




Body fluid volume and electrolyte concentration are normally maintained within very narrow limits despite wide variations in dietary intake, metabolic activity, and environmental stresses. Homeostasis of body fluids is preserved primarily by the kidneys.

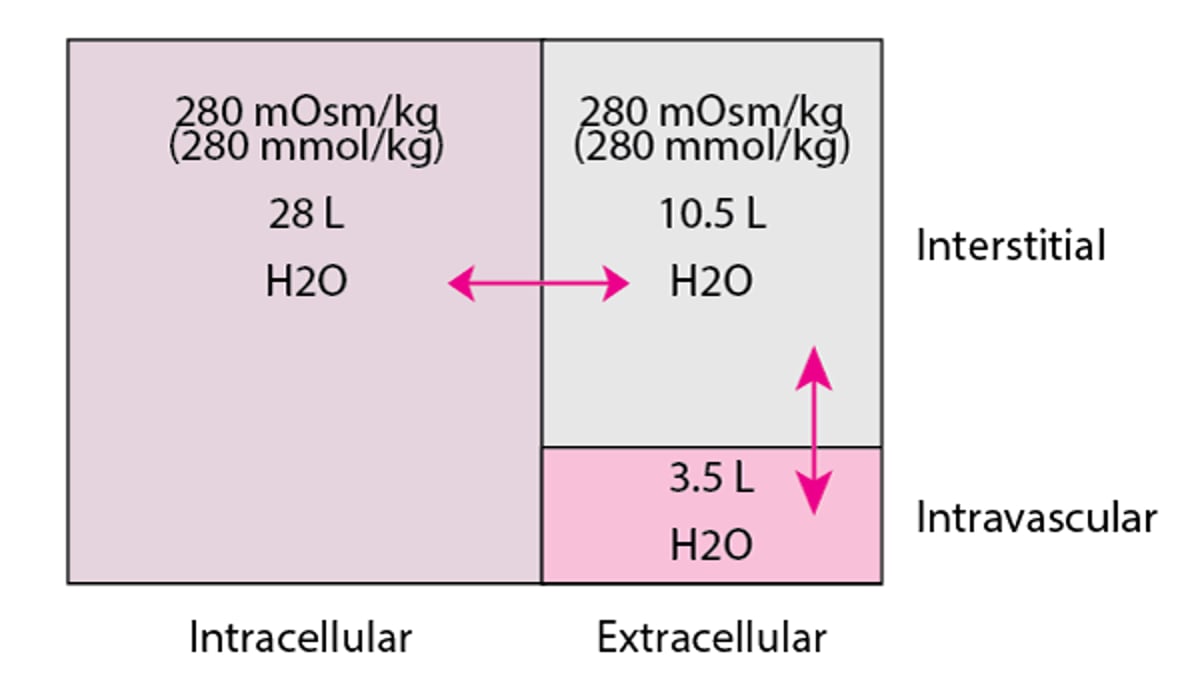
Approximately 60% of body weight in men and approximately 50% in women is made up of water (ranging from approximately 50% in people with obesity to 70% in people within or below normal body mass index). The percentage of body weight that is water is higher (70%) at birth and in early childhood. Almost two thirds of total body water (TBW) is in the intracellular compartment (intracellular fluid, or ICF); the other one third is extracellular (extracellular fluid, or ECF). Normally, approximately 25% of the ECF is in the intravascular compartment; the other 75% is interstitial fluid (see figure Fluid Compartments in an Average 70-kg Man).
Fluid compartments in an average 70-kg man
Total body water = 70 kg × 0.60 = 42 L (280 mOsm/kg [280 mmol/kg]). |

Fluid in the various compartments of the body vary in their electrolyte composition. The major intracellular cation is potassium. The major extracellular cation is sodium. Concentrations of intracellular and extracellular cations are as follows:
Intracellular potassium concentration averages 140 mEq/L (140 mmol/L).
Extracellular potassium concentration is 3.5 to 5 mEq/L (3.5 to 5 mmol/L).
Intracellular sodium concentration is 12 mEq/L (12 mmol/L).
Extracellular sodium concentration averages 140 mEq/L (140 mmol/L).
Osmotic forces
The concentration of combined solutes in water is osmolarity (amount of solute per L of solution), which, in body fluids, is similar to osmolality (amount of solute per kg of solution). Water crosses cell membranes freely from areas of low solute concentration to areas of high solute concentration. Thus, osmolality tends to equalize across the various body fluid compartments, resulting primarily from movement of water and not solutes. However, some solutes, such as urea, also freely diffuse across cell membranes and thus have little or no effect on water shifts (little or no osmotic activity). Other solutes, including several electrolytes, are restricted primarily to one fluid compartment and have the greatest osmotic activity. For example, sodium is restricted to the extracellular compartment and potassium to the intracellular. Osmolality of body fluids is normally between 275 and 290 mOsm/kg (275 and 290 mmol/kg) and can be measured directly in the laboratory or estimated according to the formula.
Estimated plasma osmolality is calculated in conventional units (mOsm/kg)


where serum sodium is expressed in mEq/L, and glucose and blood urea nitrogen (BUN) are expressed in mg/dL.
Estimated plasma osmolality can be calculated in SI units.
All values in this equation are expressed in mmol/L.
Sodium is the major determinant of plasma osmolality. Apparent changes in calculated osmolality may result from errors in the measurement of sodium, which can occur in patients with severe dyslipidemia or hyperproteinemia because the lipid or protein occupies space in the volume of serum taken for analysis; the concentration of sodium in serum itself is not affected. Methods of measuring serum electrolytes with direct ion-selective electrodes circumvent this problem.
An osmolar gap is present when measured osmolality exceeds estimated osmolality by ≥ 10 mOsm/kg ( ≥ 10 mmol/kg). It is caused by unmeasured osmotically active substances present in the plasma. The most common are alcohols (ethanol, methanol, isopropanol, ethylene glycol), mannitol, and glycine.
Tonicity is the effective osmolality of a fluid. The difference in tonicity between fluids in 2 compartments creates an osmotic force between them that promotes the movement of water from the compartment with lower tonicity into that with higher tonicity. In homeostasis, the osmotic activity of fluid is balanced between major compartments of the body, so relatively little net movement of fluid occurs between them. Osmotic force can shift water into or out of the same compartments. For example, plasma proteins have a small osmotic effect that along with serum sodium tends to draw water into the plasma; this osmotic effect is normally counter-balanced by vascular hydrostatic forces that drive water out of the plasma.
Water intake and excretion
Water intake is regulated by thirst. Thirst is triggered by receptors in the anterolateral hypothalamus that respond to increases in plasma osmolality or decreases in intravascular volume.
Water excretion by the kidneys is regulated primarily by vasopressin (argininevasopressin or antidiuretic hormone [ADH]). Vasopressin is released by the posterior pituitary and results in increased water reabsorption in the distal nephron. Vasopressin release is stimulated by any of the following:
Increased plasma osmolality
Decreased blood volume
Decreased blood pressure
Stress
Homeostasis is maintained as thirst-induced increased water intake decreases plasma osmolality. Low plasma osmolality in turn reduces thirst and inhibits vasopressin secretion, allowing the kidneys to once again produce dilute urine.
The average daily fluid intake is about 2.5 L. In healthy adults, the amount needed to replace losses from the urine and other sources is approximately 1 to 1.5 L/day. However, on a short-term basis, an average young adult with normal kidney function may ingest as little as 200 mL of water each day to excrete the nitrogenous and other wastes generated by cellular metabolism. More is needed in people with any loss of renal concentrating capacity. Renal concentrating capacity is lost in
Older adults
People with or , many forms of chronic kidney disease (CKD), hypercalcemia, severe salt restriction, chronic overhydration, or hyperkalemia
People who ingest ethanol
People with osmotic diuresis (eg, due to high-protein diets or hyperglycemia)
Other obligatory water losses are mostly insensible losses from the lungs and skin, averaging about 0.4 to 0.5 mL/kg/hour or about 650 to 850 mL/day in a 70-kg adult; patients who are febrile lose additional water due to increased metabolic rate. Gastrointestinal losses are usually negligible, except when marked vomiting, diarrhea, or both occur. Sweat losses can be significant during environmental heat exposure or excessive exercise.
The diluting capacity of healthy kidneys in young adults allows for a maximum daily fluid intake as much as 25 L; greater amounts quickly lower plasma osmolality.
Dehydration occurs when water intake (and a small amount produced by cellular respiration) is not adequate to replace water losses (excretion and insensible losses) (see Volume Depletion).
Rarely, a person cannot perceive thirst due to hypothalamic dysfunction when vasopressin release may be impaired by tumors or infiltrative disorders affecting the posterior pituitary, or by trauma to the brain. In many cases, a specific cause cannot be identified. (See also .)







