




Atrial fibrillation and atrial flutter are very fast electrical discharge patterns that make the atria (upper chambers of the heart) contract very rapidly, with some of the electrical impulses reaching the ventricles and sometimes causing them to contract faster and less efficiently than normal.
These disorders often result from conditions that cause the atria to enlarge.
Symptoms depend on how fast the ventricles contract and may include awareness of heartbeats (palpitations), weakness, dizziness or light-headedness, shortness of breath, and chest pain.
Electrocardiography (ECG) confirms the diagnosis.
Treatment includes medications to slow the ventricles’ contractions and sometimes medications or electrical shocks (cardioversion) to restore normal heart rhythm.
(See also Overview of Abnormal Heart Rhythms.)
Atrial fibrillation and atrial flutter are more common among older adults and people who have a heart disorder. Atrial fibrillation is much more common than atrial flutter. Many people with atrial flutter also have episodes of atrial fibrillation. Atrial fibrillation and atrial flutter may come and go or be sustained.
Atrial fibrillation
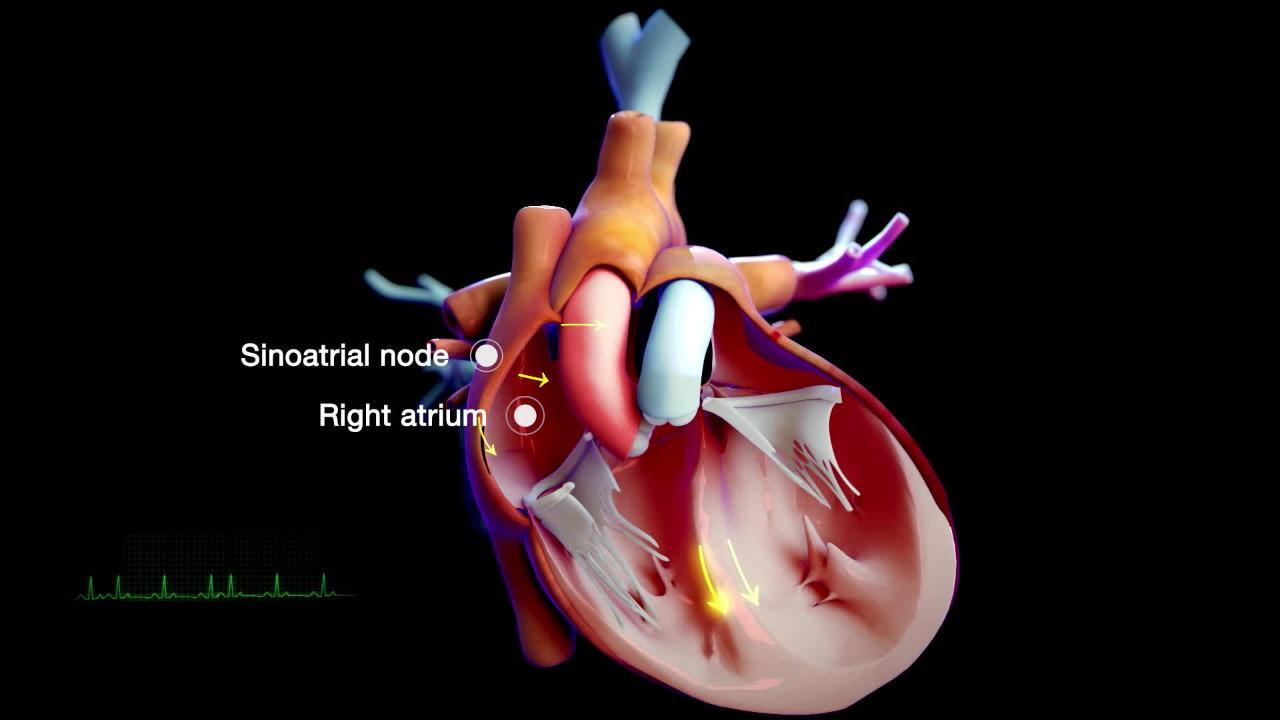
During atrial fibrillation, electrical impulses are triggered from many areas in and around the atria rather than just one area (the sinoatrial node—see figure Tracing the Heart's Electrical Pathway). The resulting electrical activity is chaotic rather than organized and thus, the atrial walls quiver rather than contract. Because the atria do not contract normally, they do not help pump blood into the ventricles. When the atria do not help pump blood to the ventricles, the maximum amount of blood that the heart pumps is reduced by about 10%. This slightly lower maximum output is usually not a problem except in people who have heart disease, particularly when they exert themselves.
Only some, and unpredictable numbers, of the chaotic electrical impulses are conducted through the atrioventricular node to the ventricles. Thus, the ventricles beat irregularly. For most people who are not being treated for atrial fibrillation, the impulses are conducted to the ventricles at a faster-than-normal rate (often 140 to 160 times per minute, compared to the normal heart rate of about 60 to 100 beats per minute). Even faster rates occur during exercise.
Atrial flutter
During atrial flutter, unlike in atrial fibrillation, electrical activity in the atria is coordinated. Thus, the atria do contract, but at a very rapid rate (250 to 350 times per minute). This rate is too fast to allow every impulse to be conducted through the atrioventricular node to the ventricles. For most people who are not being treated, every second atrial impulse gets to the ventricules, resulting in a ventricular rate of about 150 beats per minute.
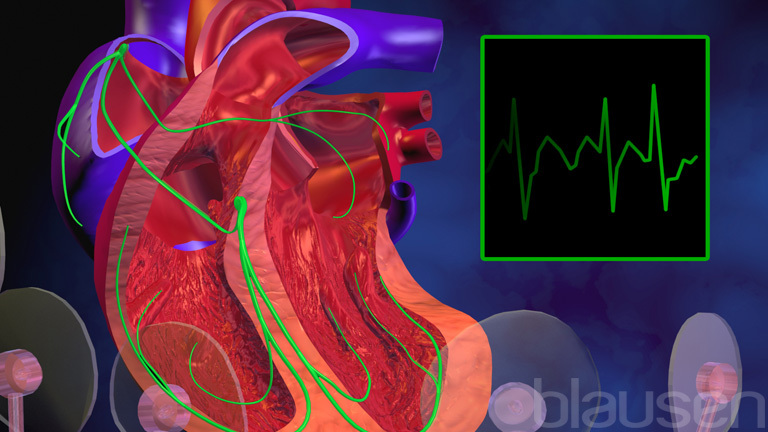
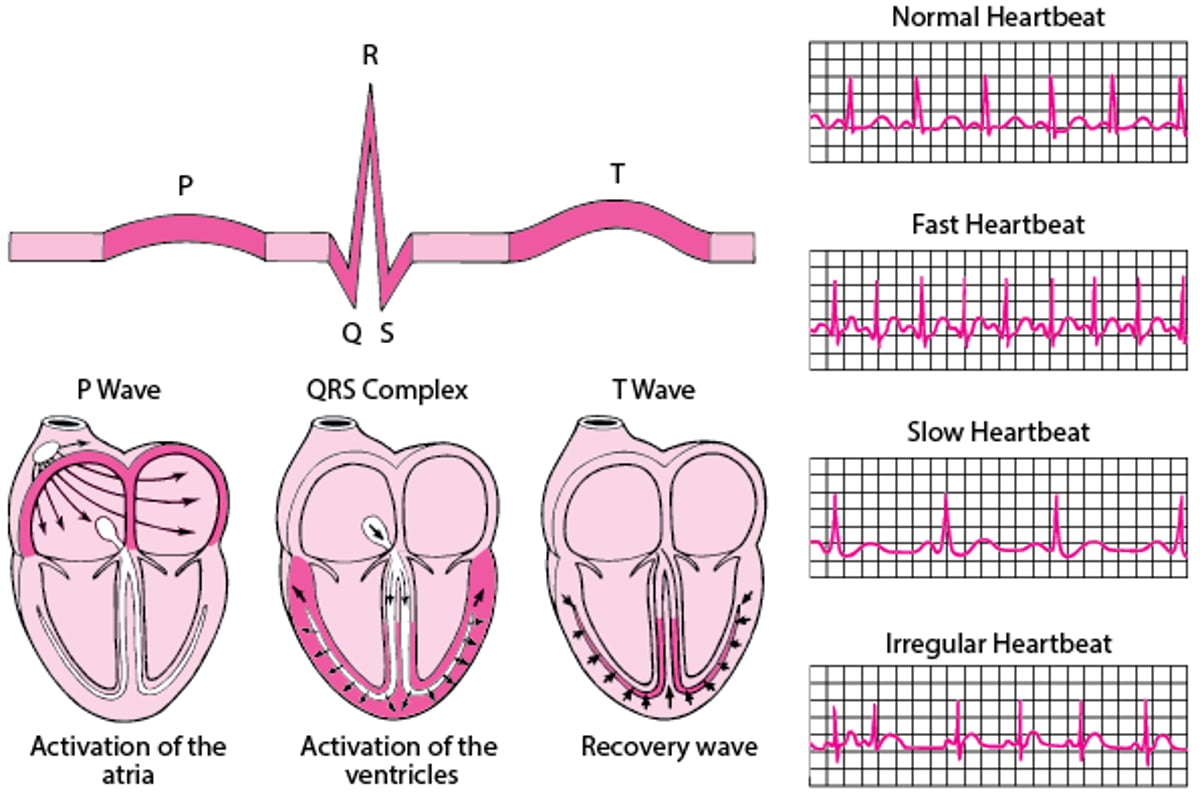
ECG: Reading the Waves
An electrocardiogram (ECG) represents the electrical current moving through the heart during a heartbeat. The current's movement is divided into parts, and each part is given an alphabetic designation in the ECG. Each heartbeat begins with an impulse from the heart's pacemaker (sinus or sinoatrial node). This impulse activates the upper chambers of the heart (atria). The P wave represents activation of the atria. Next, the electrical current flows down to the lower chambers of the heart (ventricles). The QRS complex represents activation of the ventricles. The ventricles must then undergo an electrical change to get ready for the next heart beat. This electrical activity is called the recovery wave, which is represented by the T wave. Many kinds of abnormalities can often be seen on an ECG. They include a previous heart attack (myocardial infarction), an abnormal heart rhythm (arrhythmia), an inadequate supply of blood and oxygen to the heart (ischemia), and excessive thickening (hypertrophy) of the heart's muscular walls. Certain abnormalities seen on an ECG can also suggest bulges (aneurysms) that develop in weaker areas of the heart's walls. Aneurysms may result from a heart attack. If the rhythm is abnormal (too fast, too slow, or irregular), the ECG may also indicate where in the heart the abnormal rhythm starts. Such information helps doctors begin to determine the cause. |

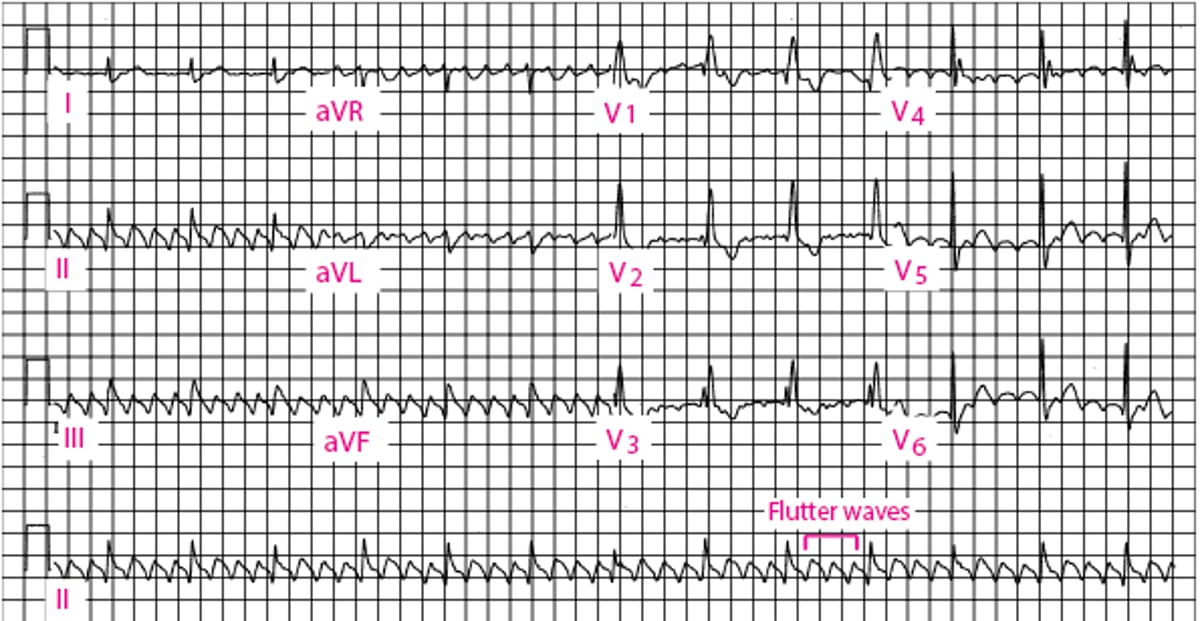
Atrial Flutter
The bigger deflections are QRS complexes, which represent the activity of the ventricules (the bottom heart chambers). The smaller deflections represent activity of the atria (the upper heart chambers). The smaller deflections show atrial flutter deflections that are rapid (300 atrial beats per minute), regular in timing, and regular in shape, with a characteristic sawtooth pattern. The larger deflections show the ventricular response to the atrial flutter and, in this case, are regular at 75 ventricular beats per minute. |

Atrial Fibrillation
The bigger deflections are QRS complexes, which represent the activity of the ventricles (the bottom heart chambers). The smaller deflections represent the activity of the atria (the upper heart chambers). The smaller deflections are only visible in the lead labeled V1 (which is the closest lead to the upper heart chambers) and show atrial fibrillation deflections that are very rapid (more than 300 per minute), irregular in timing, and irregular in shape. The larger deflections show the ventricular response to the atrial fibrillation, are always irregular in timing, and, in this case, range from 60 to 150 ventricular beats per minute. |
Causes of Atrial Fibrillation and Atrial Flutter
Atrial fibrillation or atrial flutter may occur even when there is no other heart disorder. More often, these arrhythmias are caused by such conditions as
Heart valve disorders affecting the mitral and/or tricuspid valves
An overactive thyroid gland (hyperthyroidism)
Heart valve disorders and high blood pressure cause the atria to enlarge, making atrial fibrillation or atrial flutter more likely.
Complications
The main complications include the following:
Blood clots in the atria
Rapid heart rate, causing decreased heart output
In atrial fibrillation or atrial flutter, the atria do not empty completely into the ventricles with each beat. Over time, some blood inside the atria may stagnate, and blood clots may form. Pieces of the clot may break off, often shortly after atrial fibrillation converts back to normal rhythm—whether spontaneously or because of treatment. These pieces of clot may pass into the left ventricle, travel through the bloodstream (becoming emboli), and block a smaller artery. If pieces of a clot block an artery in the brain, a stroke results. Rarely, a stroke is the first sign of atrial fibrillation or atrial flutter.
When atrial fibrillation or atrial flutter causes the heart to beat too rapidly, the ventricles do not have enough time to fill completely with blood. Because they do not fill completely, the amount of blood pumped by the heart decreases. This decrease may cause the blood pressure to fall, and heart failure may occur.
Did You Know...
|
Symptoms of Atrial Fibrillation and Atrial Flutter
Symptoms of atrial fibrillation or atrial flutter depend largely on how fast the ventricles beat. When the ventricular rate is normal or only slightly increased (less than about 120 beats per minute), people usually have no symptoms. Higher rates cause unpleasant awareness of heart beats (palpitations), shortness of breath,or chest pain.
In people with atrial fibrillation, the pulse is usually rapid and is always irregular.
In people with atrial flutter, the pulse is usually rapid and can be regular or irregular.
The reduced pumping ability of the heart may cause weakness, faintness, and shortness of breath. When the ventricular rate is very fast, some people, especially older adults and those with heart disorders, develop heart failure or chest pain. Very rarely, such people may develop shock (very low blood pressure).
Diagnosis of Atrial Fibrillation and Atrial Flutter
Electrocardiography
Symptoms suggest the diagnosis of atrial fibrillation or atrial flutter, and electrocardiography (ECG) confirms it.
Ultrasound of the heart (echocardiography) is done. It enables doctors to evaluate the heart valves and look for blood clots in the atria.
Doctors usually also do blood tests to look for an overactive thyroid gland.
Treatment of Atrial Fibrillation and Atrial Flutter
Slowing the heart rate
Anticoagulants
Restoring normal heart rhythm
Ablation
Treatment of atrial fibrillation or atrial flutter is designed to control the rate at which the ventricles contract, to restore the normal rhythm of the heart, and to treat the disorder causing the arrhythmia. Medications to prevent the formation of blood clots and emboli (anticoagulants) are usually given.
Treatment of the underlying disorder is important but does not always alleviate atrial fibrillation or atrial flutter. However, treatment of an overactive thyroid gland or surgery to correct a heart valve disorder or a birth defect of the heart may help.
Slowing the heart rate
Restoring normal heart rhythm
Atrial fibrillation or atrial flutter may spontaneously convert to a normal rhythm. In some people, these arrhythmias must be immediately converted to a normal rhythm by applying electricity (cardioversion). Such people include those in whom the atrial fibrillation or atrial flutter causes heart failure or other symptoms of low heart output.
Before restoring normal rhythm, because there is a risk that a blood clot will break off and cause a stroke during conversion, measures must be taken to prevent blood clots.
Methods of conversion include
Electrical shock (synchronized cardioversion)
Medications
An electrical shock to the heart is the most effective approach. The electrical shock is synchronized to be given only at a certain point in the heart's electrical activity (synchronized cardioversion) so that it does not cause ventricular fibrillation. Cardioversion is effective in 70 to 90% of people.
Certain antiarrhythmic medicationsSome Medications Used to Treat Arrhythmias) also may restore a normal rhythm. However, these medications are effective in only about 25 to 65% of people and often cause side effects.
Conversion to a normal rhythm by any means becomes less likely the longer the arrhythmia has been present (especially after 6 months or more), the larger the atria become, and the more severe the underlying heart disorder becomes. When conversion is successful, the risk of recurrence is high, even if people are taking a medication to prevent recurrence (typically one of the same medications used to convert the arrhythmia to a normal rhythm).
Ablation procedures
Rarely, when all other treatments of atrial fibrillation are ineffective, the atrioventricular node can be destroyed by an ablation procedure. Ablation is a process to kill a specific area of abnormal tissue using energy from radiofrequency waves, lasers, or electrical current, or by applying very cold temperatures. Energy is applied using a catheter inserted into the heart.
By destroying the atrioventricular node, this ablation procedure completely stops conduction from the atria to the ventricles. Thus, although the atria continue to fibrillate, the ventricular rate slows down. However, a permanent artificial pacemaker is required to activate the ventricles afterward.
Another type of ablation procedure for atrial fibrillation destroys atrial tissue near the pulmonary veins (pulmonary vein isolation). Pulmonary vein isolation spares the atrioventricular node and can stop the atrial fibrillation but is less often successful (60 to 80%), and the risk of serious complications is significant (1 to 5%). Accordingly, this procedure is often reserved for the best candidates (for example, younger people who have no significant heart disease like a heart valve disorder, people without other options such as those with atrial fibrillation that does not respond to medications, or people with heart failure).
For people who have atrial flutter, ablation may be used to interrupt the flutter circuit in the atrium and permanently re-establish normal rhythm. This procedure is successful in about 90% of people.
Preventing blood clots
Measures to prevent blood clots (and thus prevent stroke) are necessary in the vast majority of people when atrial fibrillation or atrial flutter is converted back to normal rhythm. Most people also need such measures during long-term treatment. Doctors typically give an anticoagulantfactor Xa
The decision regarding the need for an anticoagulant,the type of anticoagulant to be prescribed, and the duration of treatment depends on the specific underlying heart disease, if any, and on the presence or absence of one or more risk factors for developing stroke. Such risk factors include
Age 65 years or older
High blood pressure
Diabetes
Certain heart disorders, including heart failure, rheumatic mitral stenosis, presence of a mechanical artificial heart valve
A previous stroke or transient ischemic attack
Disease affecting the blood vessels
Being female
More Information
The following English-language resource may be useful. Please note that The Manual is not responsible for the content of this resource.
American Heart Association: Atrial fibrillation: Information about symptoms and diagnosis of atrial fibrillation and resources for people living with atrial fibrillation







