blastic or lytic.

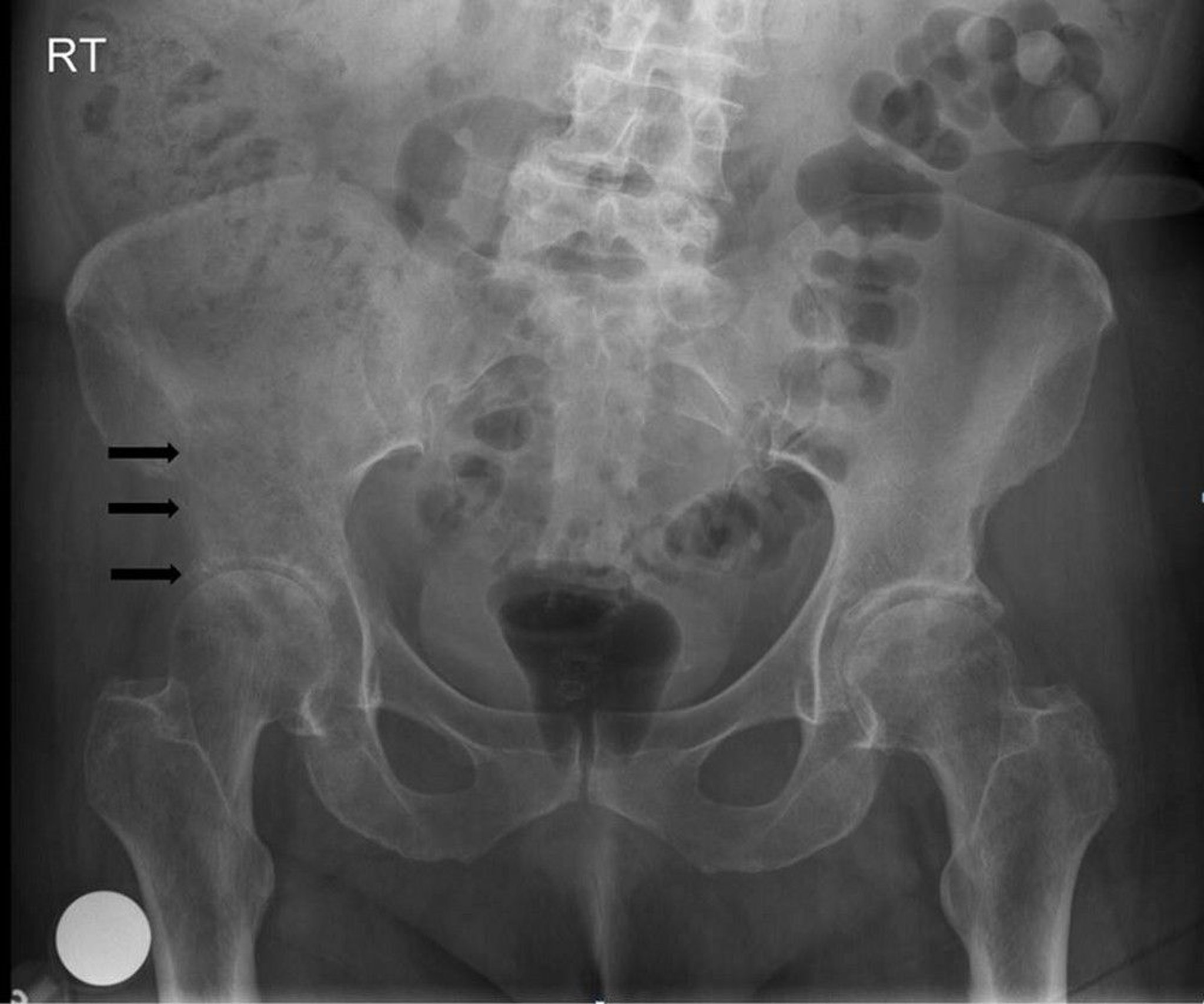
Image courtesy of Michael J. Joyce, MD, and Hakan Ilaslan, MD.
CT and particularly MRI are highly sensitive for specific metastases. However, if metastases are suspected, a radionuclide whole-body scan, which is not quite as sensitive or specific, is usually done. Bone scan is more sensitive for early and asymptomatic bone metastases than plain x-rays and can be used to scan the entire body. Lesions on the scan are usually presumed to be metastases if the patient has a known primary cancer.
Metastases should be suspected in patients who have multiple lesions on bone scan. Although metastases are suspected in patients with known cancer and a single bone lesion, the lesion may not be a metastasis; thus, a needle biopsy of the lesion is often done to confirm the diagnosis of a metastasis. Whole-body PET-CT is now often used for some tumors; it is more specific for bone metastases than is radionuclide bone scan and can identify many extraskeletal metastases.
An evaluation to identify an initially unknown primary cancer in a patient with a single or multiple bony lesions includes a comprehensive history and physical examination; CT of the chest, abdomen, and pelvis; mammography in females; and prostate-specific antigen (PSA) measurement in males. Such an approach will identify the primary cancer over 85% of the time. However, bone biopsy, especially fine-needle or core biopsy, is necessary if metastatic tumor is suspected and the primary tumor has not been otherwise diagnosed. Biopsy with use of immunohistologic stains may give clues to the primary tumor type. Sometimes the primary tumor cannot be identified after these tests plus PET-CT and any indicated endoscopy.
In patients who present with a fracture, especially older patients, it is important to determine if it is a pathologic fracture due to a cancer. Such a fracture should be suspected if the patient has a known primary cancer. However, the fracture may be the initial manifestation of a cancer elsewhere in the body. The radiographic appearance may be destructive, suggesting a cancer, but may have only subtle abnormalities, for example, such as punctate calcifications that are easily missed may be the only findings suggesting a cancer. Also, although unusual, a bone lesion thought to be the cause of a metastatic fracture may be a fracture through a primary bone tumor such as chondrosarcoma or osteosarcoma. An atypical (as judged by patient age or radiographic appearance) destructive "metastatic" lesion with or without fracture especially with punctate calcifications must be discriminated from the rare primary bone tumor with the help of a musculoskeletal surgical oncologist or musculoskeletal radiologist.

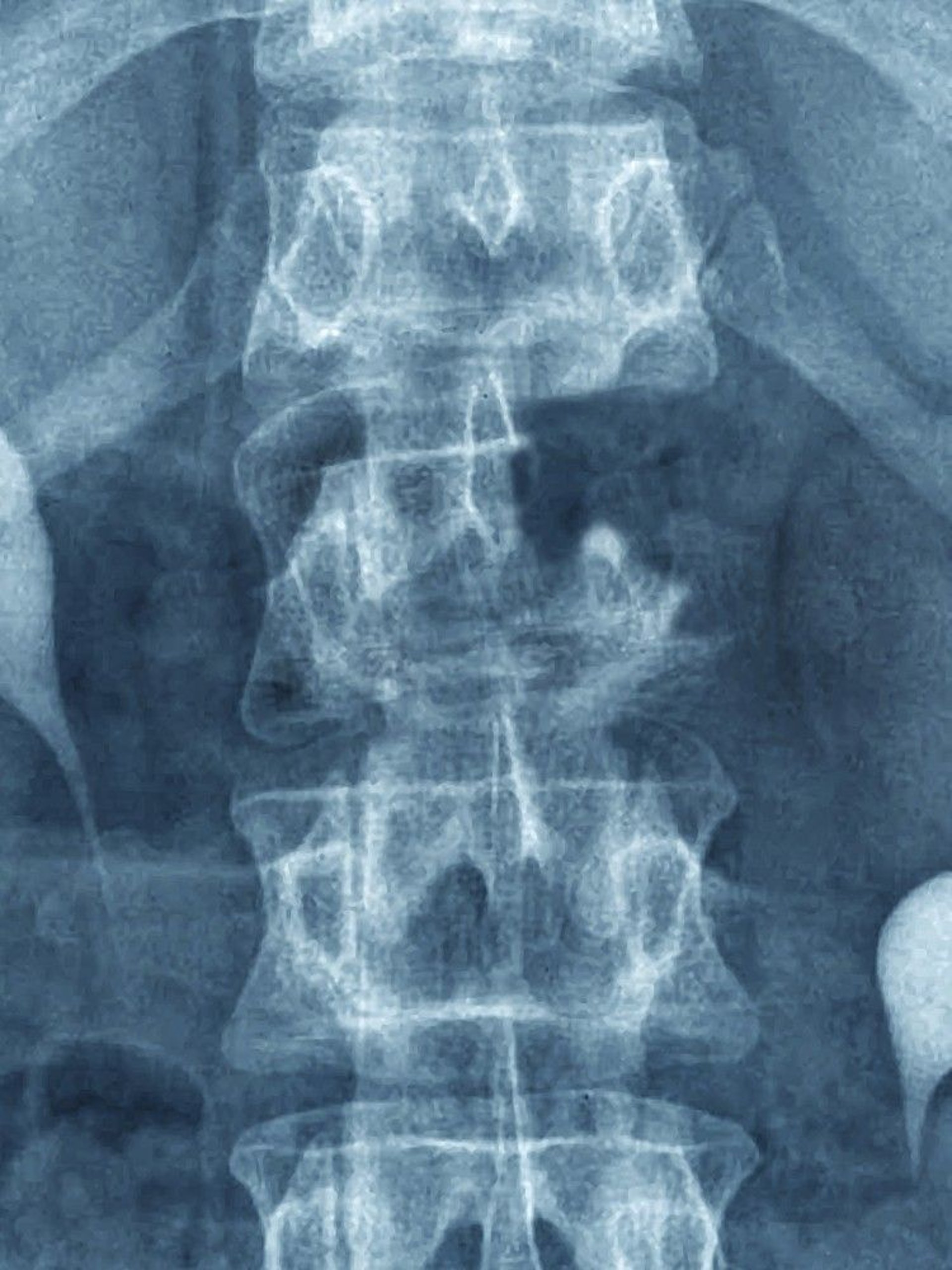
CAVALLINI JAMES/BSIP/SCIENCE PHOTO LIBRARY
Treatment of Metastatic Bone Tumors
Usually radiation therapy for symptomatic or large or progressively enlarging lesions
Surgery to stabilize bone at risk of pathologic fracture or resect highly diseased bone (with joint reconstruction if needed)
Kyphoplasty or vertebraplasty for certain painful vertebral fractures
denosumab
If bone destruction is extensive, resulting in imminent or actual pathologic fracture, surgical fixation or resection and reconstruction may be required to provide stabilization and help minimize morbidity. When the primary cancer has been removed and only limited bone metastasis remains (especially if the metastatic lesion appears ≥ 1 year after the primary tumor), en bloc excision sometimes combined with radiation therapy, chemotherapy, or both rarely may be curative. Insertion of methyl methacrylate into the spine (kyphoplasty or vertebraplasty) relieves pain and expands and stabilizes compression fractures that do not have epidural soft tissue extension.


This image shows bone destruction due to a metastasis secondary to renal cell carcinoma in the proximal femur. The location and extent of bone destruction make the risk of fracture extremely high (imminent fracture).
Image courtesy of Michael J. Joyce, MD, and David M. Joyce, MD.


This x-ray shows a large metastatic lytic lesion of the femoral medial condyle with imminent fracture.
Image courtesy of Michael J. Joyce, MD, and David M. Joyce, MD.


This image shows a failed surgical management of a metastatic breast lesion requiring a second operation.
Image courtesy of Michael J. Joyce, MD, and David M. Joyce, MD.
This image shows bone destruction due to a metastasis secondary to renal cell carcinoma in the proximal femur. The location and extent of bone destruction make the risk of fracture extremely high (imminent fracture).
Image courtesy of Michael J. Joyce, MD, and David M. Joyce, MD.
This x-ray shows a large metastatic lytic lesion of the femoral medial condyle with imminent fracture.
Image courtesy of Michael J. Joyce, MD, and David M. Joyce, MD.
This image shows a failed surgical management of a metastatic breast lesion requiring a second operation.
Image courtesy of Michael J. Joyce, MD, and David M. Joyce, MD.
Key Points
Carcinomas of breast, lung, prostate, and kidney are the most common sources of metastatic bone tumors.
Bone metastases should be suspected in patients with known cancer, when pain is at more than one site, and/or when findings on imaging studies suggest metastases.
Bone biopsy is needed if the primary tumor is unknown after clinical and radiographic evaluation.
Patients with known solid organ cancer and limited bone lesions may require a needle biopsy to confirm metastatic disease and exclude a second primary tumor.
Pathologic fractures may require treatment with surgery, kyphoplasty, or vertebraplasty.







