

In benign paroxysmal positional vertigo, short (< 60 seconds) episodes of vertigo occur with certain head positions without associated hearing loss. Nausea and nystagmus develop. Diagnosis is primarily clinical. Treatment involves canalith repositioning maneuvers. Medications and surgery are rarely, if ever, indicated.
Benign paroxysmal positional vertigo (BPPV) is the most common cause of relapsing otogenic vertigo. The lifetime prevalence of BPPV in a population-based survey in Germany was 2.4% (1). It is characterized by a female preponderance. It affects people increasingly as they age and can severely affect balance in older adults, leading to potentially injurious falls.
Reference
1. von Brevern M, Radtke A, Lezius F, et al. Epidemiology of benign paroxysmal positional vertigo: a population based study. J Neurol Neurosurg Psychiatry. 2007;78(7):710-715. doi:10.1136/jnnp.2006.100420
Etiology of Benign Paroxysmal Positional Vertigo
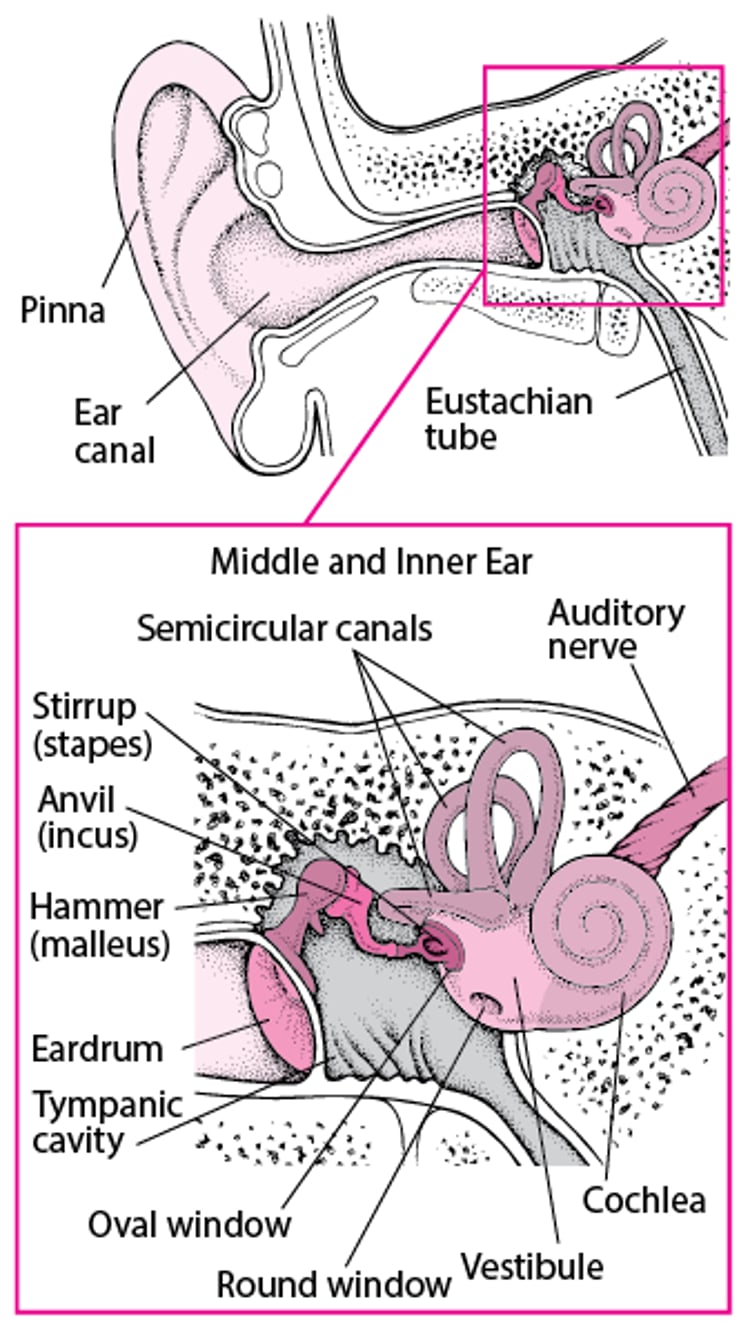
BPPV is thought to be caused by the displacement of otoconial crystals (calcium carbonate crystals normally embedded in the saccule and utricle) into the semicircular canals, a process called canalithiasis. These displaced crystals, which are also called canaliths, stimulate hair cells most commonly in the posterior semicircular canal, occasionally in the lateral semicircular canal, and rarely in the superior semicircular canal; this process creates the illusion of motion for the patient. Physiologic processes occurring during aging can lead to the fragmentation of otoconia, which can then dislodge and migrate into the semicircular canals (1).
Risk factors include the following:
Spontaneous degeneration of the utricular otolithic membranes
Labyrinthine concussion
Ear surgery
Recent viral infection (eg, viral neuronitis)
Head trauma
Prolonged immobilization (anesthesia or bed rest)
Previous vestibular disorders (eg, Meniere disease)
Occlusion of the anterior vestibular artery
Giant cell arteritis (2)
Osteoporosis (3)
Components of metabolic syndrome (hypertension, diabetes mellitus, and hyperlipidemia) (4)
Inside the Ear

Etiology references
1. Parham K, Kuchel GA. A Geriatric Perspective on Benign Paroxysmal Positional Vertigo. J Am Geriatr Soc. 2016;64(2):378-385. doi:10.1111/jgs.13926
2. Amor-Dorado JC, Llorca J, Costa-Ribas C, Garcia-Porrua C, Gonzalez-Gay MA. Giant cell arteritis: a new association with benign paroxysmal positional vertigo. Laryngoscope. 2004;114(8):1420-1425. doi:10.1097/00005537-200408000-00020
3. Byun H, Chung JH, Lee SH, Park CW, Kim EM, Kim I. Increased risk of benign paroxysmal positional vertigo in osteoporosis: a nationwide population-based cohort study. Sci Rep. 2019;9(1):3469. Published 2019 Mar 5. doi:10.1038/s41598-019-39830-x
4. Chen J, Zhang S, Cui K, Liu C. Risk factors for benign paroxysmal positional vertigo recurrence: a systematic review and meta-analysis. J Neurol. 2021;268(11):4117-4127. doi:10.1007/s00415-020-10175-0
Symptoms and Signs of Benign Paroxysmal Positional Vertigo
Patients with BPPV typically report a brief spinning or a rotational sensation with head movement. Nausea and vomiting may occur, but hearing loss and tinnitus are absent. Vertigo is triggered when the patient’s head moves (eg, when rolling over in bed or bending over to pick up something). Acute paroxysms of vertigo last only a few seconds to minutes; episodes tend to peak in the morning and abate throughout the day. However, episodes may recur for weeks or even months; some cases may then spontaneously resolve.
Diagnosis of Benign Paroxysmal Positional Vertigo
Primarily history and physical examination
Sometimes gadolinium-enhanced MRI if findings suggest central nervous system (CNS) lesion
The diagnosis of BPPV is based on characteristic symptoms, nystagmus elicited by the Dix-Hallpike maneuver (also called the Barany maneuver), and the absence of other abnormalities noted during neurologic examination (1). Such patients require no further testing. Audiometry is usually normal.
In the Dix-Hallpike (a provocative test for positional nystagmus), the following occur:
The patient sits erect on an examination table so that when the patient lies back, the head extends beyond the end of the examination table.
With support, the patient is rapidly lowered to a horizontal position, and the head is extended back 45° below horizontal and rotated 45° to the left.
The patient is told to fixate the eyes on a single location; visual fixation can shorten or even abolish nystagmus, so the maneuver is ideally done with the person wearing Frenzel lenses to make visual fixation on anything impossible.
The patient is returned to an upright position, and the maneuver is repeated with rotation to the right.
Vertigo and nystagmus can take about 5 to 10 seconds (sometimes up to 30 seconds) to appear (latency). Symptoms last 10 to 30 seconds, then decrease and disappear (ie, fatigue).
The duration of nystagmus and development of vertigo are noted. Nystagmus is torsional and occurs when the head is turned to the affected ear. Any position or maneuver that causes nystagmus should be repeated to see whether the nystagmus fatigues.
Unlike the positional nystagmus caused by BPPV, positional nystagmus caused by a CNS lesion has the following characteristics:
Lacks latency, fatigability, and severe subjective sensation
May continue for as long as the position is maintained
May be vertical or change direction
If rotary, is likely to be in an unexpected direction
In general, clinicians should not obtain imaging in patients who meet diagnostic criteria for BPPV in the absence of additional signs and/or symptoms inconsistent with BPPV that warrant imaging. If patients have nystagmus suggesting a CNS lesion, gadolinium-enhanced MRI of the brain and internal auditory canal is performed.
Diagnosis reference
1. Bhattacharyya N, Gubbels SP, Schwartz SR, et al. Clinical Practice Guideline: Benign Paroxysmal Positional Vertigo (Update). Otolaryngol Head Neck Surg. 017;156(3_suppl):S1-S47. doi:10.1177/0194599816689667
Treatment of Benign Paroxysmal Positional Vertigo
Provocative maneuvers to fatigue symptoms
Canalith repositioning maneuvers
BPPV is usually self-limited, and subsides spontaneously in several weeks or months. Medications (such as those used in Meniere disease) are not routinely recommended (1). Often, the adverse effects of medications may worsen dysequilibrium. Rarely, patients with severe symptoms can be treated with benzodiazepines or antihistamines until definitive repositioning can be performed. In these cases, it is important to consider other diagnoses and that medications suppress nystagmus elicited by Dix-Hallpike, making definitive diagnosis more difficult.
Because BPPV is fatigable, one therapeutic approach is to have the patient perform provocative maneuvers early in the day in a safe environment. Symptoms are then usually minimal for the rest of the day.
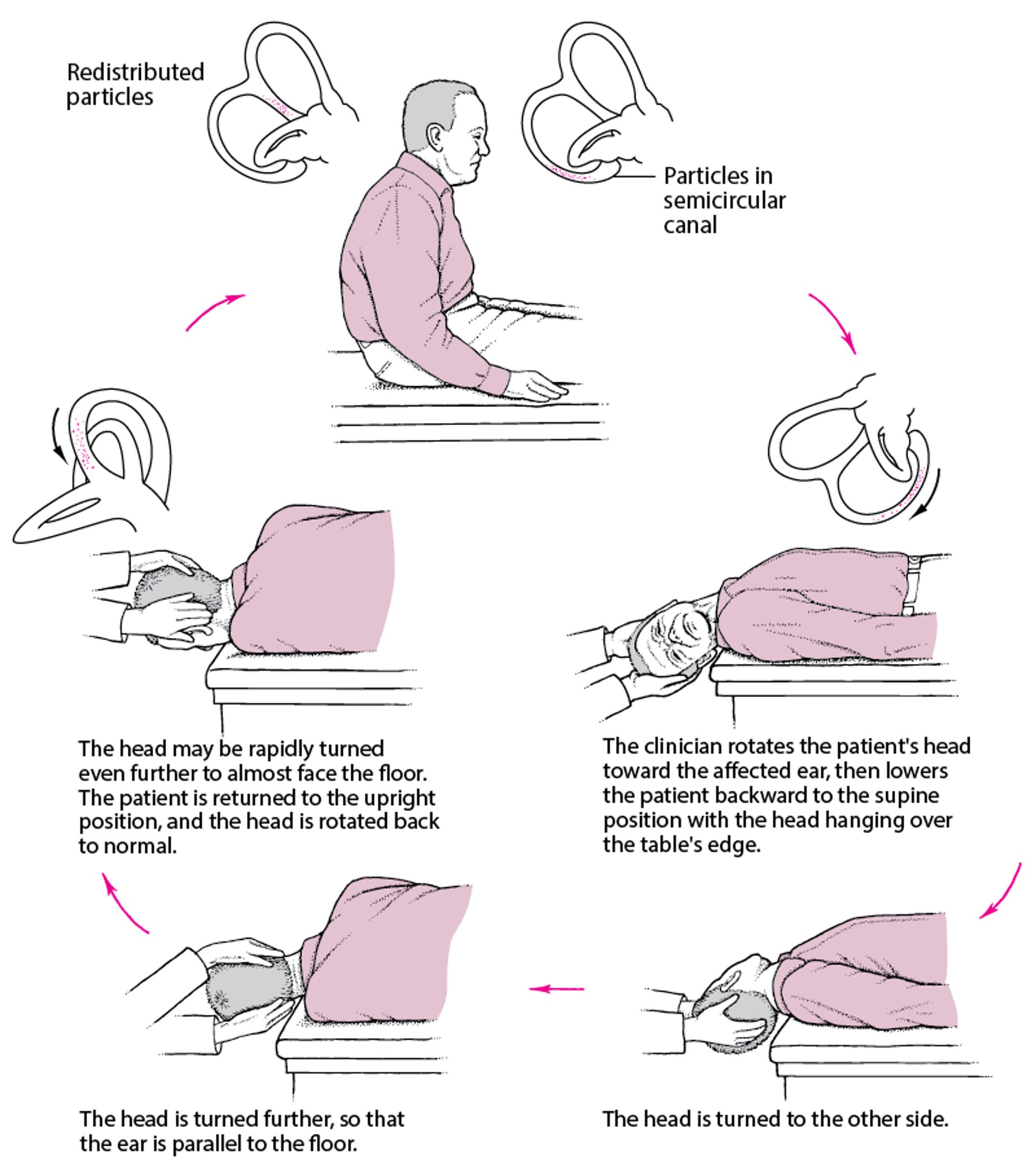
Canalith-repositioning maneuvers (most commonly the Epley maneuver or, less commonly, the Semont maneuver, or Brandt-Daroff exercises) involve moving the head through a series of specific positions intended to return the errant canalith to the utricle. After the Epley or Semont maneuver is done, the patient should try to avoid neck flexion or extension for 1 to 2 days. These maneuvers can be repeated as necessary. All of these maneuvers can be done by the patient at home.
Epley Maneuver: A Simple Treatment for a Common Cause of Vertigo
The maneuver is done by following the clockwise order of the red arrows below. |

For the Semont maneuver, the patient is seated upright in the middle of an examination table. The patient’s head is rotated toward the unaffected ear; this rotation is maintained throughout the maneuver. Next, the torso is lowered laterally onto the examination table so that the patient is lying on the side of the affected ear with the nose pointed up. After at least 30 seconds in this position, the patient is quickly moved through the upright position without straightening the head and is lowered laterally to the other side, now with the nose pointed down. After at least 30 seconds in this position, the patient is slowly returned to the upright position, and the head is rotated back to normal.
The Brandt-Daroff exercise can be taught to the patient. The patient sits upright, then lies on one side with the nose pointed up at a 45-degree angle. The patient remains in this position for about 30 seconds or until the vertigo subsides and then moves back to the seated position. The same motion is repeated on the opposite side. This cycle is repeated 5 times in a row, 3 times/day, for about 2 weeks, or until there is no more vertigo with the exercise.
Treatment reference
1. Bhattacharyya N, Gubbels SP, Schwartz SR, et al. Clinical Practice Guideline: Benign Paroxysmal Positional Vertigo (Update). Otolaryngol Head Neck Surg. 017;156(3_suppl):S1-S47. doi:10.1177/0194599816689667
Key Points
In BPPV, vertigo is caused by displacement of otoconial crystals into a semicircular canal; symptoms are triggered by head movement.
Nausea and vomiting may also occur, but not tinnitus or hearing loss.
Diagnosis is primarily clinical, but some patients require MRI to exclude other conditions.
Treat with canalith-repositioning maneuvers.
Medications rarely help and may worsen dysequilibrium symptoms.





