


Jaundice is a yellow discoloration of the skin and eyes caused by hyperbilirubinemia (elevated serum bilirubin concentration). The serum bilirubin level required to cause jaundice varies with skin tone and body region, but jaundice usually becomes visible on the sclera at a level of 2 to 3 mg/dL (34 to 51 micromol/L) and on the face at about 4 to 5 mg/dL (68 to 86 micromol/L). With increasing bilirubin levels, jaundice seems to advance in a head-to-foot direction, appearing at the umbilicus at about 15 mg/dL (257 micromol/L) and at the feet at about 20 mg/dL (342 micromol/L). Slightly more than half of all neonates become visibly jaundiced in the first week of life. Almost all hyperbilirubinemia in the immediate neonatal period is unconjugated, which is termed indirect bilirubin, based on older laboratory measurement methods; conjugated bilirubin is termed direct bilirubin. For further discussions of cholestasis and disorders of bilirubin excretion in the neonatal period see neonatal cholestasis.
Consequences of hyperbilirubinemia
Hyperbilirubinemia may be harmless or harmful depending on its cause and the degree of elevation. Some causes of jaundice are intrinsically dangerous whatever the bilirubin level. But hyperbilirubinemia of any etiology is a concern once the level is high enough. The threshold for concern varies by
Age
Degree of prematurity
Health status
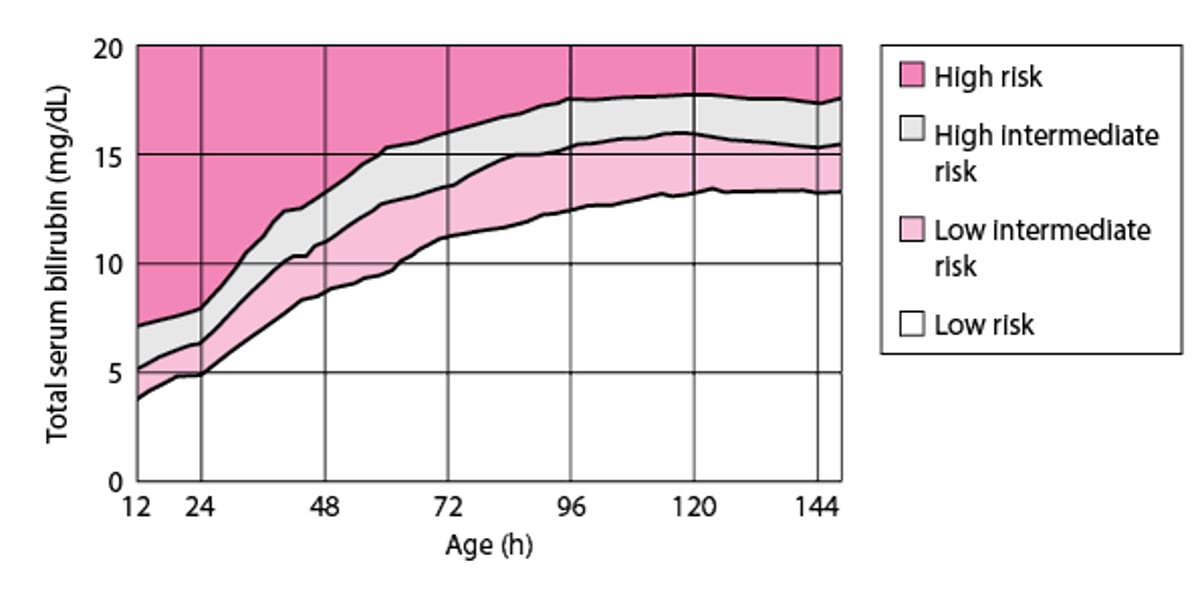
Among healthy term infants, the threshold for concern typically is considered to be a level > 18 mg/dL (> 308 micromol/L); see figure Risk of hyperbilirubinemia in neonates (1). However, infants who are premature, small for gestational age, and/or ill (eg, with sepsis, hypothermia, or hypoxia) are at greater risk and intervention may be done at lower levels. In such infants, although risk increases with increasing hyperbilirubinemia, there is no level of hyperbilirubinemia that is considered safe; treatment is given based on age and clinical factors. There are now suggested operational thresholds to initiate phototherapy based on gestational age.
Neurotoxicity is the major consequence of neonatal hyperbilirubinemia. An acute encephalopathy can be followed by a variety of neurologic impairments, including cerebral palsy and sensorimotor deficits; cognition is usually spared. Kernicterus
When serum bilirubin concentration is markedly elevated
Risk of hyperbilirubinemia in neonates
Risk is based on total serum bilirubin levels. (Adapted from Bhutani VK, Johnson L, Sivieri EM: Predictive ability of a predischarge hour-specific serum bilirubin for subsequent significant hyperbilirubinemia in healthy term and near-term newborns. Pediatrics 103(1):6–14, 1999. doi: 10.1542/peds.103.1.6) |

General reference
1. Maisels MJ, Bhutani VK, Bogen D, et al: Hyperbilirubinemia in the newborn infant ≥ 35 weeks gestation: An update with clarifications. Pediatrics 124(4):1193–1198, 2009. doi: 10.1542/peds.2009-0329
Pathophysiology of Neonatal Hyperbilirubinemia
Mechanisms of hyperbilirubinemia
Hyperbilirubinemia can be caused by one or more of the following processes:
Increased production
Decreased hepatic uptake
Decreased conjugation
Impaired excretion
Impaired bile flow (cholestasis)
Increased enterohepatic circulation
Etiology of Neonatal Hyperbilirubinemia
Classification
There are several ways to classify and discuss causes of hyperbilirubinemia. Because transient jaundice is common among healthy neonates (unlike adults, in whom jaundice always signifies a disorder), hyperbilirubinemia can be classified as physiologic or pathologic. It can be classified by whether the hyperbilirubinemia is unconjugated, conjugated, or both. It also can be classified by mechanism ( see Table: Causes of Neonatal Hyperbilirubinemia).
Causes
Most cases involve unconjugated hyperbilirubinemia. Some of the most common causes of neonatal jaundice include
Physiologic hyperbilirubinemia
Breastfeeding jaundice
Breast milk jaundice
Pathologic hyperbilirubinemia due to hemolytic disease
Liver dysfunction (eg, caused by parenteral alimentation causing cholestasis, neonatal sepsis, neonatal hepatitis) may cause a conjugated or mixed hyperbilirubinemia.
Physiologic hyperbilirubinemia occurs in almost all neonates. Shorter neonatal red blood cell life span increases bilirubin production, deficient conjugation due to the deficiency of uridine diphosphate-glucuronosyltransferase (UGT) decreases clearance, and low bacterial levels in the intestine combined with increased hydrolysis of conjugated bilirubin increase enterohepatic circulation. Bilirubin levels can rise up to 18 mg/dL (308 micromol/L) by 3 to 4 days of life (7 days in Asian infants) and fall thereafter.
Breastfeeding jaundice develops in one sixth of breastfed infants during the first week of life. Breastfeeding increases enterohepatic circulation of bilirubin in some infants who have decreased milk intake and who also have dehydration or low caloric intake. The increased enterohepatic circulation also may result from reduced intestinal bacteria that convert bilirubin to nonresorbed metabolites.
Breast milk jaundice is different from breastfeeding jaundice. It develops after the first 5 to 7 days of life and peaks at about 2 weeks. It is thought to be caused by an increased concentration of beta-glucuronidase in breast milk, causing an increase in the deconjugation and reabsorption of bilirubin.
Pathologic hyperbilirubinemia in term infants is diagnosed if
Jaundice appears in the first 24 hours, after the first week of life, or lasts > 2 weeks
Total serum bilirubin rises by > 5 mg/dL/day (> 86 micromol/L/day)
Total serum bilirubin is > 18 mg/dL (> 308 micromol/L/day)
Infant shows symptoms or signs of a serious illness
Some of the most common pathologic causes are
Immune and nonimmune hemolytic anemia
Hematoma resorption
Causes of Neonatal Hyperbilirubinemia
Mechanism | Causes |
|---|---|
Increased enterohepatic circulation | Breast milk (breast milk jaundice) Breastfeeding failure (breastfeeding jaundice) Fasting or other cause for hypoperistalsis Intestinal atresia or stenosis, including annular pancreas Meconium ileus or meconium plug syndrome Swallowed blood |
Overproduction | Breakdown of extravascular blood (eg, hematomas; petechiae; pulmonary, cerebral, or occult hemorrhage) Polycythemia due to maternofetal or fetofetal transfusion or delayed umbilical cord clamping |
Overproduction due to hemolytic anemia | Certain drugs and agents in neonates with G6PD deficiency Maternofetal blood group incompatibility (eg, Rh, ABO) Red blood cell enzyme deficiencies (eg, of G6PD or pyruvate kinase) |
Undersecretion due to biliary obstruction | Alpha-1 antitrypsin deficiency* Choledochal cyst* Cystic fibrosis* (inspissated bile) Dubin-Johnson syndrome and Rotor syndrome* Parenteral nutrition Tumor or band* (extrinsic obstruction) |
Undersecretion due to metabolic-endocrine conditions | Crigler-Najjar syndrome (familial nonhemolytic jaundice types 1 and 2) Drugs and hormones Hypermethioninemia Hypopituitarism and anencephaly Lucey-Driscoll syndrome Tyrosinosis |
Mixed overproduction and undersecretion | Asphyxia Intrauterine infections Severe erythroblastosis fetalis TORCH infections |
* Jaundice may also occur outside the neonatal period. | |
G6PD = glucose-6-phosphate dehydrogenase; TORCH =toxoplasmosis, other pathogens, rubella, cytomegalovirus, and herpes simplex. | |
Adapted from Poland RL, Ostrea EM Jr: Neonatal hyperbilirubinemia. In Care of the High-Risk Neonate, ed. 3, edited by MH Klaus and AA Fanaroff. Philadelphia, WB Saunders Company, 1986. | |
Evaluation of Neonatal Hyperbilirubinemia
History
History of present illness should note age of onset and duration of jaundice. Important associated symptoms include lethargy and poor feeding (suggesting possible kernicterus), which may progress to stupor, hypotonia, or seizures and eventually to hypertonia. Patterns of feeding can be suggestive of possible breastfeeding failure or underfeeding. Therefore, history should include what the infant is being fed, how much and how frequently, urine and stool production (possible breastfeeding failure or underfeeding), how well the infant is latching on to the breast or taking the nipple of the bottle, whether the mother feels that her milk has come in, and whether the infant is swallowing during feedings and seems satiated after feedings.
Review of systems should seek symptoms of causes, including respiratory distress, fever, and irritability or lethargy (sepsis); hypotonia and poor feeding (hypothyroidism, metabolic disorder); and repeated episodes of vomiting (intestinal obstruction).
Past medical history should focus on maternal infections (toxoplasmosis, other pathogens, rubella, cytomegalovirus, and herpes simplex [TORCH] infections), disorders that can cause early hyperbilirubinemia (maternal diabetes), maternal Rh factor and blood group (maternofetal blood group incompatibility), and a history of a prolonged or difficult birth (hematoma or forceps trauma).
Family history should note known inherited disorders that can cause jaundice, including glucose-6-phosphate dehydrogenase (G6PD) deficiency, or other red cell enzyme deficiencies, thalassemias, and spherocytosis, and also any history of siblings who have had jaundice.
Physical examination
Overall clinical appearance and vital signs are reviewed.
The skin is inspected for extent of jaundice. Gentle pressure on the skin can help reveal the presence of jaundice.
The physical examination should focus on signs of causative disorders.
The general appearance is inspected for plethora (maternofetal transfusion), macrosomia (maternal diabetes), and lethargy or extreme irritability (sepsis or infection) and for any dysmorphic features such as macroglossia (hypothyroidism) and flat nasal bridge or bilateral epicanthal folds (Down syndrome).
For the head and neck examination, any bruising and swelling of the scalp consistent with a cephalohematoma are noted. Lungs are examined for crackles (rales), rhonchi, and decreased breath sounds (pneumonia). The abdomen is examined for distention, mass (hepatosplenomegaly), or pain (intestinal obstruction). Neurologic examination should focus on signs of hypotonia or weakness (metabolic disorder, hypothyroidism, sepsis).
Red flags
The following findings are of particular concern:
Jaundice in the first day of life
Total serum bilirubin > 18 mg/dL (> 308 micromol/L)
Rate of rise of total serum bilirubin > 0.2 mg/dL/hour (> 3.4 micromol/L/hour) or > 5 mg/dL/day (> 86 micromol/L/day)
Conjugated bilirubin concentration > 1 mg/dL (> 17 micromol/L) if total serum bilirubin is < 5 mg/dL (< 86 micromol/L) or > 20% of total serum bilirubin (suggests neonatal cholestasis)
Jaundice after 2 weeks of age
Lethargy, irritability, respiratory distress
Interpretation of findings
Evaluation should focus on distinguishing physiologic from pathologic jaundice. History, physical examination, and timing can help, but typically total serum bilirubin and conjugated serum bilirubin levels are measured.
Timing
Jaundice that develops in the first 24 to 48 hours, or that persists > 2 weeks, is most likely pathologic. Jaundice that does not become evident until after 2 to 3 days is more consistent with physiologic, breastfeeding, or breast milk jaundice. An exception is undersecretion of bilirubin due to metabolic factors (eg, Crigler-Najjar syndrome, hypothyroidism, drugs), which may take 2 to 3 days to become evident. In such cases, bilirubin typically peaks in the first week, accumulates at a rate of < 5 mg/dL/day (< 86 micromol/L), and can remain evident for a prolonged period. Because most neonates are now discharged from the hospital or nursery within 48 hours, many cases of hyperbilirubinemia are detected only after discharge.
Physical Findings in Neonatal Jaundice
Findings | Timing of Jaundice | Cause |
|---|---|---|
General examination | ||
Fever, tachycardia, respiratory distress | First 24 hours Accumulates > 5 mg/dL/day (> 86 micromol/L/day) | |
Lethargy, hypotonia | May appear in the first 24–48 hours Can be prolonged (> 2 weeks) | Hypothyroidism, metabolic disorder |
Macrosomia | 24–48 hours Can accumulate > 5 mg/dL (> 86 micromol/L) | |
Petechiae | First 24 hours Accumulates > 5 mg/dL (> 86 micromol/L) | Hemolytic states (eg, maternofetal blood group incompatibility, red blood cell enzyme deficiencies, hereditary spherocytosis, thalassemias, sepsis) |
Plethora | First 24 hours Accumulates > 5 mg/dL (> 86 micromol/L) | Maternofetal or fetofetal transfusion, delayed umbilical cord clamping |
Head and neck examination | ||
Bilateral slanting palpebral fissures, flat nasal bridge, macroglossia, flattened occiput | First 2–3 days | |
Cephalohematoma | 24–48 hours Can accumulate > 5 mg/dL (> 86 micromol/L) | |
Macroglossia | 24–48 hours Can be prolonged (> 2 weeks) | |
Abdominal examination | ||
Abdominal distention, decreased bowel sounds | Possible delayed manifestation (2–3 days or later) | Intestinal obstruction (eg, cystic fibrosis, Hirschsprung disease, intestinal atresia or stenosis, pyloric stenosis, biliary atresia) |
TORCH =toxoplasmosis, other pathogens, rubella, cytomegalovirus, and herpes simplex. | ||
Testing
Diagnosis of hyperbilirubinemia is suspected by the infant’s color and is confirmed by measurement of serum bilirubin. Noninvasive techniques for measuring bilirubin in infants, including transcutaneous and digital photography–based techniques, are being used increasingly and correlate well with serum bilirubin measurements. Risk of hyperbilirubinemia is based on age-specific total serum bilirubin levels.
A bilirubin concentration > 10 mg/dL (> 171 micromol/L) in preterm infants or > 18 mg/dL (> 308 micromol/L) in term infants warrants additional testing, including hematocrit, blood smear, reticulocyte count, direct Coombs test, total serum bilirubin and direct serum bilirubin concentrations, and blood type and Rh group of the infant and mother.
Other tests, such as blood, urine, and cerebrospinal fluid cultures to detect sepsis and measurement of red blood cell enzyme levels to detect unusual causes of hemolysis, may be indicated by the history and physical examination. Such tests also may be indicated for any neonates with an initial bilirubin level > 25 mg/dL (> 428 micromol/L).
Treatment of Neonatal Hyperbilirubinemia
Treatment of hyperbilirubinemia is directed at the underlying disorder. In addition, treatment for hyperbilirubinemia itself may be necessary.
Physiologic jaundice usually is not clinically significant and resolves within 1 week. Frequent formula feedings can reduce the incidence and severity of hyperbilirubinemia by increasing gastrointestinal motility and frequency of stools, thereby minimizing the enterohepatic circulation of bilirubin. The type of formula does not seem important in increasing bilirubin excretion.
Breastfeeding jaundice may be prevented or reduced by increasing the frequency of feedings. If the bilirubin level continues to increase > 18 mg/dL (>
Definitive treatment of hyperbilirubinemia involves
Phototherapy
Exchange transfusion

Phototherapy
This treatment remains the standard of care, most commonly using fluorescent white light. (Blue light, wavelength 425 to 475 nm, is most effective for intensive phototherapy.) Phototherapy is the use of light to photoisomerize unconjugated bilirubin into forms that are more water-soluble and can be excreted rapidly by the liver and kidney without glucuronidation. It provides definitive treatment of neonatal hyperbilirubinemia and prevention of kernicterus. (See also the American Academy of Pediatrics' technical report on using phototherapy to prevent severe neonatal hyperbilirubinemia in neonates who are ≥ 35 weeks gestation.)
For neonates born at ≥ 35 weeks gestation, phototherapy is an option when unconjugated bilirubin is > 12 mg/dL (> 205.2 micromol/L) and may be indicated when unconjugated bilirubin is > 15 mg/dL (257 micromol/L) at 25 to 48 hours, 18 mg/dL (308 micromol/L) at 49 to 72 hours, and 20 mg/dL (342 micromol/L) at > 72 hours ( see Figure: Risk of hyperbilirubinemia in neonates). Phototherapy is not indicated for conjugated hyperbilirubinemia.
For neonates born at < 35 weeks gestation, threshold bilirubin levels for treatment are lower because premature infants are at a greater risk of neurotoxicity. The more preterm the infant, the lower the threshold ( see Table: Suggested Thresholds* for Starting Phototherapy or Exchange Transfusion in Infants < 35 Weeks Gestation).
Suggested Thresholds* for Starting Phototherapy or Exchange Transfusion in Infants < 35 Weeks Gestation
Gestational Age (weeks) | Phototherapy (total serum bilirubin, mg/dL [micromol/L]) | Exchange Transfusion (total serum bilirubin, mg/dL [micromol/L]) |
|---|---|---|
< 28 | 5–6 [86–103] | 11–14 [188–239] |
28 to < 30 | 6–8 [103–137] | 12–14 [205–239] |
30 to < 32 | 8–10 [137–171] | 13–16 [222–274] |
32 to < 34 | 10–12 [171–205] | 15–18 [257–308] |
34 to < 35 | 12–14 [205–239] | 17–19 [291–325] |
* Consensus-based recommendations adapted from Maisels MJ, Watchko JF, Bhutani VK, Stevenson DK: An approach to the management of hyperbilirubinemia in the preterm infant less than 35 weeks of gestation. J Perinatol 32:660–664, 2012. doi: 10.1038/jp.2012.71 | ||
Because visible jaundice may disappear during phototherapy even though serum bilirubin remains elevated, skin color cannot be used to evaluate jaundice severity. Blood taken for bilirubin determinations should be shielded from bright light, because bilirubin in the collection tubes may rapidly photo-oxidize.
Exchange transfusion
This treatment can rapidly remove bilirubin from circulation and is indicated for severe hyperbilirubinemia, which most often occurs with immune-mediated hemolysis. Small amounts of blood are withdrawn and replaced through an umbilical vein catheter, or other access as available, to remove partially hemolyzed and antibody-coated red blood cells (RBCs) as well as circulating immunoglobulins. The blood is replaced with uncoated donor RBCs that do not have the RBC membrane antigen that binds the circulating antibodies. That is, type O blood is used if the neonate is sensitized to AB antigens and Rh-negative blood is used if the neonate is sensitized to Rh antigen. Because adult donor RBCs have more ABO antigen sites than fetal cells, type-specific transfusion will intensify the hemolysis. Only unconjugated hyperbilirubinemia can cause kernicterus, so if conjugated bilirubin is elevated, the level of unconjugated rather than total bilirubin is used to determine the need for exchange transfusion.
For term infants, specific indications are serum bilirubin ≥ 20 mg/dL (≥ 342 micromol/L) at 24 to 48 hours or ≥ 25 mg/dL (≥ 428 micromol/L) at > 48 hours and failure of phototherapy to result in a 1- to 2-mg/dL (17- to 34-micromol/L) decrease within 4 to 6 hours of initiation or at the first clinical signs of kernicterus regardless of bilirubin levels. If the serum bilirubin level is > 25 mg/dL (≥ 428 micromol/L) when the neonate is initially examined, preparation for an exchange transfusion should be made in case intensive phototherapy fails to lower the bilirubin level.
Thresholds have been suggested for neonates born at < 35 weeks gestation (see table Suggested Thresholds* for Starting Phototherapy or Exchange Transfusion in Infants 35 Weeks Gestation). Previously, some clinicians used criteria based solely on patient weight, but these criteria have been replaced by the more specific guidelines described above.
Most often, 160 mL/kg (twice the infant’s total blood volume) of packed RBCs is exchanged over 2 to 4 hours; an alternative is to give 2 successive exchanges of 80 mL/kg each over 1 to 2 hours. To do an exchange, a volume of blood is withdrawn and then immediately replaced by transfused blood. The volume of each can vary depending on the infant's size, but volumes are typically near 20 mL for the average term infant. This procedure is repeated until the total desired volume is exchanged. For critically ill or premature infants, aliquots of 5 to 10 mL are used to avoid sudden major changes in blood volume. The goal is to reduce bilirubin by nearly 50%, with the knowledge that hyperbilirubinemia may rebound to about 60% of pretransfusion level within 1 to 2 hours. It is also customary to lower the target level by 1 to 2 mg/dL (17 to 34 micromol/L) in conditions that increase the risk of kernicterus (eg, fasting, sepsis, acidosis). Exchange transfusions may need to be repeated if bilirubin levels remain high. Finally, there are risks and complications with the procedure, and the success of phototherapy has reduced the frequency of exchange transfusion.
Key Points
Neonatal jaundice is caused by increased bilirubin production, decreased bilirubin clearance, or increased enterohepatic circulation.
Some jaundice is normal in neonates.
Risk varies with postnatal age, total serum bilirubin value, prematurity, and health of the neonate.
Treatment depends on cause and degree of bilirubin elevation; the more preterm the infant, the lower the threshold level for treatment.
Definitive treatments include phototherapy and exchange transfusion.
More Information
The following is an English-language resource that may be useful. Please note that THE MANUAL is not responsible for the content of this resource.
American Academy of Pediatrics technical report: Using phototherapy to prevent severe neonatal hyperbilirubinemia in neonates who are ≥ 35 weeks gestation







