


Onchocerciasis is a filarial nematode infection with Onchocerca volvulus. Blackflies (Simulium
(See also Approach to Parasitic Infections and Overview of Filarial Nematode Infections.)
An estimated 21 million people are infected with onchocerciasis worldwide; about 14.6 million have skin disease and 1.15 million have visual impairment or loss. Onchocerciasis is the 2nd leading cause of infectious blindness worldwide (after trachoma).
Onchocerciasis is most common in tropical and sub-Saharan regions of Africa. Small foci exist in Yemen and along the Venezuelan border with the Brazilian Amazon. Blindness due to onchocerciasis is fairly rare in the Americas; Colombia, Ecuador, Mexico, and Guatemala have been declared free of onchocerciasis by the World Health Organization (WHO). People who live or work near rapidly flowing streams or rivers are the most likely to be infected. In addition to residents, longterm travelers (eg, missionaries, aid workers, field researchers) are at risk.
Pathophysiology of Onchocerciasis
Onchocerciasis is spread by blackflies (Simulium species) that breed in swiftly flowing streams (hence, the term river blindness). Many blackfly bites are needed before disease develops.
Infective larvae inoculated into the skin during the bite of a blackfly develop into adult worms in 12 to 18 months. Adult female worms may live up to 15 years in subcutaneous nodules. Females are 33 to 50 cm long; males are 19 to 42 mm long. Mature female worms produce microfilariae that migrate mainly through the skin and invade the eyes.

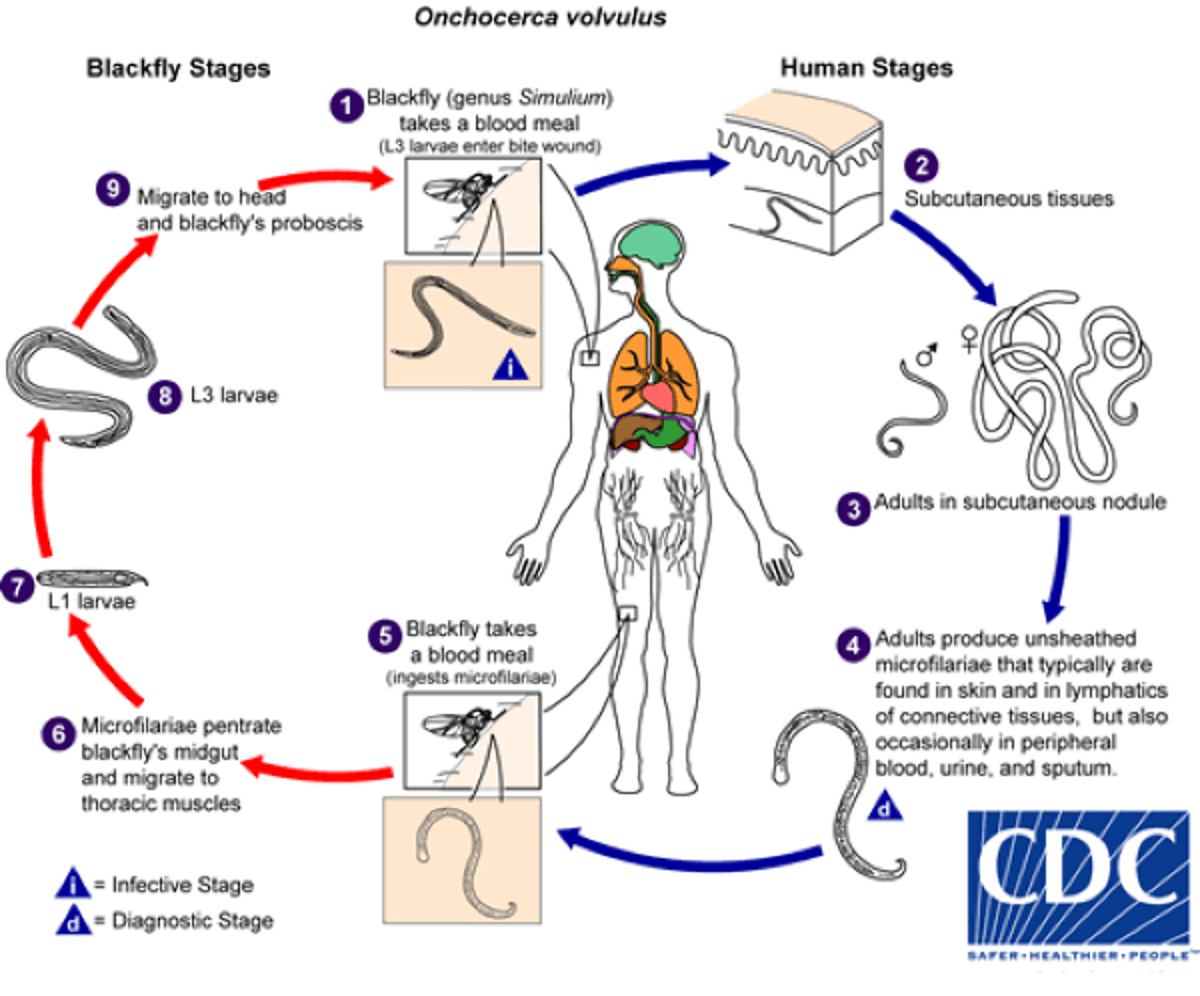
Image from the Centers of Disease Control and Prevention, Global Health, Division of Parasitic Diseases and Malaria.
Symptoms and Signs of Onchocerciasis
Onchocerciasis typically affects
Skin (nodules, dermatitis)
Eyes
Nodules
The subcutaneous (or deeper) nodules (onchocercoma) that contain adult worms may be visible or palpable but are otherwise asymptomatic. They are composed of inflammatory cells and fibrotic tissue in various proportions. Old nodules may caseate or calcify.
Patients may have enlargement of inguinal, femoral, or other lymph nodes. Localized swelling of the genitalia and inguinal hernias can develop.
Skin disease
Onchocercal dermatitis is caused by the microfilarial stage of the parasite. Intense pruritus may be the only symptom in lightly infected people.
Skin lesions usually consist of a nondescript maculopapular rash with secondary excoriations, scaling ulcerations and lichenification, and mild to moderate lymphadenopathy. Other skin abnormalities can include premature wrinkling, atrophy, patchy hypopigmentation, and loss of elasticity. In severe cases, patients may develop folds of atrophic skin in the lower abdomen and upper medial thighs ("hanging groin").
Onchocercal dermatitis is generalized in most patients, but a localized and sharply delineated form of eczematous dermatitis with hyperkeratosis, scaling, and pigment changes (Sowdah) is common in Yemen and Sudan.
Eye disease
Ocular involvement ranges from mild visual impairment to complete blindness. Lesions of the anterior portion of the eye include
Punctate (snowflake) keratitis (an acute inflammatory infiltrate surrounding dying microfilariae that resolves without causing permanent damage)
Sclerosing keratitis (an ingrowth of fibrovascular scar tissue that may cause subluxation of the lens and blindness)
Anterior uveitis or iridocyclitis (which may deform the pupil)
Chorioretinitis, optic neuritis, and optic atrophy may also occur.

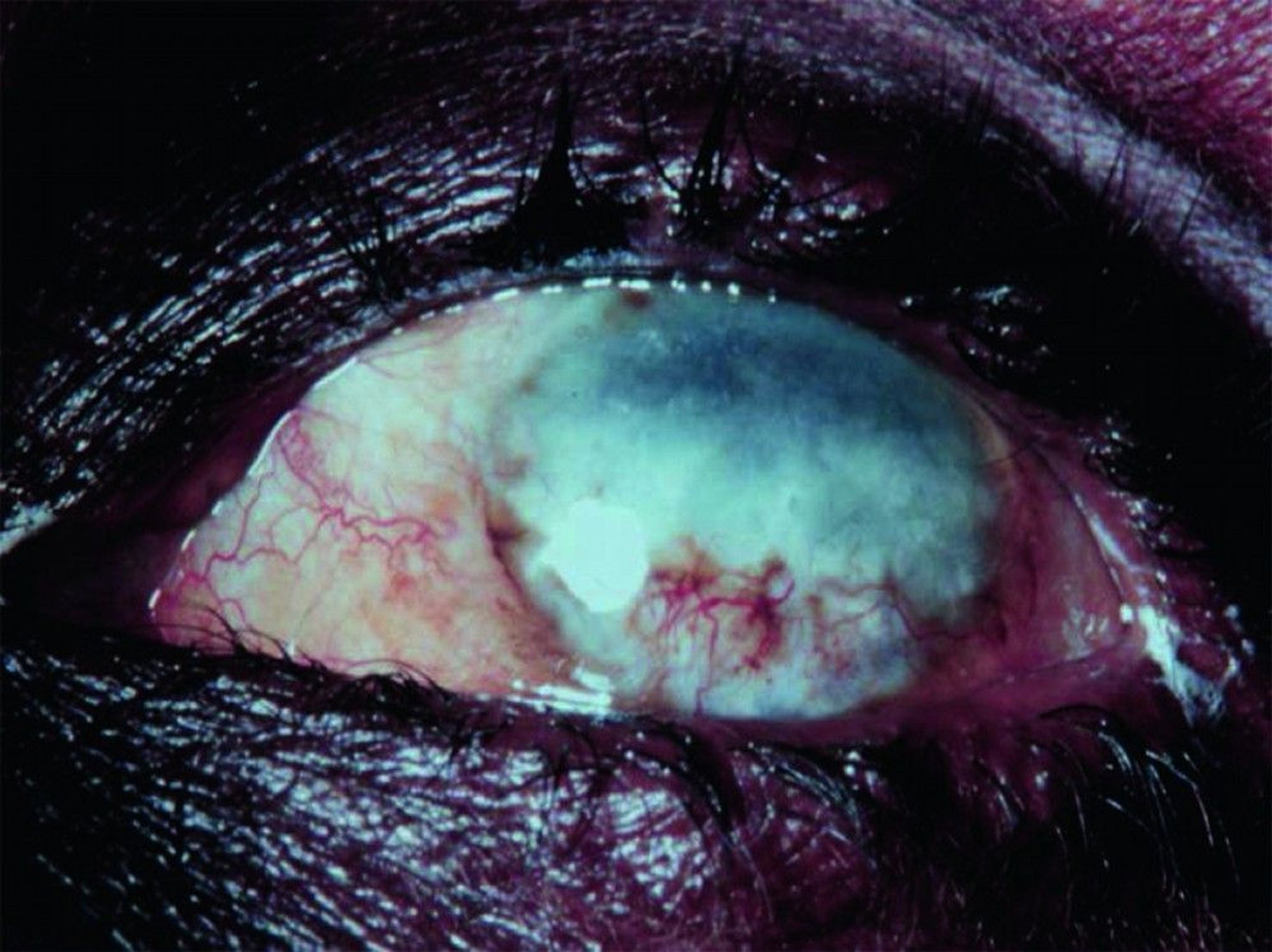
© Springer Science+Business Media
Diagnosis of Onchocerciasis
Microscopic examination of skin snips or biopsies
Slit-lamp examination of the cornea and anterior chamber of the eye
Demonstration of microfilariae in skin snips or biopsies is the traditional diagnostic method for onchocerciasis; multiple samples are usually taken (see table Collecting and Handling Specimens for Microscopic Diagnosis of Parasitic Infections). PCR-based methods to detect parasite DNA in skin samples are more sensitive than standard techniques but are available only in research settings.
Microfilariae may also be visible in the cornea and anterior chamber of the eye during slit-lamp examination.
Antibody detection is of limited value; there is substantial antigenic cross-reactivity among O. volvulus and other filaria and different helminths, and a positive serologic test does not distinguish between past and current infection.
Palpable nodules (or deep nodules detected by ultrasonography or MRI) can be excised and examined for adult worms, but this procedure is rarely necessary.
Treatment of Onchocerciasis
Loa loaLoa loa coinfections.
Pearls & Pitfalls
|
Wolbachia, which O. volvulus
Prevention of Onchocerciasis
No drug has been shown to protect against infection with O. volvulusSimuliumOnchocerciasis Control ProgrammeWHO: Onchocerciasis).
Simulium bites can be minimized by avoiding fly-infested areas, by wearing protective clothing, and possibly by liberally applying insect repellents.
Key Points
Onchocerciasis is a filarial infection that causes skin lesions, rash, and, more importantly, eye disease, leading to visual impairment and sometimes blindness.
Diagnose by slit-lamp examination of the eye and microscopic examination of a skin snip; where available, polymerase chain reaction (PCR) testing may be helpful.
Loa loa if they have been in areas of central Africa where both parasites are transmitted.







