

Pelvic organ prolapse results from laxities (similar to hernias) in the ligaments, fascia, and muscles supporting the pelvic organs (pelvic floor—see figure ). Pelvic organ prolapse is a common gynecologic issue. Prevalence is difficult to determine, and reported rates vary (in one study of 8,000 women, 8.3% reported symptomatic prolapse) (1). Treatment is based on symptoms.
Pelvic organ prolapse affects various anatomic structures of the female reproductive tract and pelvic floor, and includes
Anterior vaginal wall prolapse
Posterior vaginal wall prolapse
Apical prolapse (vaginal vault prolapse)
Uterine prolapse
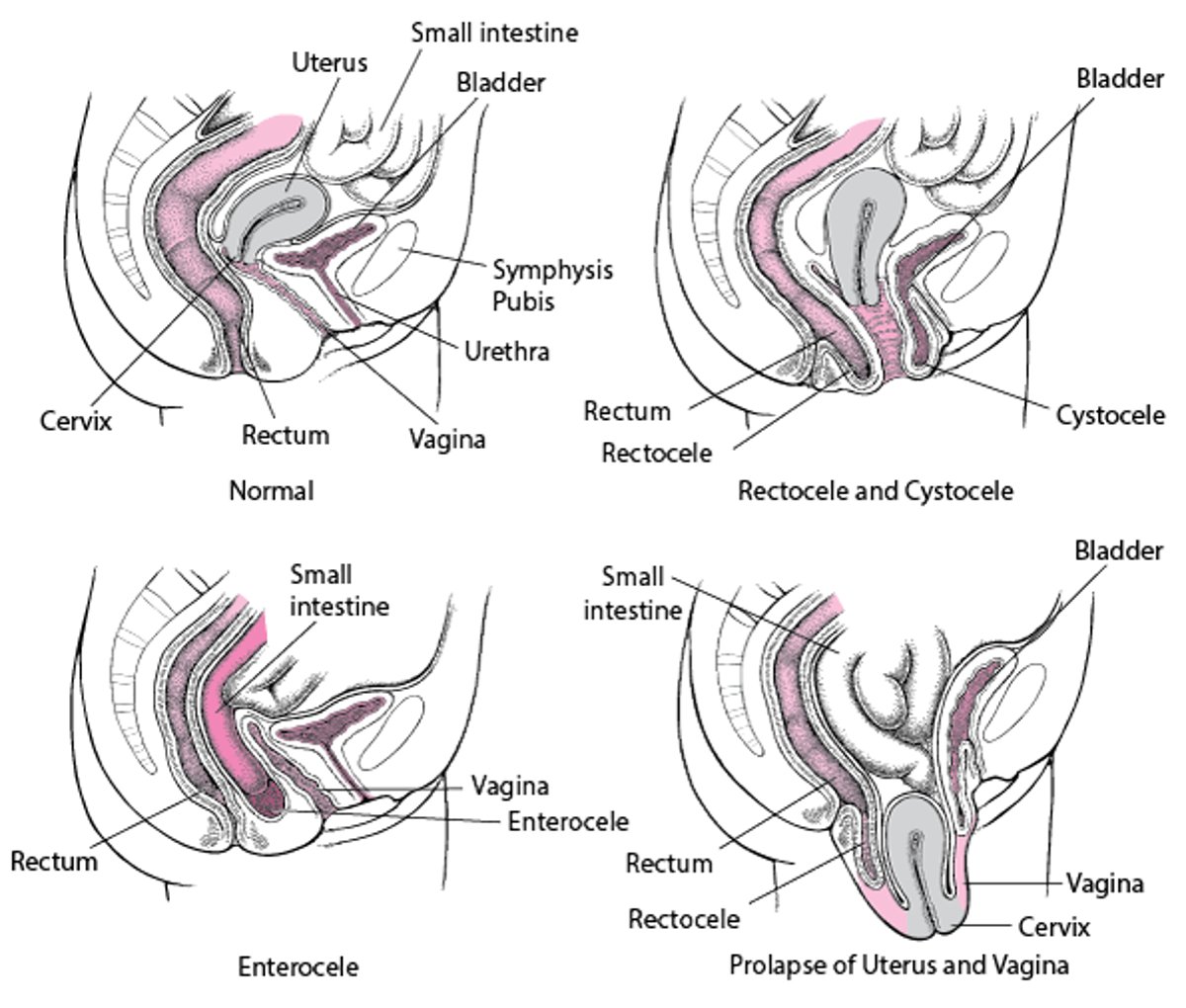
Prolapse of the vaginal wall allows surrounding organs to protrude into the vagina; commonly used terms include cystocele, urethrocele, enterocele, and rectocele, depending on the organ. Procidentia is collapse of the anterior and posterior vaginal walls and apical prolapse. Usually, prolapse involves multiple sites.
Pelvic Organ Prolapse

Risk Factors for Pelvic Organ Prolapse
Common risk factors include (2)
Parity; additional obstetric history risk factors include prolonged second stage of labor, vaginal delivery, operative vaginal delivery, and high-birthweight infant
Obesity
Increasing age
Injury (eg, due to pelvic surgery)
Chronic increased intraabdominal pressure (ie, due to constipation, lifting heavy items, chronic respiratory disorders)
Less common risk factors include sacral nerve disorders and connective tissue disorders.
Staging of Pelvic Organ Prolapse
Severity of pelvic organ prolapse can be staged by the Pelvic Organ Prolapse-Quantification (POP-Q) system (3):
Stage 0: No prolapse
Stage I: Most distal prolapse is more than 1 cm above the hymen
Stage II: Most distal prolapse is between 1 cm above and 1 cm below the hymen
Stage III: Most distal prolapse is more than 1 cm below hymen but 2 cm shorter than total vaginal length
Stage IV: Complete eversion
The POP-Q system is recommended by professional organizations because it is a reliable and reproducible classification system that is based on predefined anatomic landmarks (4).
The Baden-Walker system, which is based on level of protrusion, is no longer commonly used because it is imprecise and not reproducible.
References
1. Tegerstedt G, Maehle-Schmidt M, Nyrén O, Hammarström M: Prevalence of symptomatic pelvic organ prolapse in a Swedish population. Int Urogynecol J Pelvic Floor Dysfunct. 2005;16(6):497-503. doi:10.1007/s00192-005-1326-1
2. Vergeldt TF, Weemhoff M, IntHout J, Kluivers KB: Risk factors for pelvic organ prolapse and its recurrence: a systematic review. Int Urogynecol J. 2015;26(11):1559-1573. doi:10.1007/s00192-015-2695-8
3. Bump RC, Mattiasson A, Bø K, et al. The standardization of terminology of female pelvic organ prolapse and pelvic floor dysfunction. Am J Obstet Gynecol. 1996;175(1):10-17. doi:10.1016/s0002-9378(96)70243-0
4. Pelvic Organ Prolapse: ACOG Practice Bulletin, Number 214. Obstet Gynecol. 2019 (reaffirmed 2024);134(5):e126-e142. doi:10.1097/AOG.0000000000003519





