



Hypothermia is a core body temperature < 35° C. Symptoms progress from shivering and lethargy to confusion, coma, and death. Treatment for mild hypothermia is passive rewarming, using a warm environment and insulating blankets. Severe hypothermia requires active rewarming of both the body surface (eg, with forced-air warming systems, radiant sources) and the core (eg, with warm air inhalation, heated infusion and lavage, extracorporeal blood rewarming).

 Waves (V4)")
(See also Overview of Cold Injury.)
Primary hypothermia is widely underreported and can be classified as accidental (most common), homicidal, or suicidal. Secondary hypothermia, which is due to underlying medical conditions, may be underrecognized and has a significant effect on mortality risk in cardiovascular and neurologic disorders.
Etiology of Hypothermia
Hypothermia results when body heat loss exceeds body heat production. Hypothermia is most common during cold weather or immersion in cold water, but it may occur in warm climates when people lie immobile on a cool surface (eg, when they are intoxicated) or after very prolonged immersion in swimming-temperature water (eg, 20 to 24° C). Wet clothing and wind increase risk of hypothermia.
Conditions that cause loss of consciousness, immobility, or both (eg, trauma, hypoglycemia, seizure disorders, stroke, drug or alcohol intoxication) are common predisposing factors. Older adults and the very young also are at high risk:
Older adults often have diminished temperature sensation and impaired mobility and communication, resulting in a tendency to remain in an overly cool environment. These impairments, combined with diminished subcutaneous fat, contribute to hypothermia in older adults—sometimes even indoors in cool rooms.
The very young have similarly diminished mobility and communication and have an increased surface area/mass ratio, which enhances heat loss.
Pathophysiology of Hypothermia
Hypothermia slows all physiologic functions, including cardiovascular and respiratory systems, nerve conduction, mental acuity, neuromuscular reaction time, and metabolic rate. Thermoregulation ceases below about 30° C; the body must then depend on an external heat source for rewarming.
Renal cell dysfunction and decreased levels of vasopressin (ADH) lead to production of a large volume of dilute urine (cold diuresis). Diuresis plus fluid leakage into the interstitial tissues causes hypovolemia. Vasoconstriction, which occurs with hypothermia, may mask hypovolemia, which then manifests as sudden shock or cardiac arrest during rewarming (rewarming collapse) when peripheral vasculature dilates.
Immersion in cold water can trigger the diving reflex, which involves apnea, bradycardia, and increased peripheral vascular resistance; blood is shunted to essential organs (eg, heart, brain). The reflex is most pronounced in small children and may help protect them. Also, hypothermia due to total immersion in near-freezing water may protect the brain from hypoxia by decreasing metabolic demands. The decreased demand probably accounts for the occasional survival after prolonged cardiac arrest due to extreme hypothermia.
Symptoms and Signs of Hypothermia
Intense shivering occurs initially, but then progressively ceases, which allows body temperature to drop more precipitously. Central nervous system dysfunction progresses as the body temperature decreases; people do not sense the cold. Lethargy and clumsiness are followed by confusion, irritability, sometimes hallucinations, and eventually coma. Pupils may become unreactive. Respirations and heartbeat slow and ultimately cease. Initial sinus bradycardia is followed by slow atrial fibrillation; the terminal rhythm is ventricular fibrillation or asystole.
Diagnosis of Hypothermia
Core temperature measurement
Consideration of intoxication, myxedema, sepsis, hypoglycemia, and trauma
Diagnosis is by measuring core, not oral, temperature using an electronic thermometer. Rectal and esophageal probes are most accurate.
Temperature thresholds for classifying hypothermia severity vary. The Wilderness Medical Society Clinical Practice Guidelines uses the following (1):
Mild: 32 to 35°C
Moderate: 28 to 32°C
Severe: < 28°C
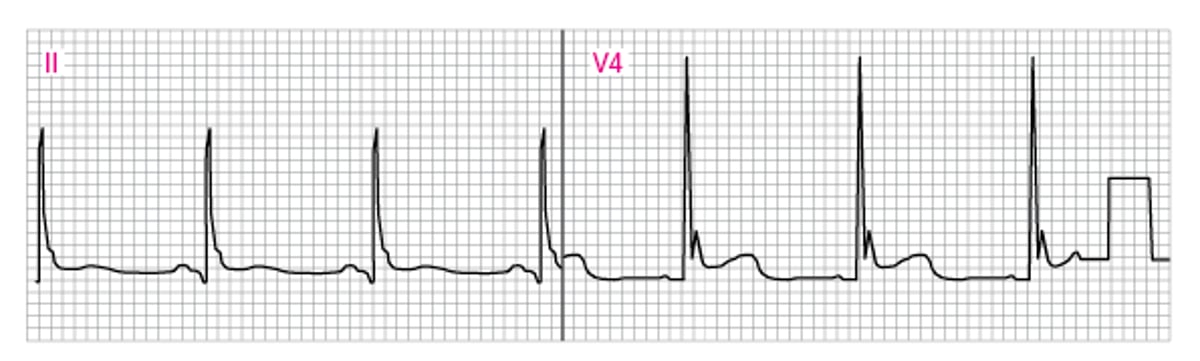
Laboratory tests include complete blood count, glucose (including bedside measurement), electrolytes, blood urea nitrogen, creatinine, and arterial blood gases (ABGs). ABGs are not corrected for low temperature. An electroencephalogram (EEG) may show J (Osborn) waves (see figure Abnormal ECG showing J [Osborn] waves [V4]) and interval prolongation (PR, QRS, QT).
If the cause of hypothermia is unclear, testing to detect contributing factors includes measuring a serum alcohol level, thyroid stimulating hormone (TSH), free thyroxine, and cortisol, as well as screening for other exposures (ie, certain medications and substances such as toxins or illicit drugs). Sepsis and occult head or skeletal trauma must be considered. Hypoadrenalism and hypothyroidism (including myxedema) can contribute to hypothermia and are often occult, with no history of cold intolerance, dry skin, arthralgias, or lassitude. Failure to rewarm is a clue. Myxedema characteristically prolongs the relaxation phase of the ankle reflex more than the contraction phase.
Abnormal ECG Showing J (Osborn) Waves (V4)
The J (Osborn) wave is visible as a hump at the junction of the QRS complex and ST segment. Computer programs cannot reliably differentiate J waveform abnormalities from myocardial injury current. |


Diagnosis reference
1. Dow J, Giesbrecht GG, Danzl DF, et al. Wilderness Medical Society Clinical Practice Guidelines for the Out-of-Hospital Evaluation and Treatment of Accidental Hypothermia: 2019 Update. Wilderness Environ Med. 30(4S):S47-S69, 2019. doi: 10.1016/j.wem.2019.10.002
Treatment of Hypothermia
Drying and insulation
Fluid resuscitation
Active rewarming unless hypothermia is mild, accidental, and uncomplicated
The first priority is to prevent further heat loss by removing wet clothing and insulating the patient. Subsequent measures depend on how severe hypothermia is and whether cardiovascular instability is present. Restoring a normal temperature is less urgent for patients with mild hypothermia than severe hyperthermia. For stable patients, elevating the core temperature by 1° C/hour is acceptable.
Fluid resuscitation is essential because patients are typically hypovolemic. Administer 500 cc to 2 L of 0.9% saline solution (20 mL/kg for children) IV; if possible, heat the solution to 40 to 42° C. More fluid is given as needed to maintain perfusion.
Pearls & Pitfalls
|
Passive rewarming
In mild hypothermia (temperature 32 to 35° C) with intact thermoregulation (indicated by shivering) (1), wrapping the patient in heated blankets and providing warm fluids to drink are adequate.
Active rewarming
Active rewarming is required if patients have any of the following:
Temperature < 32° C
Cardiovascular instability
Hormone insufficiency (such as hypoadrenalism or hypothyroidism)
Hypothermia secondary to trauma
Hypothermia secondary to toxins
Predisposing disorders
For moderate hypothermia (body temperature at the warmer end of the range, 28 to 32° C) (1) , external rewarming with forced hot air enclosures may be used. External heat is best applied to the thorax because warming the extremities may increase metabolic demands on a depressed cardiovascular system.
For severe hypothermia (body temperatures < 28° C) (1), core rewarming is required, particularly for those with low blood pressure or cardiac arrest.
Core rewarming options include
Inhalation
IV infusion
Lavage
Extracorporeal core rewarming (ECR)
Providing heated (40 to 45° C), humidified oxygen via face mask or endotracheal tube eliminates respiratory heat loss and can add 1 to 2° C/hour to the rewarming rate.
IV crystalloids or blood should be heated to 40 to 42° C, especially with massive volume resuscitations.
Closed thoracic lavage through 2 thoracostomy tubes (see How To Do Tube and Catheter Thoracostomy) is very efficient in severe cases. Peritoneal lavage with dialysate heated to 40 to 45° C, using 2 catheters with outflow suction, is especially useful for severely hypothermic patients with rhabdomyolysis, toxin ingestion, or electrolyte abnormalities. Heated lavage of the bladder or gastrointestinal tract transfers only minimal heat.
Several types of extracorporeal life support may be options, including hemodialysis, venovenous (V-V) or continuous venoarterial (V-A) extracorporeal membrane oxygenation (ECMO), and cardiopulmonary bypass. These measures require a prearranged protocol with appropriate specialists. Although intuitively attractive and heroic, such measures are not routinely available or commonly used in many hospitals.
Cardiopulmonary resuscitation (CPR)
Hypotension and bradycardia are expected when core temperature is low. If these symptoms are due solely to hypothermia, they need not be aggressively treated.
Endotracheal intubation after oxygenation, when needed, must be done gently to avoid precipitating a nonperfusing cardiac arrhythmia.
CPR should be withheld if patients have a perfusing rhythm unless true cardiac arrest is confirmed by absence of cardiac motion on bedside cardiac ultrasonography. Treat with fluids and active rewarming. Chest compressions are not done, because
Pulses may quickly return with rewarming
Chest compressions may convert the perfusing rhythm to a nonperfusing rhythm
Patients with a nonperfusing rhythm (ventricular fibrillation or asystole) require CPR with chest compressions and endotracheal intubation. Successful defibrillation is difficult if body temperature is low; 1 attempt at maximum energy setting for the defibrillator (200 J for biphasic and 360 J for monophasic) may be made but, if ineffective, further attempts are generally deferred until the temperature reaches > 30° C.
Advanced cardiac life-support medications (eg, antiarrhythmics, vasopressors, inotropes) are usually not given until the temperature reaches > 30° C. Low-dose dopamine (1 to 5 mcg/kg/min) or other catecholamine infusions are typically reserved for patients with disproportionately severe hypotension who do not respond to fluid resuscitation and rewarming (30° C. Low-dose dopamine (1 to 5 mcg/kg/min) or other catecholamine infusions are typically reserved for patients with disproportionately severe hypotension who do not respond to fluid resuscitation and rewarming (2).
Advanced life support should be continued until the temperature reaches 32° C unless obviously lethal injuries or disorders are present. Severe hyperkalemia (> 12 mEq/L [12 mmol/L]) during resuscitation typically indicates a fatal outcome and can guide decisions to terminate resuscitation efforts (2).
Treatment references
1. Musi ME, Sheets A, Zafren K, et al. Clinical staging of accidental hypothermia: The Revised Swiss System: Clinical staging of accidental hypothermia: The Revised Swiss System: Recommendation of the International Commission for Mountain Emergency Medicine (ICAR MedCom). Resuscitation. 162:182, 2021. doi: 10.1016/j.resuscitation.2021.02.038
2. Lott C, Truhlar A, Alfonzo A, et al. European Resuscitation Council Guidelines 2021: Cardiac arrest in special circumstances. Resuscitation. 2021. 161:152
Prognosis for Hypothermia
Patients who have been immersed in icy water for 1 hour or (rarely) longer have been successfully rewarmed without permanent brain damage (see Drowning: Prognosis), even when core temperatures were very low or pupils were unreactive. Outcome is difficult to predict and cannot be based on the Glasgow Coma Scale.
Grave prognostic markers include:
Evidence of cell lysis (serum potassium > 12 mEq/L [12 mmol/L])
Intravascular thrombosis (fibrinogen < 50 mg/dL [1.47 micromol/L])
A nonperfusing cardiac rhythm (ventricular fibrillation or asystole)
For a given degree and duration of hypothermia, children are more likely to recover than adults.
Key Points
Measure core temperature in the rectum or esophagus using an electronic thermometer or probe.
Above about 32° C, insulation with heated blankets and warm fluids to drink are adequate treatment.
Below about 32° C, active rewarming should be done, typically using forced-air hot air enclosures; heated, humidified oxygen; warm IV fluid; and sometimes heated lavage or extracorporeal methods (eg, cardiopulmonary bypass, hemodialysis).
At lower temperatures, patients are hypovolemic and require fluid resuscitation.
CPR is not done if there is a perfusing rhythm.
When CPR is done in patients with a nonperfusing rhythm, defibrillation is deferred (after 1 initial attempt) until temperature reaches about 30° C.
Advanced cardiac life-support medications are usually not given until temperature reaches about 30° C.







