


Reentrant supraventricular tachycardias (SVT) involve reentrant pathways with a component above the bifurcation of the His bundle. Patients have sudden episodes of palpitations that begin and terminate abruptly; some have dyspnea or chest discomfort. Diagnosis is clinical and by electrocardiography. Initial treatment is usually with vagotonic maneuvers. If these maneuvers are ineffective, treatment is with IV adenosine or nondihydropyridine calcium channel blockers for narrow QRS rhythms or for wide QRS rhythms known to be a reentrant SVT with aberrant conduction that requires atrioventricular nodal conduction. Procainamide or amiodarone are effective for other wide QRS rhythms. Synchronized cardioversion can be done for all cases in which drugs are ineffective or there is hemodynamic instability.
(See also Overview of Arrhythmias.)
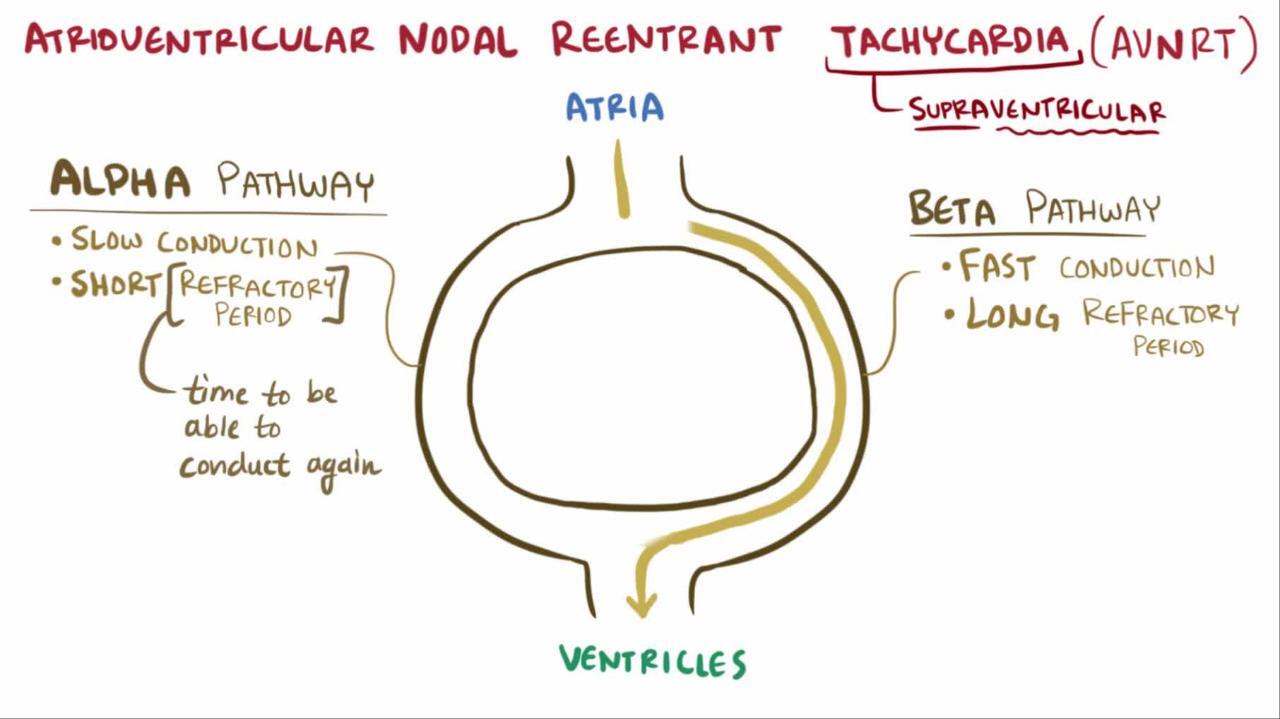
Pathophysiology of Reentrant SVTs
The reentry pathway (see figure Mechanism of typical reentry) in supraventricular tachycardia may be
Within the atrioventricular (AV) node (about 50%)
An accessory bypass tract (40%) OR
Confined to the atria or sinoatrial (SA) node (10%)
AV nodal reentrant tachycardia occurs most often in otherwise healthy patients. It is most commonly triggered by an atrial premature beat.
Accessory pathway reentrant tachycardia involves tracts of conducting tissue that partially or totally bypass normal AV connections (bypass tracts). They run most commonly from the atria directly to the ventricles and less commonly from the atrium to a portion of the conduction system or from a portion of the conduction system to the ventricle. They can be triggered by atrial premature beats or ventricular premature beats.
Синдром Вольфа-Паркінсона-Уайта (WPW)
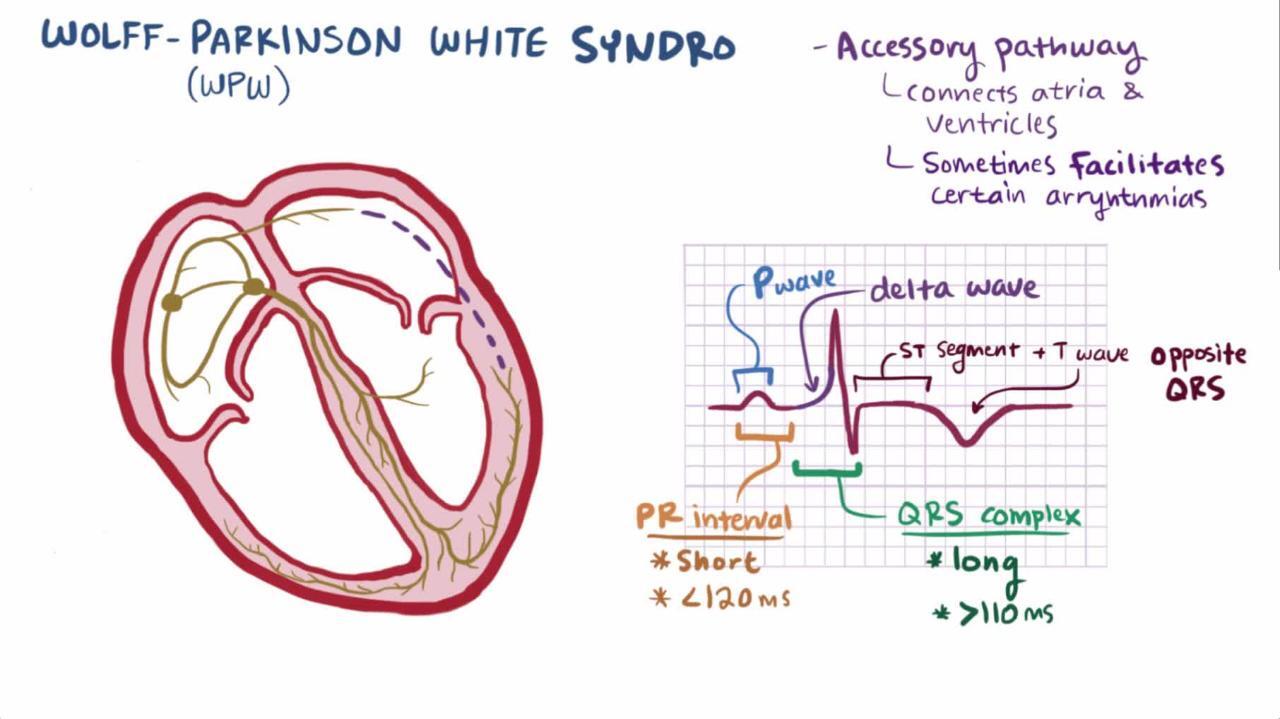
WPW (preexcitation) syndrome is the most common accessory pathway SVT, occurring in about 1 to 3/1000 people. WPW syndrome is mainly idiopathic, although it is more common among patients with hypertrophic cardiomyopathy or other forms of cardiomyopathy, transposition of the great vessels, or Epstein anomaly. There are two main forms of WPW syndrome:
Classic
Concealed
In classic (or manifest) WPW syndrome, antegrade conduction occurs over both the accessory pathway and the normal conducting system during sinus rhythm. The accessory pathway, being faster, depolarizes some of the ventricle early, resulting in a short PR interval and a slurred upstroke to the QRS complex (delta wave—see figure Classic Wolff-Parkinson-White syndrome).
Класичний синдром Вольфа-Паркінсона-Уайта (WPW)
Leads I, II, III, V3 through V6 show classic features of WPW syndrome, with a short PR interval and a delta wave during sinus rhythm. |


The delta wave prolongs QRS duration to > 0.12 second, although the overall configuration, apart from the delta wave, may appear normal. Depending on the orientation of the delta wave, a pseudoinfarction pattern Q-wave may be present. Because the early depolarized parts of the ventricle also repolarize early, the T-wave vector may be abnormal.
In concealed WPW syndrome, the accessory pathway does not conduct in an antegrade direction; consequently, the above electrocardiographic (ECG) abnormalities do not appear. However, it conducts in a retrograde direction and thus can participate in reentrant tachycardia.
In the most common form of reentrant tachycardia (called orthodromic reciprocating tachycardia), the circuit uses the normal atrioventricular (AV) conduction pathway to activate the ventricles, returning to the atrium via the accessory AV connection. The resultant QRS complex is thus narrow (unless bundle branch block coexists) and without a delta wave. Orthodromic reciprocating tachycardia is typically a short RP tachycardia with the retrograde P wave in the ST segment.
Rarely, the reentrant circuit revolves in the opposite direction, from the atrium to the ventricle via the accessory AV connection, and returning from the ventricle in the retrograde direction up the normal AV conduction system (called antidromic reciprocating tachycardia). The QRS complex is wide because the ventricles are activated abnormally. In patients with 2 accessory AV connections (not uncommon), a reciprocating tachycardia using one accessory connection in the antegrade direction and the other in the retrograde direction may occur.
Tachycardias in WPW syndrome may begin as or degenerate into atrial fibrillation (AF), which can be very dangerous if there is antegrade conduction over the accessory pathway (manifest WPW). In this case, the normal rate-limiting effects of the atrioventricular (AV) node are bypassed, and the resultant excessive ventricular rates (sometimes 200 to 300 beats/minutes) may lead to ventricular fibrillation.
Symptoms and Signs of Reentrant SVTs
Most patients present during young adulthood or middle age. They typically have episodes of sudden-onset, sudden-offset, rapid, regular palpitations often associated with symptoms of hemodynamic compromise (eg, dyspnea, chest discomfort, light-headedness). Attacks may last only a few seconds or persist for several hours (rarely, > 12 hours).
Infants present with episodic breathlessness, lethargy, feeding problems, or rapid precordial pulsations. If the episode of tachycardia is protracted, infants may present with heart failure.
Examination is usually unremarkable except for a heart rate of 160 to 240 beats/minute.
Diagnosis of Reentrant SVTs
Electrocardiography (ECG)
Diagnosis of supraventricular tachycardia is by ECG showing rapid, regular tachycardia. Previous tracings, if available, are reviewed for ECG signs of manifest WPW syndrome.
P waves vary. In most cases of AV node reentry, retrograde P waves are in the terminal portion of the QRS complex (often producing a pseudo-R′ deflection in lead V1); about one third occur just after the QRS complex, and very few occur before. P waves always follow the QRS complex in orthodromic reciprocating tachycardia of WPW syndrome.
QRS complex is narrow except with coexisting bundle branch block, antidromic tachycardia, or dual accessory connection reciprocating tachycardia. Wide-complex tachycardia must be distinguished from ventricular tachycardia (see table Indications for Implantable Cardioverter-Defibrillators and figures Classic Wolff-Parkinson-White syndrome and Narrow QRS tachycardia).
Цінні поради та підводні камені
|
Тахікардія з вузькими комплексами QRS: ортодромна реципрокна тахікардія з використанням додаткового шляху при синдромі Вольфа-Паркінсона-Уайта
Activation is as follows: atrioventricular node, His-Purkinje system, ventricle, accessory pathway, atria. The P wave closely follows the QRS complex; it is a short RP interval tachycardia (PR > RP). |


Treatment of Reentrant SVTs
Vagotonic maneuvers
Adenosine
Verapamil or diltiazem if narrow, regular QRS complex
For frequent recurrence, ablation
Many episodes stop spontaneously before treatment.
Vagotonic maneuvers (eg, Valsalva maneuver, unilateral carotid sinus massage, ice water facial immersion, swallowing of ice-cold water), particularly if used early, may terminate the tachyarrhythmia; some patients use these maneuvers at home.
AV node blockers are used if vagotonic maneuvers are ineffective and the QRS complex is narrow (indicating orthodromic conduction) and regular (indicating the episode is not atrial fibrillation); blocking conduction through the AV node for one beat interrupts the reentrant cycle. Adenosine is the first choice. Dose is 6 mg by rapid IV bolus (0.05 to 0.1 mg/kg in children), followed by a 20-mL saline bolus. If this dosage is ineffective, 2 subsequent 12-mg doses are given every 5 minutes. Adenosine sometimes causes a brief (2- to 3-second) period of cardiac standstill, which may distress patient and physician. Verapamil 5 mg IV or diltiazem 0.25 to 0.35 mg/kg IV are alternatives.
For a regular, wide QRS complex tachycardia known to be an antidromic reciprocating tachycardia not involving double accessory pathways (which must be identified by the history; they cannot be established acutely), AV nodal blockers may also be effective. However, if the mechanism of the tachycardia is unknown and ventricular tachycardia has not been excluded, AV nodal blockers should be avoided because they may worsen ventricular tachycardias. In such cases (or those in which drugs are ineffective), IV procainamide or amiodarone can be used. Alternatively, synchronized cardioversion with 50 joules (0.5 to 2 joules/kg for children) is quick and safe and may be preferred to these more toxic drugs.
When episodes of AV nodal reentrant tachycardia are frequent or bothersome, options include long-term antiarrhythmics or transvenous catheter ablation. Generally, ablation is recommended, but if it is not acceptable, drug prophylaxis usually begins with digoxin and proceeds, as required, to beta-blockers, nondihydropyridine calcium channel blockers, or both, then to one or more class Ia, class Ic, or class III antiarrhythmics (see table Antiarrhythmic Drugs). However, postadolescent patients with manifest Wolff-Parkinson-White syndrome (in whom atrial fibrillation becomes more likely) should not receive digoxin or a nondihydropyridine calcium channel blocker alone (see also Atrial Fibrillation and Wolff-Parkinson-White Syndrome).
Ключові моменти
Symptoms of reentrant supraventricular tachycardias begin and end suddenly.
Wolff-Parkinson-White (preexcitation) syndrome is the most common accessory pathway SVT.
QRS complexes are typically narrow, rapid, and regular; however, wide complexes may occur and must be differentiated from ventricular tachycardia.
Vagotonic maneuvers (eg, Valsalva maneuver) sometimes help.
Use atrioventricular (AV) nodal blockers for narrow complex tachycardia; adenosine is the first choice, and if ineffective, verapamil or diltiazem are alternatives.
Avoid AV nodal blockers for wide complex tachycardia; use synchronized cardioversion or procainamide or amiodarone.
