




Enterobiasis is an intestinal infestation by the pinworm Enterobius vermicularis
(See also Approach to Parasitic Infections.)
As many as a billion people worldwide from all socioeconomic classes are infected. Pinworm infestation is the most common helminthic infection in the United States, occurring in an estimated 20 to 42 million people. Most cases are in school-aged and young children, their family members, or caregivers.
Pathophysiology of Pinworm Infestation
Pinworm ova become infective within a few hours of reaching the perineum. Infestation usually results from transfer of ova from the perianal area to fomites (clothing, bedding, furniture, rugs, toys, toilet seats), from which the ova are picked up by the new host, transmitted to the mouth, and swallowed. Thumb sucking is a risk factor. Reinfestation (autoinfestation) easily occurs through finger transfer of ova from the perianal area to the mouth. Pinworm infections have also been attributed to anilingus among adults.
Pinworms reach maturity in the lower gastrointestinal tract within 2 to 6 weeks. The female worm migrates out of the anus to the perianal region (usually at night) to deposit ova. The sticky, gelatinous substance in which the ova are deposited and the movements of the female worm cause perianal pruritus. The ova can survive on fomites as long as 3 weeks at normal room temperature.

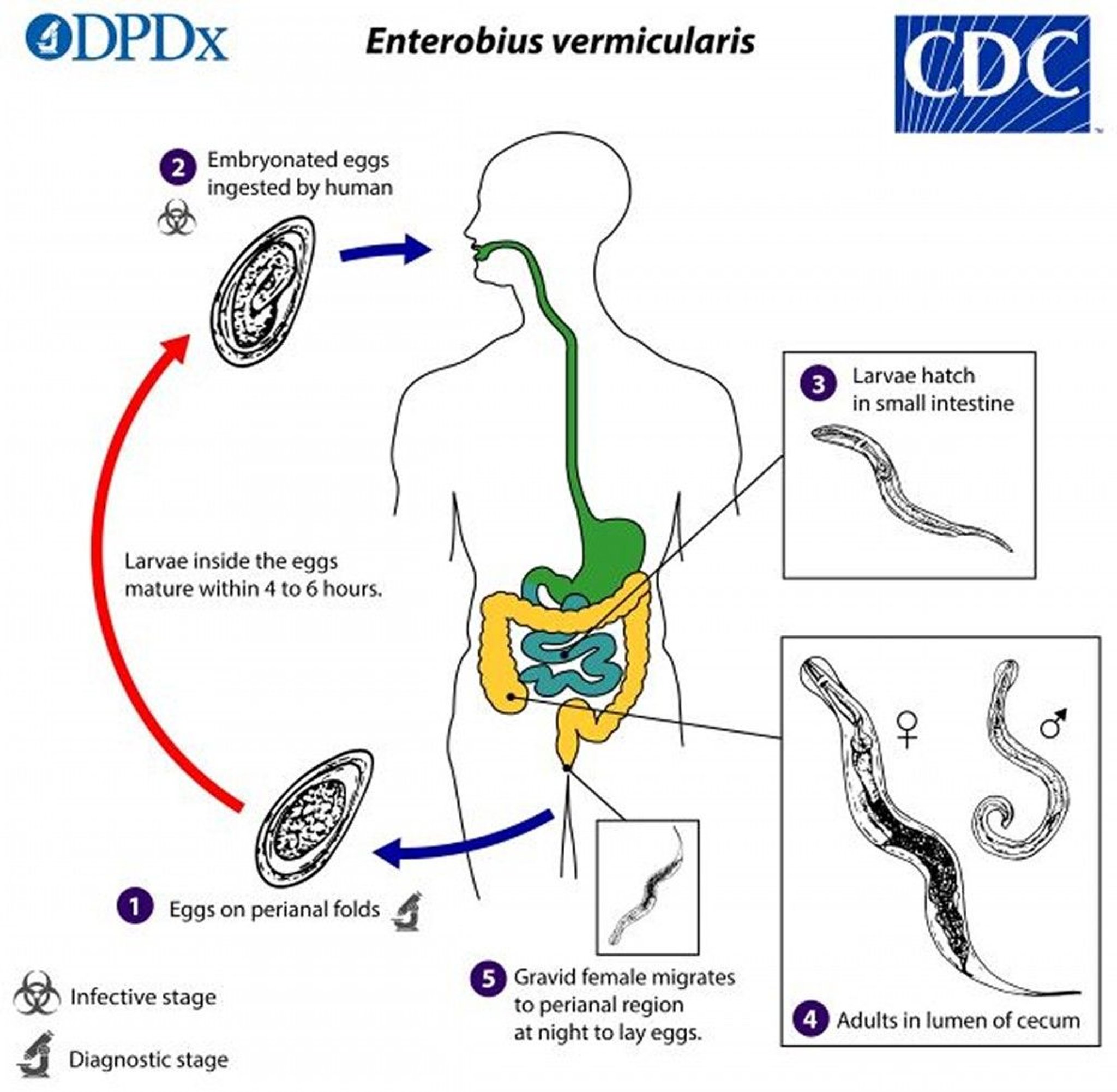
Image from the Centers for Disease Control and Prevention, Global Health, Division of Parasitic Diseases and Malaria.
Symptoms and Signs of Pinworm Infestation
Most infected people have no symptoms or signs, but some experience perianal pruritus and develop perianal excoriations from scratching. Secondary bacterial skin infection may occur. Rarely, migrating female worms ascend the human female genital tract, causing vaginitis and, even less commonly, peritoneal lesions.
Many other conditions (eg, abdominal pain, insomnia, seizures) have been attributed to pinworm infestation, but a causal relationship is unlikely. Pinworms have been found obstructing the appendiceal lumen in cases of appendicitis, but the presence of the parasites may be coincidental.
Diagnosis of Pinworm Infestation
Examination of the perianal region for worms, ova, or both
Pinworm infestation can be diagnosed by finding the female worm, which is 8 to 13 mm long (males are 2 to 5 mm), in the perianal region 1 or 2 hours after a child goes to bed at night or in the morning or by using a low-power microscope to identify ova on cellophane tape. Samples are obtained in the early morning before the child arises by patting the perianal skinfolds with a strip of cellophane tape, which is then placed sticky side down on a glass slide and viewed microscopically. The 50- by 30-micron ova are oval with a thin shell that contains a curled-up larva. A drop of toluene placed between tape and slide dissolves the adhesive and eliminates air bubbles under the tape, which can hamper identification of the ova. This procedure should be repeated on 3 successive mornings if necessary.
On occasion, the diagnosis can be made by examining samples taken from under the patient's fingernails.
Eggs may also be encountered, but less frequently, in stool, urine, or vaginal smears.
Treatment of Pinworm Infestation
Because pinworm infestation is seldom harmful, prevalence is high, and reinfestation is common, treatment is indicated only for symptomatic infections. However, most parents actively seek treatment when their children have pinworms.
A single dose of any of the following, repeated in 2 weeks, is effective in eradicating pinworms (but not ova) in > 90% of cases:
Carbolated petrolatum (ie, containing carbolic acid) or other antipruritic creams or ointments applied to the perianal region may relieve itching.
Prevention of Pinworm Infestation
Pinworm reinfestation is common because viable ova may be excreted for 1 week after therapy, and ova deposited in the environment before therapy can survive 3 weeks. Multiple infestations within the household are common, and treatment of the entire family may be necessary.
The following can help prevent the spread of pinworm:
Washing the hands with soap and warm water after using the toilet, after changing diapers, and before handling food (the most successful way)
Frequently washing clothing, bedding, and toys
If people are infected, showering every morning to help remove eggs on the skin
Vacuuming the environment to try to eliminate eggs
Avoidance of oral-anal contact during sex
Key Points
Pinworm infestation is the most common helminthic infection in the United States; most cases occur in school-aged or younger children, in adults who care for children, or in family members of an infected child. Infections also occur in institutionalized people and those who have oral-anal contact during sex.
Pinworm infestation is seldom harmful, and reinfestation is common.
Ova deposited in the environment can survive 3 weeks.
Pinworm eggs may be ingested when people touch their mouth after they scratch their perianal area or after they handle contaminated clothes or other objects (eg, bed linens).
Most infected people have no symptoms or signs, but some experience perianal pruritus.
Diagnose pinworm infestation by collecting ova in the morning on cellophane tape and using a low-power microscope to identify them; diagnosis can also be made by finding the female worm in the perianal region 1 or 2 hours after a child goes to bed at night.







