




Unstable angina results from acute obstruction of a coronary artery without myocardial infarction. Symptoms include chest discomfort with or without dyspnea, nausea, and diaphoresis. Diagnosis is by electrocardiography (ECG) and the presence or absence of biomarkers. Treatment is with antiplatelets, anticoagulants, nitrates, statins, and beta-blockers. Coronary angiography with percutaneous intervention or coronary artery bypass surgery is often necessary.
(See also Overview of Acute Coronary Syndromes.)
Unstable angina is a type of acute coronary syndrome that is defined as one or more of the following in patients whose cardiac biomarker levels do not meet criteria for acute myocardial infarction (MI):
Rest angina that is prolonged (usually > 20 minutes)
New-onset angina of at least class 3 severity in the Canadian Cardiovascular Society (CCS) classification (see table Canadian Cardiovascular Society Classification System for Angina Pectoris)
Increasing angina, ie, previously diagnosed angina that has become distinctly more frequent, more severe, longer in duration, or lower in threshold (eg, increased by ≥ 1 CCS class or to at least CCS class 3)
Unstable angina is clinically unstable and often a prelude to myocardial infarction or arrhythmias or, less commonly, to sudden death.
Symptoms and Signs of Unstable Angina
Patients have symptoms of angina pectoris (typically chest pain or discomfort) except that the pain or discomfort of unstable angina usually is more intense, lasts longer, is precipitated by less exertion, occurs spontaneously at rest, is progressive (crescendo) in nature, or involves any combination of these features.
Unstable angina is classified based on severity and clinical situation (see table Canadian Cardiovascular Classification System for Angina Pectoris). Also considered are whether unstable angina occurs during treatment for chronic stable angina and whether transient changes in ST-T waves occur during angina. If angina has occurred within 48 hours and no contributory extracardiac condition is present, troponin levels may be measured to help estimate prognosis; troponin-negative results indicate a better prognosis than troponin-positive.
Diagnosis of Unstable Angina
Serial ECGs
Serial cardiac biomarkers
Immediate coronary angiography for patients with complications (eg, persistent chest pain, hypotension, unstable arrhythmias)
Delayed angiography (24 to 48 hours) for stable patients
(See figure Approach to Unstable Angina.)
Evaluation begins with initial and serial ECG and serial measurements of cardiac biomarkers to help distinguish between unstable angina and acute myocardial infarction (MI)—either non–ST-segment elevation MI (NSTEMI) or ST-segment elevation MI (STEMI). This distinction is the center of the decision pathway because fibrinolytics benefit patients with STEMI but not those with NSTEMI and unstable angina. Also, urgent cardiac catheterization is indicated for patients with acute STEMI but not generally for those with NSTEMI or unstable angina.
ECG
ECG is the most important test and should be done as soon as possible (eg, within 10 minutes of presentation) ECG changes such as ST-segment depression, ST-segment elevation, or T-wave inversion may occur during unstable angina but are transient.
Cardiac biomarkers
Patients suspected of having unstable angina should have a highly sensitive assay of cardiac troponin (hs-cTn) done on presentation and 2 to 3 hours later. If a standard Tn assay is used, measurements are done at presentation and 6 hours later.
Creatine kinase MB fraction (CK-MB) is not elevated in unstable angina. Cardiac troponin, particularly when measured using high-sensitivity troponin tests, may be slightly increased but does not meet the criteria for myocardial infarction (above the 99th percentile of the upper reference limit or URL).
Coronary angiography
Patients with unstable angina whose symptoms have resolved typically undergo angiography within the first 24 to 48 hours of hospitalization to detect lesions that may require treatment. Coronary angiography most often combines diagnosis with percutaneous coronary intervention (PCI—ie, angioplasty, stent placement).
After initial evaluation and therapy, coronary angiography may be used in patients with evidence of ongoing ischemia (ECG findings or symptoms), hemodynamic instability, recurrent ventricular tachyarrhythmias, and other abnormalities that suggest recurrence of ischemic events.
Treatment of Unstable Angina
Pharmacologic therapy: Antiplatelet agents, antianginal drugs, anticoagulants, and in some cases other medications
Angiography to assess coronary artery anatomy
Reperfusion therapy: Percutaneous coronary intervention or coronary artery bypass surgery
Post-discharge rehabilitation and chronic medical management of coronary artery disease
Prehospital care
Oxygen
Nitrates
Triage to appropriate medical center
1). Early diagnostic data and response to treatment can help determine the need for and timing of revascularization.
Hospital admission
Risk-stratify patient and choose timing of reperfusion strategy
Pharmacologic therapy with antiplatelets, anticoagulants, and other medications based on reperfusion strategy
On arrival to the emergency department, the patient's diagnosis is confirmed. Pharmacologic therapy and timing of revascularization depend on the clinical picture. In clinically unstable patients (patients with ongoing symptoms, hypotension or sustained arrhythmias), urgent angiography with revascularization is indicated. In clinically stable patients, angiography with revascularization may be deferred for 24 to 48 hours (see figure Approach to Unstable Angina).
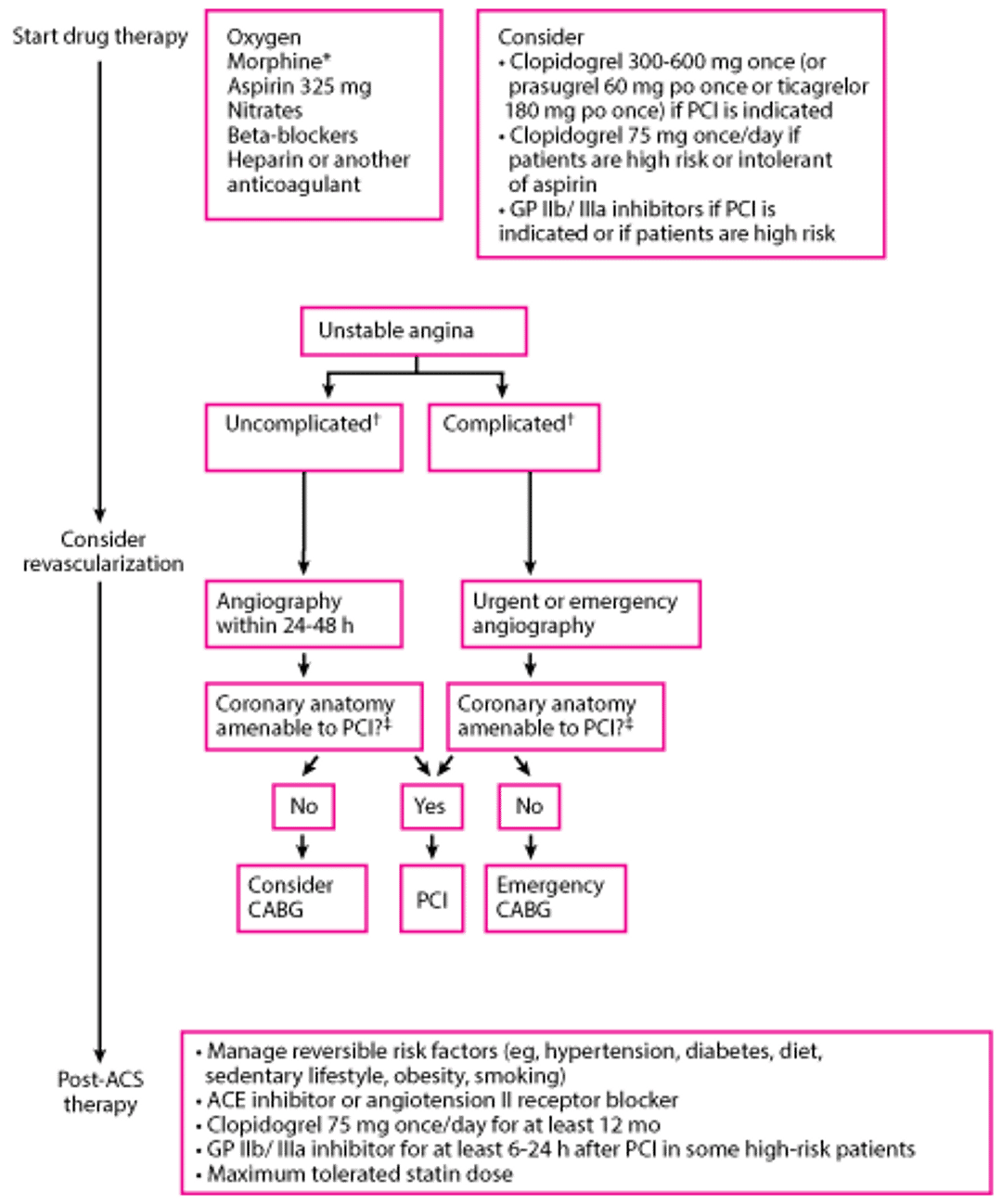
Approach to Unstable Angina
* Morphine should be used judiciously (eg, if nitroglycerin is contraindicated or if the patient has symptoms despite nitroglycerin therapy). Data suggest that morphine attenuates activity of some P2Y12 receptor inhibitors and may contribute to worse patient outcomes. |
† Complicated means that the hospital course was complicated by recurrent angina or infarction, heart failure, or sustained recurrent ventricular arrhythmias. Absence of any of these events is termed uncomplicated. |
‡ CABG is still generally preferred to PCI for patients with the following:
Also, lesions that are long or near bifurcation points are often not amenable to PCI. |
CABG = coronary artery bypass grafting; GP = glycoprotein; NSTEMI = non–ST-segment elevation myocardial infarction; PCI = percutaneous coronary intervention; STEMI = ST-segment elevation myocardial infarction. |

Pharmacologic treatment of unstable angina
All patients should be given antiplatelet agents, anticoagulants, and if chest pain is present, antianginals. The specific medications used depend on the reperfusion strategy and other factors; their selection and use is discussed in Medications for Acute Coronary Syndrome. Other medications, such as beta-blockers, angiotensin-converting enzyme (ACE) inhibitors, and statins, should be initiated during admission (see table Medications for Coronary Artery Disease).
Patients with unstable angina should be given the following (unless contraindicated)
Anticoagulants: A heparin (unfractionated or low molecular weight heparin
Sometimes a glycoprotein IIb/IIIa inhibitor when PCI is done
Beta-blocker
Angiotensin-converting enzyme (ACE) inhibitor
Statin
Aspirin reduces short- and long-term mortality risk (2prasugrel and ticagrelor are more rapid in onset and may be preferred.
Either a low molecular weight heparin (LMWH), unfractionated heparinheparin-induced thrombocytopenia.
3).
Nitroglycerin is preferable to morphine, which should be used judiciously (eg, if a patient has a contraindication to nitroglycerin or is in pain despite maximal nitroglycerin therapy). is initially given sublingually, followed by continuous IV drip if needed. Morphine, given 2 to 4 mg IV, repeated every 15 minutes as needed, is highly effective but can depress respiration, can reduce myocardial contractility, and is a potent venous vasodilator. Evidence also suggests that morphine interferes with some P2Y12 receptor inhibitor activity. A large retrospective trial also showed that morphine may increase mortality in patients with acute myocardial infarction (4, 5). Hypotension and bradycardia may also occur secondary to morphine use, but these complications can usually be overcome by prompt elevation of the lower extremities.
Standard therapy for all patients with unstable angina includes beta-blockers, ACE inhibitors, and statins. Beta-blockers are recommended unless contraindicated (eg, by bradycardia, heart block, hypotension, or asthma), especially for high-risk patients. Beta-blockers reduce heart rate, arterial pressure, and contractility, thereby reducing cardiac workload and oxygen demand. ACE inhibitors may provide long-term cardioprotection by improving endothelial function. If an ACE inhibitor is not tolerated because of cough or rash (but not angioedema or renal dysfunction), an may be substituted. Statins are also standard therapy regardless of lipid levels and should be continued indefinitely.
Reperfusion therapy in unstable angina
Fibrinolytic drugs, which can be helpful in patients with STEMI, do not benefit patients with unstable angina.
Angiography is typically done during admission—within 24 to 48 hours of admission if the patient is stable or immediately in unstable patients (eg, with ongoing symptoms, hypotension, sustained arrhythmias). Angiographic findings help determine whether PCI or coronary artery bypass grafting (CABG) is indicated. Choice of reperfusion strategy is further discussed in Revascularization for Acute Coronary Syndromes.
Pearls & Pitfalls
|
Rehabilitation and post-discharge treatment
Functional evaluation
Changes in lifestyle: Regular exercise, diet modification, weight loss, smoking cessation
Medications: Continuation of antiplatelets, beta-blockers, ACE inhibitors, and statins
Patients who did not have coronary angiography during admission, have no high-risk features (eg, heart failure, recurrent angina, ventricular tachycardia or ventricular fibrillation after 24 hours, mechanical complications such as new murmurs, shock), and have an ejection fraction > 40% usually should have stress testing of some sort before or shortly after discharge.
The acute illness and treatment of unstable angina should be used to strongly motivate the patient to modify risk factors. Evaluating the patient’s physical and emotional status and discussing them with the patient, advising about lifestyle (eg, smoking, diet, work and play habits, exercise), and aggressively managing risk factors may improve prognosis.
On discharge, all patients should be continued on appropriate antiplatelets, statins, antianginals, and other medications based on comorbidities.
Treatment references
1. Nakayama N, Yamamoto T, Kikuchi M, et al: Prehospital Administration of Aspirin and Nitroglycerin for Patients With Suspected Acute Coronary Syndrome—A Systematic Review. Circ Rep 4(10):449–457, 2022. doi:10.1253/circrep.CR-22-0060
2. Antithrombotic Trialists' Collaboration: Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients [published correction appears in BMJ 2002 Jan 19;324(7330):141]. BMJ 324(7329):71–86, 2002. doi:10.1136/bmj.324.7329.71
3. Amsterdam EA, Wenger NK, Brindis RG, et al: 2014 AHA/ACC Guideline for the Management of Patients With Non–ST-Elevation Acute Coronary Syndromes. J Am Coll Cardiol 64 (24):e139–e228, 2014. doi: 10.1016/j.jacc.2014.09.017
4. Kubica J, Adamski P, Ostrowska M, et al: Morphine delays and attenuates ticagrelor exposure and action in patients with myocardial infarction: the randomized, double-blind, placebo-controlled IMPRESSION trial. Eur Heart J 37(3):245–252, 2016. doi: 10.1093/eurheartj/ehv547
5. Meine TJ, Roe MT, Chen AY, et al: Association of intravenous morphine use and outcomes in acute coronary syndromes: results from the CRUSADE Quality Improvement Initiative. Am Heart J 149(6):1043-1049, 2005. doi 10.1016/j.ahj.2005.02.010
Prognosis for Unstable Angina
Prognosis after an episode of unstable angina depends upon how many coronary arteries are diseased, which arteries are affected, and how severely they are affected. For example, stenosis of the proximal left main artery or equivalent (proximal left arterial descending and circumflex artery stenosis) has a worse prognosis than does distal stenosis or stenosis in a smaller arterial branch. Left ventricular function also greatly influences prognosis; the presence of significant left ventricular dysfunction (even with 1- or 2-vessel disease) warrants a lower threshold for revascularization.
Overall, a substantial proportion of patients with unstable angina have a myocardial infarction within 3 months of onset; sudden death is less common (see table Risk of Adverse Events at 14 Days in Unstable Angina or NSTEMI). Marked ECG changes with chest pain indicate higher risk of subsequent MI or death.
Key Points
Unstable angina is new, worsening, or rest angina in patients whose cardiac biomarkers do not meet criteria for myocardial infarction.
Symptoms of unstable angina include new or worsening chest pain or chest pain occurring at rest.
Diagnosis is based on serial ECGs and cardiac biomarkers.
Immediate treatment includes oxygen, antianginals, antiplatelets, and anticoagulants.
For patients with ongoing symptoms, hypotension, or sustained arrhythmias, do immediate angiography.
For stable patients, do angiography within 24 to 48 hours of hospitalization.
Following recovery, initiate or continue antiplatelet agents, beta-blockers, angiotensin-converting enzyme inhibitors, and statins.







