


Thoracentesis is needle aspiration of fluid from a pleural effusion.
Thoracentesis may be done for diagnosis and/or therapy.
Indications for Thoracentesis
Thoracentesis can be performed for diagnostic or therapeutic purposes:
To determine the etiology of pleural fluid that is new or of uncertain etiology (see figure Diagnosis of Pleural Effusion)
To relieve symptoms in patients with dyspnea caused by a large pleural effusion
Thoracentesis is usually not needed when the etiology of the pleural fluid is apparent (eg, viral pleuritis, typical heart failure) and the pleural effusion is either asymptomatic or can be treated more conservatively (eg, such as with diuretics).
The selection of laboratory tests typically done on pleural fluid is discussed in pleural effusion.
Pleurodesis (injection of an irritating substance into the pleural space, which causes obliteration of the space) may be done after several therapeutic thoracenteses to help prevent recurrence of pleural fluid accumulation, such as in malignant effusions.
Contraindications to Thoracentesis
Absolute contraindications:
None
Relative contraindications:
Bleeding disorder or anticoagulation
Altered chest wall anatomy
Cellulitis or herpes zoster at the site of thoracentesis puncture
Pulmonary disease severe enough to make complications life threatening
Uncontrolled coughing or an uncooperative patient
Complications of Thoracentesis
Major complications include:
Bleeding (hemoptysis due to lung puncture)
Infection
Re-expansion pulmonary edema and/or hypotension (1)
Hemothorax due to damage to intercostal vessels
Puncture of the spleen or liver
Vasovagal syncope
Equipment for Thoracentesis
Mask and protective eyewear, drapes, and gloves
Local anesthetic (eg, 10 mL of 1% lidocaine), 25-gauge and 20- to 22-gauge needles, and 10-mL syringeLocal anesthetic (eg, 10 mL of 1% lidocaine), 25-gauge and 20- to 22-gauge needles, and 10-mL syringe
Antiseptic solution for cleansing the skin with applicators
Thoracentesis needle (16- to 19-gauge) and plastic catheter
3-way stopcock
30- to 50-mL syringe
Wound dressing materials such as tape, gauze pads and/or petrolatum dressing
Bedside table for patient to lean on
Appropriate containers for collection of fluid for laboratory tests
Collection bags for removal of larger volumes
Ultrasound machine
Additional Considerations for Thoracentesis
Thoracentesis can be safely done at the patient’s bedside or in an outpatient setting.
Ample local anesthetic is necessary, but pre-procedural sedation is not required in cooperative patients.
The thoracentesis needle should not be inserted through infected skin (eg, cellulitis or herpes zoster).
Positive pressure ventilation can increase the risk of complications.
If the patient is receiving anticoagulant medications (eg, warfarin), consider giving fresh frozen plasma or another reversal agent prior to the procedure.If the patient is receiving anticoagulant medications (eg, warfarin), consider giving fresh frozen plasma or another reversal agent prior to the procedure.
Hemorrhagic complications are infrequent after ultrasound-guided thoracentesis in patients with abnormal preprocedural coagulation parameters (2).
Bloody fluid that does not clot in a collecting tube indicates that blood in the pleural space was not iatrogenic, because free blood in the pleural space rapidly defibrinates.
Only unstable patients and patients at high risk of decompensation due to complications require monitoring (eg, pulse oximetry, electrocardiography [ECG]).
If suspicion is high for an empyema or complicated parapneumonic effusion, or if there is significant risk of hemothorax, tube or catheter thoracostomy should be considered rather than thoracentesis.
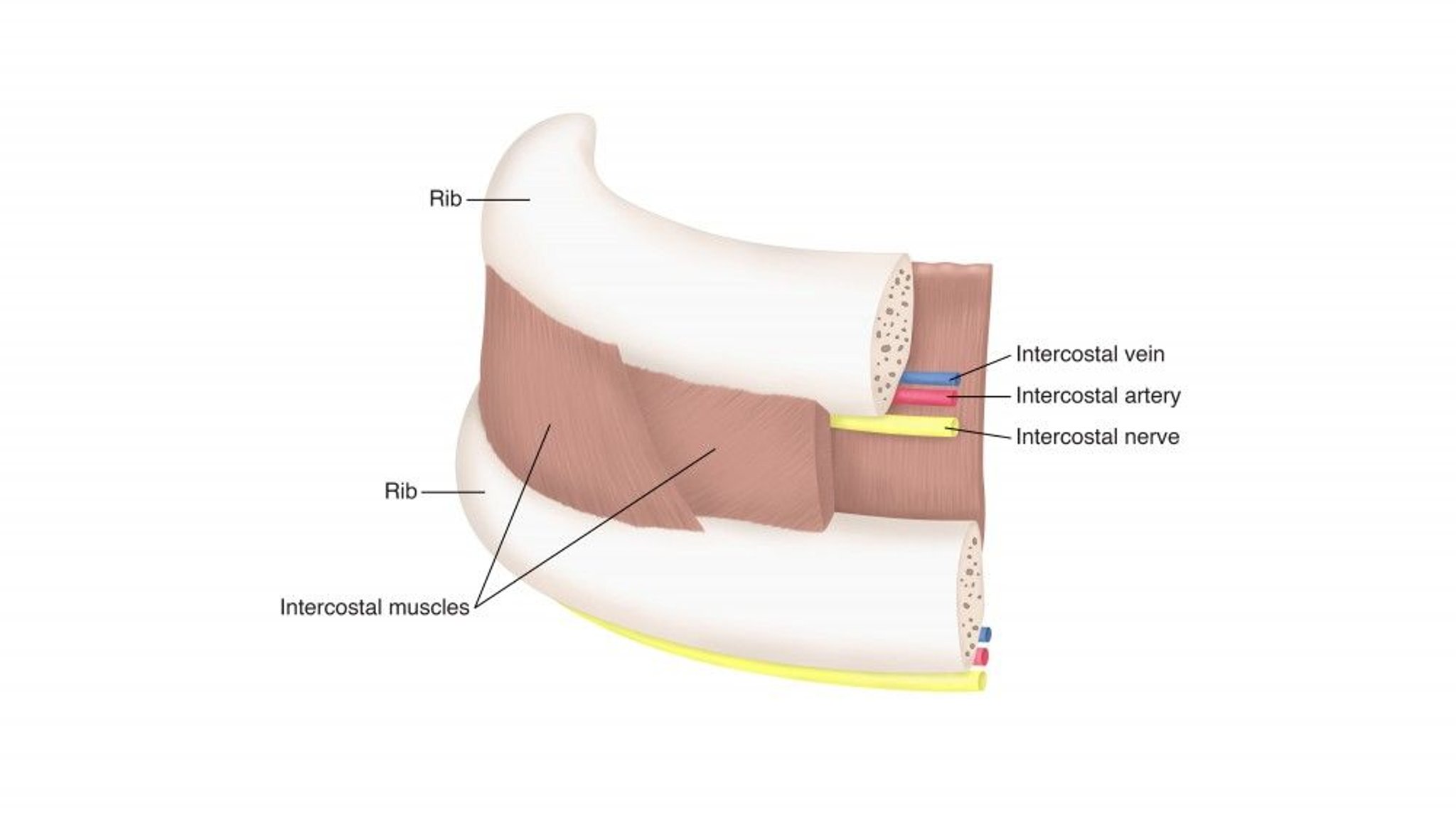
Relevant Anatomy for Thoracentesis
The intercostal neurovascular bundle is located along the lower edge of each rib. Therefore, the needle must be placed over the upper edge of the rib to avoid damage to the neurovascular bundle.

Positioning for Thoracentesis
Thoracocentesis is best done with the patient sitting upright and leaning slightly forward with arms supported; this position helps to separate the ribs.
Recumbent or supine thoracentesis (eg, in a ventilated patient) is possible but best done using ultrasound or CT to guide needle insertion.
Step-by-Step Description of Thoracentesis

Confirm the extent of the pleural effusion by chest percussion and consider an imaging study; bedside ultrasound is recommended both to reduce the risk of pneumothorax and to increase the success of the procedure (3). The procedure can be performed with the use of ultrasound initially to determine location of effusion, or ultrasound can be used during the entire procedure.
Select a needle insertion point in the mid-scapular line at the upper border of the rib one intercostal space below the top of the effusion.
Identify and mark the insertion point.
Prepare the area with a skin cleansing agent (eg, chlorhexidine pad, povidone-iodine). Prepare the area with a skin cleansing agent (eg, chlorhexidine pad, povidone-iodine).
While wearing sterile gloves, apply a sterile drape.
Using a 25-gauge needle, place a wheal of local anesthetic over the insertion point. Switch to a larger (20- or 22-gauge) needle and inject anesthetic progressively deeper until reaching the parietal pleura, which should be infiltrated the most because it is very sensitive. Continue advancing the needle until pleural fluid is aspirated and note the depth of the needle at which this occurs; this can be done with ultrasound guidance.
Attach a large-bore (16- to 19-gauge) thoracentesis needle-catheter device to a 3-way stopcock, place a 30- to 50-mL syringe on one port of the stopcock and attach drainage tubing to the other port.
Insert the needle along the upper border of the rib while aspirating and advance it into the effusion; this can be done with ultrasound guidance.
When fluid or blood is aspirated, insert the catheter over the needle into the pleural space and withdraw the needle, leaving the catheter in the pleural space. While preparing to insert the catheter, cover the needle opening during inspiration to prevent entry of air into the pleural space.
Withdraw 30 mL of fluid into the syringe and place the fluid in appropriate tubes and bottles for testing.
If a larger amount of fluid is to be drained, turn the stopcock and allow fluid to drain into a collection bag or bottle. Alternatively, aspirate fluid using the syringe, taking care to periodically release pressure on the plunger.
If a large amount of fluid (eg, > 500 mL) is withdrawn, monitor the patient's symptoms and blood pressure and stop drainage if the patient develops chest pain, dyspnea, or hypotension. Coughing is normal and represents lung re-expansion. Some clinicians recommend withdrawing no more than 1.5 L of pleural fluid in 24 hours, although there is little evidence that the risk of re-expansion pulmonary edema is directly proportional to the volume of fluid removed (1). Animal data suggest that rapidly draining long-standing effusions may lead to re-expansion pulmonary edema because of the decrease in surfactant that occurs in an atelectatic lung. Experienced operators may be able to completely drain effusions that are not long-standing in one procedure in properly monitored patients.
Remove the catheter while the patient is holding the breath or expiring. Apply a sterile dressing to the insertion site.
Aftercare for Thoracentesis
Sometimes imaging (usually chest radiograph or ultrasound) to exclude pneumothorax
Analgesia with oral nonsteroidal anti-inflammatory drugs (NSAIDs) or acetaminophen if neededAnalgesia with oral nonsteroidal anti-inflammatory drugs (NSAIDs) or acetaminophen if needed
Advise patients to report any shortness of breath or chest pain; coughing is common after fluid removal and not a cause for concern.
Evidence suggests that routine chest radiography is not necessary in asymptomatic patients, especially when an ultrasound-guided approach is used (4). Pneumothorax can also be excluded by the presence of lung sliding on multiple interspaces on ultrasound, but routine ultrasound is also not necessary (5). Post-procedural chest imaging is needed for any of the following:
The patient is mechanically ventilated
Air was aspirated
The needle was passed more than once
Symptoms or signs of pneumothorax develop
Warnings and Common Errors for Thoracentesis
Be sure to adequately anesthetize the parietal pleura to prevent perioperative pleurodynia.
Be sure to insert the thoracentesis needle just above the upper edge of the rib and not below the rib, to avoid the intercostal blood vessels and nerves at the lower edge of each rib.
Tips and Tricks for Thoracentesis
When marking the insertion point, use a skin marking pen or make an impression with a pen so that the skin cleansing method used will not remove the mark.
References
1. Feller-Kopman D, Berkowitz D, Boiselle P, et al: Large-volume thoracentesis and the risk of reexpansion pulmonary edema. Ann Thoracic Surg 84:1656–1662, 2007. doi:10.1016/j.athoracsur.2007.06.038
2. Hibbert RM, Atwell TD, Lekah A, et al: Safety of ultrasound-guided thoracentesis in patients with abnormal preprocedural coagulation parameters. Chest 144(2):456–463, 2013. doi: 10.1378/chest.12-2374
3. Barnes TW, Morgenthaler TI, Olson EJ, et al: Sonographically guided thoracentesis and rate of pneumothorax. J Clin Ultrasound 33(9): 1656–1661, 2005. doi:10.1002/jcu.20163
4. Singh K, Balthazar P, Duszak R Jr, Horný M, Hanna TN: Clinical Yield of Routine Chest Radiography after Ultrasound-Guided Thoracentesis. Acad Radiol 27(10):1379–1384, 2020. doi:10.1016/j.acra.2019.10.031
5. Gervais DA, Petersein A, Lee MJ, et al: US-guided thoracentesis: requirement for postprocedure chest radiography in patients who receive mechanical ventilation versus patients who breathe spontaneously. Radiology 204(2):503–506, 1997. doi:10.1148/radiology.204.2.9240544







