




Gynecologic diagnostic tests and procedures help identify vaginal infections (eg, trichomoniasis, bacterial vaginosis, yeast infection) and cancer and provide information on menstrual cycle and hormone levels.
Pregnancy Testing
Women who are of reproductive age may be tested for pregnancy if they are trying to become pregnant, are concerned about an unintended pregnancy, or have gynecologic symptoms.
Urine pregnancy tests also measure beta-hCG, but they are less sensitive than serum tests. Urine tests typically detect beta-hCG levels of 12 to 50 mIU/mL (1). Also, the hCG concentration is lower in urine than in serum. Urine tests are typically positive at about 1 week after the first day of the missed menstrual period. On the first day after the missed period, approximately half of pregnant women will have a negative test result.
Home urine pregnancy test sensitivity and specificity can be variable depending upon the specific test kit, user's technique, and interpretation. Thus, any positive home pregnancy test should be confirmed by either a laboratory urine or serum pregnancy test.
Pregnancy testing reference
1. Cole LA: The hCG assay or pregnancy test. Clin Chem Lab Med. 2012;50(4):617-630. doi:10.1515/CCLM.2011.808
Testing for Infection
Testing for vaginitis
Tests to evaluate for vaginitis include
Vaginal pH: Tested with pH paper (normal vaginal pH is 3.8 to 4.2; increased [more alkaline] pH is found in bacterial vaginosis and trichomoniasis)
Saline wet mount:
Potassium hydroxide (KOH) wet mount: Prepared with 10% potassium hydroxide; findings can indicate bacterial vaginosis (positive whiff test) or candidiasis (hyphae)
Nucleic acid amplification testing (NAAT): Available for bacterial vaginosis, candidiasis, and trichomoniasis
Testing for sexually transmitted infections
Tests for sexually transmitted infections of the female genital tract include the following (see CDC: Screening Recommendations and Considerations Referenced in Treatment Guidelines and Original Sources):
NAAT of a sample from the cervix, vagina, or urethra or a urine sample to test for certain local organisms (Trichomonas, Neisseria gonorrhoeae, Chlamydia trachomatis); sometimes, Gram stain and culture used for genital fluid samples
Polymerase chain reaction (PCR), viral culture, or direct fluorescent antibody testing of a swab of lesions to test for genital herpes simplex virus infection
Blood tests for systemic infections (HIV, hepatitis B or C, or syphilis)
Cervical Cancer Testing
Cervical cancer screening
Routine cervical cancer screening effectively detects preinvasive and early-stage disease and decreases cervical cancer incidence and mortality rates.
Two types of screening tests for cervical abnormalities are used:
Tests for high-risk human papillomavirus (HPV) genotypes
Pap test (cervical cytology)
Recommendations vary regarding the choice of screening test, frequency, and age to begin and discontinue screening (see table Cervical Cancer Screening). The American College of Obstetricians and Gynecologists (ACOG) follows the recommendations of the United States Preventive Services Task Force (USPSTF) (1, 2):
21 years: Begin cervical cancer screening
21 to 29 years: Cervical cytology every 3 years (alternatively, average-risk patients ≥ 25 years may begin screening with primary HPV testing alone every 5 years)
≥ 30 to 65 years: Cervical cytology alone every 3 years; or HPV test alone every 5 years; or cytology and HPV co-testing every 5 years
> 65 years: Discontinue screening if patient has adequate negative screening for the prior 10 years; for women without documentation of prior screening, continued screening until criteria for stopping are met
For women with certain indications (eg, women who have HIV infection, are immunosuppressed, have previous abnormal cervical cancer screening results), more frequent screening may be required.
If patients have had a total hysterectomy (cervix and uterus removed) and have no history of cervical cancer or high-grade cervical intraepithelial neoplasia, further cervical cancer screening is not indicated.
Abnormal results of cervical cancer screening tests require further evaluation, as appropriate.
Cervical diagnostic and treatment procedures
Diagnostic or treatment procedures of the cervix are performed if there are abnormal findings on pelvic examination, cervical cytology, or HPV testing. A cervical biopsy is also done if there is a grossly visible cervical lesion and the diagnosis is uncertain on examination.
Diagnostic procedures include
Colposcopy: Examination of the vagina and cervix with a magnifying lens (eg, to identify areas that require biopsy)
Cervical biopsy: Biopsy of cervix, usually taking a 1 to 2 mm specimen
Endocervical curettage: Insertion of a curet to obtain tissue from inside the cervical canal
Cervical conization (cone biopsy) procedures can be used for diagnosis and/or treatment. These procedures remove a conical wedge of cervical tissue using different techniques including
Loop electrical excision procedure (LEEP): Performed with a thin wire loop that conducts an electrical current
Cold knife conization: Performed with a scalpel
Laser conization: Performed with laser
Procedures used only for treatment include
Cervical ablation: Techniques include cryotherapy, carbon dioxide therapy, thermal ablation, or diathermy
Cervical testing references
1. American College of Obstetricians and Gynecologists: Updated cervical cancer screening guidelines. Published October 2016. Reaffirmed April 2023.
2. US Preventive Services Task Force: Screening for Cervical Cancer: US Preventive Services Task Force recommendation statement. JAMA 320 (7):674–686, 2018. doi:10.1001/jama.2018.10897
Other Gynecologic Biopsies
In addition to cervical biopsy, biopsy may be indicated for other parts of the lower genital tract.
Vulvar biopsy
Vulvar biopsies are indicated for patients with
Symptoms or examination findings suggestive of vulvar intraepithelial neoplasia, vulvar malignancy (eg, squamous cell carcinoma, melanoma), or vulvar dermatoses (eg, lichen sclerosus, lichen planus)
Any visible vulvar lesion for which a definitive diagnosis cannot be made on physical examination
Lesions that did not respond fully to or recurred after medical treatment
Lesions with an abnormal vascular pattern
Lesions requiring definitive treatment by excisional procedures
Relative contraindications to vulvar biopsy include bleeding diathesis and current anticoagulant therapy.
Vaginal biopsy
Vaginal biopsies are not commonly performed and are indicated when there is a concern for vaginal intraepithelial neoplasia or vaginal malignancy or when there are abnormal lesions that require pathology evaluation for diagnosis.
Relative contraindications to vaginal biopsy include bleeding diathesis and current anticoagulant therapy.
Endometrial biopsy
Endometrial sampling may be done as an office endometrial biopsy procedure or as an operative procedure (dilation and curettage with or without hysteroscopy).
Indications for endometrial biopsy include (1)
Postmenopausal uterine bleeding
Abnormal uterine bleeding (AUB) in patients who are ≥ 45 years or < 45 years with endometrial cancer risk factors (eg, obesity, history of unopposed estrogen exposure), failed medical management, or persistent AUB
Follow-up monitoring for endometrial hyperplasia
Cervical cytology with glandular cells associated with an increased risk of endometrial cancer: benign-appearing endometrial cells in patients ≥ 45 years; atypical glandular cells [AGC]-endometrial; AGC or adenocarcinoma in-situ (AIS) in patients ≥ 35 or in those < 35 with endometrial cancer risk factors or symptoms; or persistent abnormal cervical cytology results in patients with any AGC category (2)
Screening in patients at high risk for endometrial cancer (eg, Lynch syndrome)
The only absolute contraindication for endometrial biopsy is a desired intrauterine pregnancy. Relative contraindications are
Bleeding diathesis or current anticoagulant therapy
Acute infection of the vagina, cervix, uterus, or fallopian tubes
Cervical stenosis
Congenital female reproductive tract anomalies
3). Anesthesia is not required, but some clinicians advise patients to take preprocedure nonsteroidal anti-inflammatory drugs or offer patients a topical cervical anesthetic spray or paracervical block (4). Antibiotic prophylaxis is not required.
During the procedure, a thin (< 3 mm), flexible, disposable, plastic, low-pressure suction curette is inserted through the cervix to the level of the uterine fundus; mechanical dilation is not usually required. Usually, tenaculum is placed on the anterior cervix to stabilize the uterus. Suction is applied by withdrawing an internal plunger. To obtain an adequate sample of the endometrial cavity, the clinician turns the device 360° and moves it 3 times in a cephalic to caudal motion. Alternatively, for postmenopausal women, endometrial sampling with a brush device is more likely than a suction device to yield an adequate sample (5).
The most common adverse effects are uterine cramping or vasovagal reactions. Uterine perforation is a rare but more serious potential complication.
Other gynecologic biopsies references
1. Committee on Practice Bulletins—Gynecology. Practice bulletin no. 128: diagnosis of abnormal uterine bleeding in reproductive-aged women. Obstet Gynecol. 2012;120(1):197-206. doi:10.1097/AOG.0b013e318262e320
2. Perkins RB, Guido RS, Castle PE, et al. 2019 ASCCP Risk-Based Management Consensus Guidelines for Abnormal Cervical Cancer Screening Tests and Cancer Precursors [published correction appears in J Low Genit Tract Dis. 2020 Oct;24(4):427]. J Low Genit Tract Dis. 2020;24(2):102-131. doi:10.1097/LGT.0000000000000525
3. Al-Fozan H, Firwana B, Al Kadri H, Hassan S, Tulandi T. Preoperative ripening of the cervix before operative hysteroscopy. Cochrane Database Syst Rev. 2015;(4):CD005998. Published 2015 Apr 23. doi:10.1002/14651858.CD005998.pub2
4. Charoenkwan K, Nantasupha C. Methods of pain control during endometrial biopsy: A systematic review and meta-analysis of randomized controlled trials. J Obstet Gynaecol Res. 2020;46(1):9-30. doi:10.1111/jog.14152
5. Williams AR, Brechin S, Porter AJ, et al: Factors affecting adequacy of Pipelle and Tao Brush endometrial sampling. BJOG. 2008;115(8):1028-1036. doi:10.1111/j.1471-0528.2008.01773.x
Imaging Studies
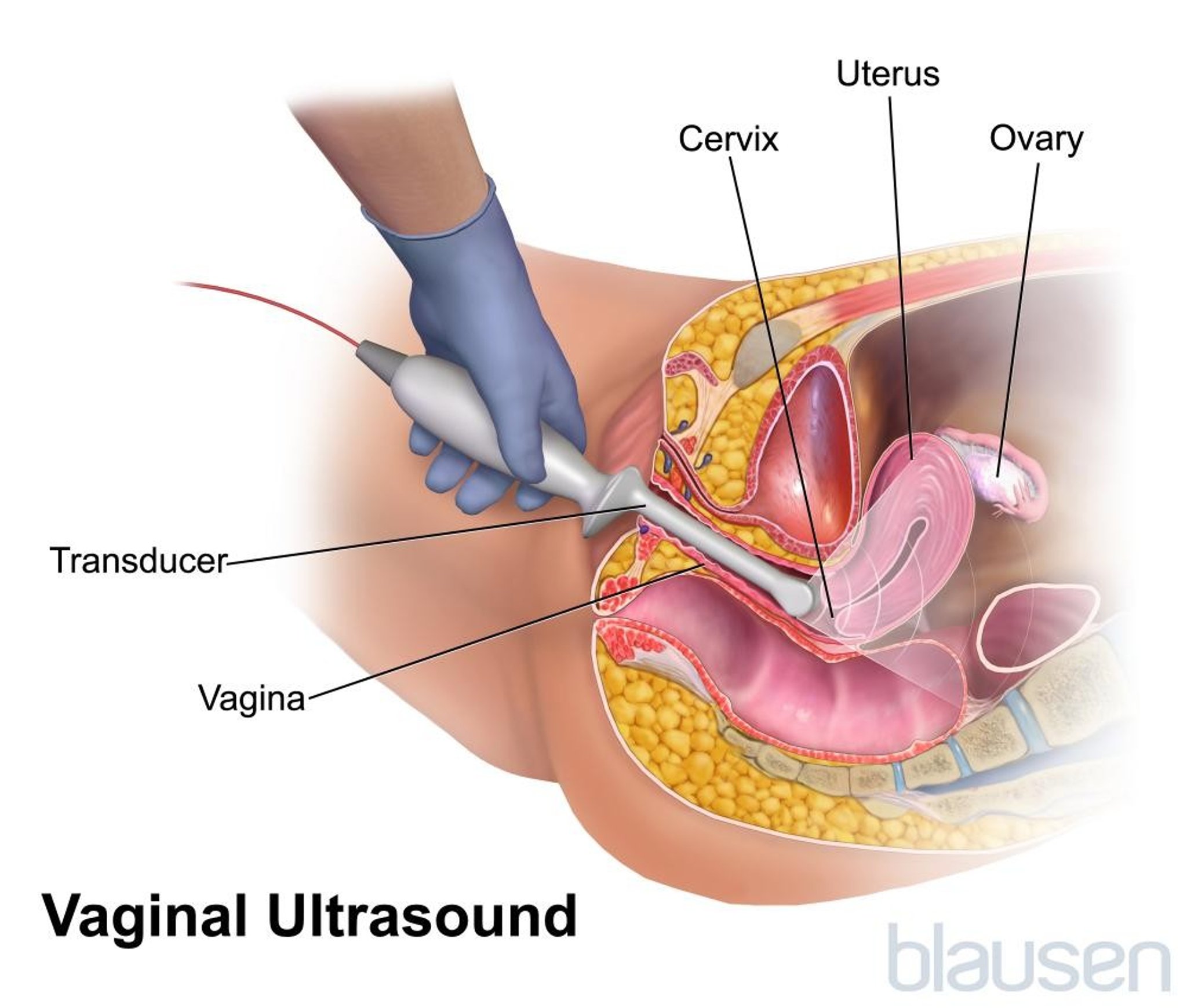
Pelvic ultrasonography done by trained radiologists or gynecologists using transvaginal, transabdominal, and sometimes transrectal probes is the most common imaging study to evaluate female reproductive tract abnormalities. Other imaging studies, such as the following, may be done for specific indications:
MRI or CT: If evaluation with ultrasonography is not adequate, MRI (which is highly specific for pelvic organ pathology but expensive) may be used. CT is usually less desirable because it is somewhat less accurate for gynecologic pathology, involves significant radiation exposure, and often requires a radiopaque agent. CT is mainly used for evaluation for metastases in gynecologic malignancies.
Sonohysterography (saline infusion sonography): Isotonic fluid is injected through the cervix into the uterus during ultrasonography. The fluid distends the uterine cavity, making it easier to detect intrauterine masses (eg, endometrial polyps, submucosal leiomyomas).
Hysterosalpingography: Fluoroscopic imaging of the uterus and fallopian tubes is done after injection of a radiopaque agent into the uterine cavity. Hysterosalpingography is usually done to check tubal patency in infertile patients, but this imaging study may also detect intrauterine lesions.

Diagnostic Procedures
Diagnostic procedures are indicated if a diagnosis is not identified by medical history, physical examination, and office procedures. These procedures may also be used for treatment.
Dilation and curettage
Dilation and curettage (D&C) involves dilation of the cervix and insertion of a curet to remove endometrial tissue, usually when endometrial hyperplasia or cancer is suspected. D&C is sometimes performed as a therapeutic procedure for abnormal uterine bleeding.
Hysteroscopy
Hysteroscopy can be performed concurrently with D&C if visualization of the uterine cavity is required. After cervical dilation, a camera (hysteroscope) is inserted through the cervix into the uterine cavity. The cavity is inspected for abnormalities. Focal biopsies or myomectomy may then be done by passing instruments through a channel in the hysteroscope.
Laparoscopy
Laparoscopy is a transabdominal procedure during which small abdominal incisions are made. A camera (laparoscope) is inserted for inspection of the abdominal cavity or for surgical procedures. Diagnostic laparoscopy is performed when abnormalities cannot be adequately detected or evaluated with imaging studies (eg, endometriosis, complex ovarian cysts).
Culdocentesis
Culdocentesis, now rarely used, is needle puncture of the posterior vaginal fornix to obtain fluid from the cul-de-sac (which is posterior to the uterus) for culture and for tests to detect blood from a ruptured ectopic pregnancy or ovarian cyst.







