





Extensive physiologic changes accompany the birth process, sometimes unmasking conditions that posed no problem during intrauterine life. For that reason, a clinician with neonatal resuscitation skills must attend each birth. Gestational age, prenatal history, and growth parameters help identify the risk of neonatal pathology.
About 10% of neonates require some respiratory assistance at birth. Fewer than 1% need extensive resuscitation. There are numerous causes of respiratory depression requiring resuscitation at birth (see table Risk Factors and Indications for Neonatal Resuscitation). The need for resuscitation rises significantly if birthweight is < 1500 g.
Risk Factors and Indications for Neonatal Resuscitation
Type of Factor | Risk Factor or Indication |
|---|---|
Neonatal respiratory distress/respiratory failure | |
Airway obstruction | Obstruction of the neonatal airway with blood, meconium , or mucus Anatomical anomalies of the airway (eg, agenesis, atresia, stenosis) |
Central nervous system abnormalities | |
Lung or chest disorder | Pulmonary hypoplasia |
Surfactant deficiency | |
Neonatal cardiovascular compromise | |
Ductal-dependent lesions causing hypoxia due to decreased pulmonary blood flow Mixing lesions causing hypoxia due to oxygenated blood mixing with deoxygenated blood (eg, truncus arteriosus) | |
Hypotension | Hypovolemia due to fetal or placental bleeding Neonatal sepsis |
Maternal factors | |
Antepartum disorders | Chronic or gestational diabetes Obesity Smoking Preterm delivery Oligohydramnios |
Placental disorders | Placental insufficiency |
Intrapartum disorders causing asphyxia | Breech presentation Cord compression Shoulder dystocia Uterine tetany Maternal and/or fetal hemorrhage Maternal hypotension Maternal hypoxemia |
Medications that cause fetal respiratory depression | Analgesics or hypnotics Anesthetics Magnesium sulfate Opioids |
Apgar Score
The Apgar score is used to describe a neonate's cardiorespiratory and neurologic condition at birth. The score is not a tool to guide resuscitation or subsequent treatment and does not determine the prognosis of an individual patient.
The Apgar score assigns 0 to 2 points for each of 5 measures of neonatal health (Appearance, Pulse, Grimace, Activity, Respiration—see table Apgar Score). Scores depend on physiologic maturity and birthweight, maternal perinatal therapy, and fetal cardiorespiratory and neurologic conditions. A score of 7 to 10 at 5 minutes is considered normal; 4 to 6, intermediate; and 0 to 3, low. Usually, scores are assigned only at 1 and 5 minutes of life. If scores are ≤ 5 at 5 minutes of life, scores should continue to be assigned every 5 minutes until the score is > 5.
There are multiple possible causes of low (0 to 3) Apgar scores, including severe, chronic problems that have a poor prognosis and acute problems that can be quickly resolved and have a good prognosis. A low Apgar score is a clinical finding and not a diagnosis.

Apgar Score
Score* | ||||
|---|---|---|---|---|
Criteria | Mnemonic | 0 | 1 | 2 |
Color | Appearance | All blue, pale | Pink body, blue extremities | All pink |
Heart rate | Pulse | Absent | < 100 beats/minute | > 100 beats/minute |
Reflex response to nasal catheter/tactile stimulation | Grimace | None | Grimace | Sneeze, cough |
Muscle tone | Activity | Limp | Some flexion of extremities | Active |
Respiration | Respiration | Absent | Irregular, slow | Good, crying |
* A total score of 7–10 at 5 minutes is considered normal; 4–6, intermediate; and 0–3, low. | ||||
Resuscitation
Neonatal resuscitation should follow the most recent recommendations of the American Academy of Pediatrics and the American Heart Association (1).
Preparation is essential. Identify perinatal risk factors, assign roles to team members, and prepare and check equipment:
At least 1 clinician skilled in the initial steps of neonatal resuscitation, including giving positive pressure ventilation (PPV), should be in attendance at every birth, and additional personnel with the ability to do a complete resuscitation should be rapidly available even in the absence of specific risk factors. A team of 4 or more members may be required for a complex resuscitation, and depending on the risk factors, it may be appropriate for the entire resuscitation team to be present prior to the birth.
Before a preterm delivery, set room temperature to 23 to 25° C (74 to 77° F).
A thermal mattress, hat, and plastic bag or wrap should be used for preterm infants < 32 weeks of gestation.
There are many perinatal risk factors that increase the likelihood of a need for resuscitation. In addition to those noted in table Risk Factors and Indications for Neonatal Resuscitation, some other risk factors include
Lack of prenatal care
Gestational age < 36 weeks or ≥ 41 weeks
Multiple gestation
Need for forceps, vacuum assist, or emergency cesarean delivery
Meconium-stained fluid
Shoulder dystocia, breech, or other abnormal presentation
Certain abnormal heart rate patterns in the fetus
Signs of infection in the neonate
Maternal risk factors (eg, fever, untreated or inadequately treated group B strep infection)
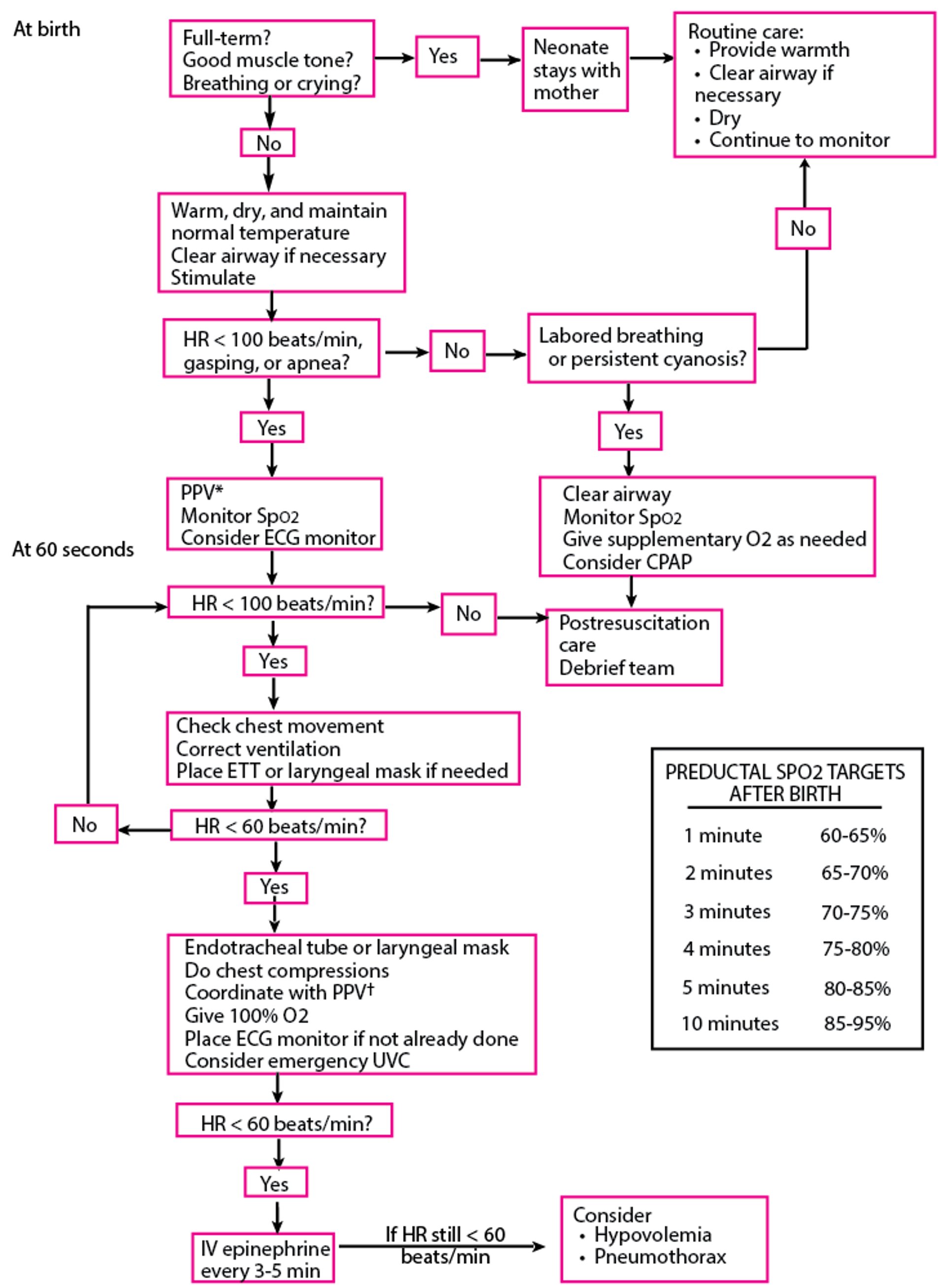
Algorithm for Resuscitation of Neonates
* PPV: Initiate resuscitation with room air (21% FiO2) for infants ≥ 35 weeks of gestational age or 21 to 30% FiO2 for infants < 35 weeks of gestational age. If SpO2 targets are not achieved, titrate inhaled oxygen concentration upward. † 3:1 compression:ventilation ratio with a total of 90 compressions and 30 breaths/minute. Compressions and ventilations are delivered sequentially, not simultaneously. Thus, give 3 compressions at a rate of 120/minute, followed by 1 ventilation over 1/2 second. CPAP = continuous positive airway pressure; ECG = electrocardiography; ETT = endotracheal tube; FiO2 = fractional inspired oxygen; HR = heart rate; PPV = positive pressure ventilation; SpO2 = oxygen saturation; UVC = umbilical venous catheter. Based on Weiner GM: Textbook of Neonatal Resuscitation, ed. 8. Itasca, American Academy of Pediatrics, 2021. |

Initial measures
Initial measures for all neonates include
Rapid assessment (within 60 seconds of birth) of breathing, heart rate, and color
Providing warmth to maintain a body temperature of 36.5 to 37.5° C
Drying
Stimulation of infant
Positioning to open airway
Suctioning if needed
Suctioning, including the use of a bulb syringe, is indicated only for infants who have obvious airway obstruction or who require positive pressure ventilation.
For the 90% of neonates who are vigorous and do not need resuscitation, establish skin-to-skin contact with the parent as soon as feasible.


The need for resuscitation is based primarily on the infant’s respiratory effort and heart rate. A 3-lead cardiac monitor is the preferred way to assess heart rate. In addition to clinical evaluation of respiration, monitor oxygen saturation using pulse oximetry with a preductal probe (ie, on the right wrist, hand, or finger), taking into account the expected slow rise in oxygen saturation over the first 10 minutes of life (see table Neonatal Oxygen Saturation Targets).
Neonatal Oxygen Saturation Targets
Time After Delivery | Preductal* SpO2 |
|---|---|
1 minute | 60–65% |
2 minutes | 65–70% |
3 minutes | 70–75% |
4 minutes | 75–80% |
5 minutes | 80–85% |
≥ 10 minutes | 85–95% |
* The right upper extremity receives preductal blood. | |
SpO2 = oxygen saturation. | |
Cord milking and delayed cord clamping
A 30- to 60-second delay in clamping the umbilical cord is recommended for preterm and term infants who do not need resuscitation. There is insufficient evidence to recommend delayed cord clamping in infants who do require resuscitation.
Recommendations for neonatal resuscitation include guidance on the appropriateness of cord milking or delayed cord clamping depending on neonatal factors (1, 2):
For vigorous term and late preterm neonates (34 to 36 6/7 weeks): Delayed cord clamping (≥ 30 seconds) can be beneficial compared with early cord clamping (< 30 seconds). Intact cord milking is not known to be beneficial compared with delayed cord clamping.
For nonvigorous term and late preterm neonates: Intact cord milking may be reasonable compared with early cord clamping (< 30 seconds).
For preterm neonates < 34 weeks who do not require resuscitation: Delayed cord clamping (≥ 30 seconds) can be beneficial compared with early cord clamping (< 30 seconds).
For preterm neonates between 28 and 34 weeks who do not require resuscitation and in whom delayed cord clamping cannot be performed, intact cord milking may be reasonable.
For preterm neonates < 28 weeks gestation: Intact cord milking is not recommended.
Ventilation and oxygenation
If the neonate’s respiratory effort is depressed, stimulation by flicking the soles of the feet and/or rubbing the back may be effective. Suctioning, unless indicated for airway obstruction, is not an effective method of stimulation and may cause a vagal response with apnea and bradycardia.
For infants with a heart rate of ≥ 100 beats/minute who have respiratory distress, labored breathing, and/or persistent cyanosis, supplemental oxygen and/or continuous positive airway pressure (CPAP) is indicated. Oxygen alone is indicated only if the infant's heart rate is > 100 beats/minute and if the infant shows no signs of respiratory distress but has persistent central cyanosis.
For infants with a heart rate of 60 to 100 beats/minute who have apnea, gasping, or ineffective respirations, positive pressure ventilation (PPV) using a T-piece resuscitator or a self-inflating bag with mask is indicated. A T-piece resuscitator is preferred over a self-inflating bag. However, because a T-piece resuscitator is powered by compressed gas, a self-inflating bag should be used instead if compressed gas is not available or fails. A supraglottic airway may also be used to provide ventilation in infants born at ≥ 34 0/7 weeks gestation (1).
Before giving PPV, the airway should be cleared by gently suctioning the mouth first and then the nose with a bulb syringe. The infant’s head and neck are supported in the neutral (sniffing) position, and the mouth is slightly opened with the jaw brought forward. Initial ventilator settings for a term infant are peak inspiratory pressure (PIP) of 20 to 25 cm H2O, positive end-expiratory pressure (PEEP) of 5 cm H2O, and an assist control (AC) or intermittent mandatory ventilation (IMV) rate of 40 to 60 breaths/minute. There are insufficient data to recommend a specific inspiratory time, but inflations of > 5 seconds are not recommended.
If the heart rate is < 60 beats/minute, neonates require compressions and PPV while awaiting endotracheal intubation.
The effectiveness of ventilation is judged mainly by rapid improvement in the heart rate. If the heart rate does not increase within 15 seconds, all of the following should be done until the heart rate is ≥ 100 beats/minute:
Adjust the mask to ensure a good seal.
Check the position of the head, mouth, and chin to ensure the airway is open. Placement of an oral airway may be considered if the mouth is not open despite good head position.
Suction the mouth and airway using a bulb syringe and/or a size 10 to 12 F catheter.
Assess chest wall rise.
If heart rate is still not increasing, the final step is to increase the airway pressure to ensure the chest wall rises adequately. Although the peak inspiratory pressure (PIP) should be set at the minimum level to which the infant responds, an initial PIP of 25 to 30 cm H2O, for the first few breaths, may be required to produce adequate ventilation in a term infant. Most of the time, preterm infants need lower pressures to obtain adequate ventilation. Because even brief periods of excessive tidal volume can easily damage neonatal lungs, particularly in preterm infants, it is important to frequently assess and adjust PIP during resuscitation. Devices that measure and control tidal volume during resuscitation have been described and may be helpful, but their role currently is not established.
Supplemental oxygen should be provided with a blender to allow the oxygen concentration to be varied in accord with the infant’s clinical condition. Positive pressure ventilation should be initiated with 21% fractional inspired oxygen (FiO2) (room air) for term infants or 21 to 30% FiO2 for preterm infants ≤ 35 weeks and titrated as indicated by pulse oximetry. An infant who requires compressions or intubation or who does not respond to PPV by demonstrating an increase in heart rate should be given 100% FiO2. Hyperoxia (O2 saturation > 95%) should be avoided. Infants who have otherwise responded well to resuscitation but who are persistently cyanotic without evidence of lung disease may have congenital heart disease.
Intubation and chest compression
If the infant does not respond to PPV delivered by mask or the heart rate is < 60 beats/minute, compressions should be initiated and the infant should undergo endotracheal intubation. Immediate endotracheal intubation is indicated if PPV is required for an infant with a prenatally diagnosed or clinically suspected diaphragmatic hernia. PPV with a bag and mask should be avoided in this circumstance so as not to inflate the bowel and further compromise the lungs. If intubation is necessary, a cardiac monitor is recommended as the most accurate way to assess the infant's heart rate.
The size of the tube and depth of intubation are selected according to the infant's weight and gestational age (see table Endotracheal Intubation in Neonates).
Endotracheal Intubation in Neonates
Weight at Time of Intubation (kg) | Weeks of Gestational Age | Insertion Depth at Lips (cm) | Endotracheal Tube Size (diameter, mm) |
|---|---|---|---|
0.5–0.6 | 23–24 | 5.5 | Size 2.5: For infants < 1 kg or < 28 weeks of gestational age |
0.7–0.8 | 25–26 | 6.0 | |
0.9–1.0 | 27–29 | 6.5 | Size 3.0: For infants 1 to 2 kg or 28 to 34 weeks of gestational age |
1.1–1.4 | 30–32 | 7.0 | |
1.5–1.8 | 33–34 | 7.5 | Size 3.5: For infants > 2 kg or > 34 weeks of gestational age |
1.9–2.4 | 35–37 | 8.0 | |
2.5–3.1 | 38–40 | 8.5 | |
3.2–4.2 | 41–43 | 9.0 | Size 3.5 to 4.0 |
Data from Kempley ST, Moreiras JW, Petrone FL: Endotracheal tube length for neonatal intubation. Resuscitation 77(3):369-373, 2008. doi: 10.1016/j.resuscitation.2008.02.002 and from Weiner GM, ed: Textbook of Neonatal Resuscitation, ed. 8. Itasca, American Academy of Pediatrics, 2021. | |||
The nasal-tragus length (distance from the base of the nasal septum to the tragus) plus 1 cm has been studied as an alternative to gestational age and weight for determining endotracheal tube placement depth. Results of these studies vary, and more research is needed (3, 4).
Many endotracheal tubes have insertion markings to be positioned at the level of the vocal cords to guide the initial placement.
Immediately after intubation, clinicians should listen for bilaterally equal breath sounds. Selective intubation of the right mainstem bronchus with decreased breath sounds on the left is common if the tube is inserted too deeply.
Tracheal intubation should be confirmed by testing for exhaled CO2 using a colorimetric detector. A positive test, in which the colorimetric indicator turns from purple/blue to yellow, confirms tracheal intubation. A negative test is most commonly due to esophageal intubation but may occur when ventilation is insufficient or there is very poor cardiac output. A fixed yellow color can be due to direct contamination by epinephrine or may indicate the device is defective.
Proper endotracheal tube depth should result in the tip of the tube being about halfway between the clavicles and the carina on chest radiograph, coinciding roughly with vertebral level T1-T2.
For infants ≥ 34 0/7 weeks (or ≥ 2000 g), a supraglottic airway may be used if there is difficulty intubating the infant. Infants of any gestational age can be sustained with appropriate bag-and-mask or T-piece resuscitator PPV if team members are unable to place an endotracheal tube. In these infants, a nasogastric tube should be placed to allow for decompression of the stomach.
After intubation, if the heart rate does not improve and there is insufficient chest rise with adequate peak inspiratory pressure, the airway may be obstructed and suctioning should be done. Thinner-diameter catheters (5 to 8 F) may clear an endotracheal tube of thin secretions but are ineffective for thick secretions, blood, or meconium. In such cases, the endotracheal tube can be removed while applying continuous suction with a meconium aspirator and sometimes the trachea can be directly suctioned with a larger (10 to 12 F) catheter. After suctioning the trachea, the infant is reintubated.
If the infant is adequately ventilated and the heart rate remains < 60 beats/minute, chest compressions should be given using the 2-thumb/chest encircling technique in a coordinated ratio of 3 compressions to 1 ventilation with 90 compressions and 30 ventilations per minute. The 2-finger technique of chest compression is not recommended. Intubation, if not already done, is always indicated when initiating chest compression, and the oxygen concentration should be increased to 100%. The heart rate should be reassessed after 60 seconds of chest compressions.
If severe bradycardia persists while the infant is adequately ventilated and chest compressions have been given for 1 minute, the umbilical vein should be catheterized or an intraosseous (IO) needle should be placed to give intravascular epinephrine as soon as possible. The dose can be repeated every 3 to 5 minutes as needed. While access is being established, a dose of If severe bradycardia persists while the infant is adequately ventilated and chest compressions have been given for 1 minute, the umbilical vein should be catheterized or an intraosseous (IO) needle should be placed to give intravascular epinephrine as soon as possible. The dose can be repeated every 3 to 5 minutes as needed. While access is being established, a dose ofepinephrine may be given via the endotracheal tube, but the efficacy of this route is unknown. The dose of epinephrine given endotracheally is different from the dose given IV/IO.
Failure to respond to resuscitation
If the infant does not respond to resuscitation and has pallor and/or poor perfusion, IV volume expansion is recommended. Crystalloid or colloid boluses should be given over longer periods in preterm infants because of the risk of intraventricular hemorrhage. Uncross-matched, O-negative packed red blood cells also may be used for volume expansion, especially if there has been acute, severe blood loss.
Medications such as sodium bicarbonate and atropine are not recommended in the course of resuscitation. Naloxone is not recommended in the initial steps of the management of respiratory depression, and one review found insufficient evidence to determine the safety and efficacy of this medication in neonates (5).
If the infant does not respond to resuscitation or suddenly deteriorates after an initial response, pneumothorax must be ruled out. Although pneumothorax may be clinically suspected by finding unilateral diminished breath sounds on auscultation, breath sounds are well-transmitted across the precordium and the presence of bilateral breath sounds can be misleading. Transillumination of the chest may be used but is often limited by the lack of an immediately available intense light source and the inability to sufficiently darken the room. Additionally, a pneumothorax may be misdiagnosed in small infants with thin skin and little subcutaneous fat or missed in large infants with thick skin and subcutaneous fat. A chest radiograph typically takes too much time to be of practical benefit during resuscitation, but bedside ultrasound offers the possibility of an accurate and rapid diagnosis if quickly available. Because pneumothorax is a reversible cause of unresponsiveness to resuscitation, bilateral thoracentesis should be considered on empirical grounds even in the absence of a definite diagnosis.
In some cases, thoracentesis is diagnostic and therapeutic for an unsuspected pleural effusion.
No resuscitation
The decision of whether to resuscitate requires discussions with the family so they understand the complexity of their infant's diagnoses and status and so the medical team understands the family's wishes. It is preferable for these discussions to occur before there is an emergent need for resuscitation. Some examples of this type of clinical situation include the following:
Infants with known lethal anomalies diagnosed before birth: Ideally, discussion with the family should be done well before delivery to arrive at a plan.
Extremely preterm infants: Institutional guidelines should be followed, bearing in mind that prenatal gestational age estimates are often not precise.
In infants with unsuspected severe anomalies discovered at delivery, an initial diagnosis and/or prognosis may be inaccurate, so resuscitation should typically be attempted.
When possible, a neonatologist should be involved in threshold of viability decisions. Obstetric dating data should be obtained directly from the pregnant patient as well as from medical records. The neonatologist should use this information to calculate the estimated date of delivery and possible range of gestational age rather than relying on the previously set estimated date of delivery. Discussion with parents should take into account current local and national outcomes data based on expected gestational age and birthweight (if known), fetal sex, singleton/multifetal gestation status, and antenatal treatment with corticosteroids. In cases in which there is a range of acceptable approaches, the parents’ input is the most important factor in determining whether to attempt resuscitation.
The goal of resuscitation for most families and physicians is the survival of the infant without severe morbidity. An infant who is born without any detectable vital signs and does not recover any sign of life in spite of appropriate resuscitation for about 20 minutes is unlikely to achieve this goal, and discontinuation of resuscitation under such circumstances is considered reasonable according to guidelines in the Textbook of Neonatal Resuscitation (6). However, there are no firm guidelines as to how long resuscitation should be continued when there is persistent severe bradycardia, or on what to do when the heart rate increases after resuscitation has been stopped. In such cases, the appropriateness of intervention should be evaluated in light of the goals of treatment.
References
1. Yamada NK, Szyld E, Strand ML, et al. 2023 American Heart Association and American Academy of Pediatrics Focused Update on Neonatal Resuscitation: An Update to the American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2024;149(1):e157-e166. doi:10.1161/CIR.0000000000001181
2. American College of Obstetricians and Gynecologists’ Committee on Obstetric Practice. Delayed Umbilical Cord Clamping After Birth: ACOG Committee Opinion, Number 814. Obstet Gynecol. 2020;136(6):e100-e106. doi:10.1097/AOG.0000000000004167
3. Uygur Ö, Öncel MY, Şimşek GK, et al. Is Nasal Septum-Tragus Length Measurement Appropriate for Endotracheal Tube Intubation Depth in Neonates? A Randomized Controlled Study. Am J Perinatol. 2021;38(7):728-733. doi:10.1055/s-0039-3400982
4. Gray MM, Delaney H, Umoren R, et al. Accuracy of the nasal-tragus length measurement for correct endotracheal tube placement in a cohort of neonatal resuscitation simulators. J Perinatol. 2017;37(8):975-978. doi:10.1038/jp.2017.63
5. Moe-Byrne T, Brown JVE, McGuire W. Naloxone for opioid-exposed newborn infants. Cochrane Database Syst Rev. 2018;10(10):CD003483. Published 2018 Oct 12. doi:10.1002/14651858.CD003483.pub3
6. Weiner GM, ed: Textbook of Neonatal Resuscitation, ed. 8. Itasca, American Academy of Pediatrics, 2021.







